Lichen planopilaris
Lichen planopilaris
the follicular hyperkeratosis is constantly present in the central part of the bald patches.9,27 Histologically, the dermal–epidermal interface change in discoid lupus erythematosus is usually pronounced and of vacuolar type, whereas in lichen planopilaris lichenoid features (i.e., a more bandlike inflammatory cell infiltrate) predominate around the hair follicle. Additional histologic features that help in the diagnosis of lupus erythematosus are the more prominent perivascular infiltrate, the presence of dermal mucin, and plasma cells.28
Lichen planopilaris includes several variants with similar clinical, histopathological, and immunohistopathological features: classic lichen planopilaris, frontal fibrosing alopecia, fibrosing alopecia in a pattern distribution, and Graham-Little syndrome.
Clinical features Classic lichen planopilaris Classic lichen planopilaris is a very common form of scarring alopecia first described by Pringle in 1895.1 It is characterized by a variable clinical course resulting in patchy areas of hair loss accompanied by follicular inflammation. It is more frequent in women (70%) and has an average age of onset of 51 years.2 It has occasionally been reported in children.3 Approximately 50% of the patients have typical lesions of lichen planus elsewhere on the skin at one time or another.2 Typical lichen planus associated with lichen planopilaris of the scalp is rarely observed.4 However, involvement of the nails and oral/vulval mucosae may also be seen.5,6
The histologic diagnosis distinction from pseudopélade of Brocq is based on the absence of marked inflammation, significant follicular plugging, thickened basement membrane, and basal vacuolar degeneration in lupus erythematosus. Pseudopélade of Brocq is characterized by white-ivory colored patches of alopecia limited to the scalp, with a ‘footprints in the snow’ appearance.29
In histopathologically inconclusive cases, direct immunofluorescence is an important tool in the differential diagnosis of discoid lupus erythematosus.30 A positive lupus band test is seen in up to 83% of cases and
Common clinical symptoms include itching, scaling, tenderness, and burning sensation. Physical examination shows variable changes depending on the stage of clinical evolution. The lesions may be single or multiple and usually involve the parietal and vertex areas of the scalp. In general, the findings result from a mixture of inflammatory changes and scarring. The inflammation is characterized by follicular keratotic papules, scaling, and perifollicular erythema (see Fig. 22.110). The scarring results in hair loss with dilated follicular ostia containing keratotic debris (Fig. 22.132). Several hair shafts may emerge through these dilated ostia, generally in a number lower than 3.7 If examination of the scalp is performed at a late stage of the disease, overlap with other scarring alopecias is common, particularly pseudopélade of Brocq. The resemblance is such that some authors claim that these two entities represent the same illness.8
1097 Scarring alopecias
In the active stages, the hair-pull and hair-pluck tests show an increase in the number of anagen hairs.9 The most useful laboratory tests other than biopsy include direct immunofluorescence and antibody screening to exclude discoid and SLE.
Occasionally, lichen planopilaris may present in areas such as the extremities, trunk, and vulva, without involvement of the scalp.10,11 Exceptionally, a facial and truncal linear distribution has been documented, following Blaschko lines.12,13 Another variant of lichen planus that may affect the adnexal structures is lichen planus poritis (lichen planus of the eccrine glands), which involves the acrosyringium and proximal eccrine ducts in the superficial part of the dermis.14
studies and the phenomenon of easy plucking of the hair in the more active lesions of the disease.
Lichen planopilaris is considered a true trichologic emergency in which treatment should be instituted promptly to avoid irreversible hair loss. In this context, the biopsy is an essential component of the diagnostic work-up.36,37 It is very important to take an adequate biopsy from an active lesion, preferably from an area that is erythematous and scaly and in which there are still hair follicles that could be easily plucked, with anagen-like hair roots.9 This affords the best opportunity of identifying the diagnostic features. A biopsy of a nonactive or burned-out area usually does not offer much information and leads to a diagnosis of end-stage scarring alopecia of undetermined etiology.
Lichen planopilaris has been associated with exposure to gold, autoimmune thyroiditis, psoriasis, scleroderma en coup de sabre, dermatitis herpetiformis, erythema dyschromicum perstans, scalp trauma, and break dancing.15–23 The disease has also been reported restricted to an epidermal nevus, in association with etanercept and imiquimod treatment, following whole brain irradiation and after hair transplantation and facial cosmetic surgery.23–30
Pathogenesis and histologic features Although the pathogenesis of lichen planopilaris is similar to that of lichen planus occurring elsewhere, several differences have been reported.31
Lichen planopilaris is considered a hair-specific autoimmune disease in which activated T lymphocytes target follicular antigens, mainly the epithelium of the infundibulo-isthmic region (the bulge area). In the majority of cases it does not affect the hair bulb or the dermal–epidermal interface. The antigen targeted in this response is unknown. Lichen planopilaris has been associated with an increased frequency of HLA DRB111 and DQB103 alleles.32
The histologic study should include an examination of horizontal and vertical sections, (Fig. 22.133).38 However, horizontal sections provide particularly valuable information, as the infiltrate is limited mainly to the infundibulum and isthmic region of the hair follicle. Typical findings consist of a lichenoid tissue reaction with formation of apoptotic bodies within the follicular epithelium but with little involvement of the intervening epidermis. Perifollicular fibrosis facilitates a tendency for the follicles to fuse creating an ‘owl eye’ appearance (Fig. 22.134 and see Fig. 22.117). The lower portion of the hair follicle and the bulb are usually not affected, but in severe cases the inferior segment and the suprabulbar zone may be involved These changes are uneven according to disease progression and provide more information in the active and early-stage disease process. Lichen planopilaris does not usually show the classic bandlike infiltrate seen in ordinary lichen planus.
Some studies have shown an increment in the number of CD8+ T cells compared with the CD4+ T-cell population and a decrease in proliferative bulge stem cells. The latter favors a cell-mediated cytotoxic immune response in the pathogenesis of the disease.33 Nevertheless, a further study has shown low numbers of CD8+ T cells in ‘early’ active stages of the disease and in the late ‘fibrotic’ phase, preservation of the bulge stem cells. This suggests that the irreversible loss of hair follicles bulge cells is not necessarily a consequence of T cell-mediated destruction.34 A further significant finding in the etiopathogenesis of lichen planopilaris has been the observation of an altered distribution of integrins in the affected follicular keratinocytes, facilitating loss of adhesion of follicular keratinocytes to the stroma.35 This could also explain the artifactual clefts observed in histologic
The interface changes are characterized by focal loss of attachment between the follicular epithelium and the surrounding dermis. As a result, artifactual clefts are sometimes apparent and colloid bodies are often found. An associated mononuclear inflammatory cell infiltrate is present within the perifollicular connective tissue sheath, which is usually thickened (Fig. 22.135). Basal follicular keratinocytes in the involved area become squamotized with larger size, prominent eosinophilic cytoplasm, and cytoplasmic angulation (Fig. 22.136). Although mucinous perifollicular fibroplasia may be observed around the follicle, there is no accumulation of dermal mucin (Fig. 22.137, see Fig. 22.111).36
In the late stages, the hair follicle is completely destroyed and replaced by a sclerotic collagenous follicular scar with loss of sebaceous glands. The only structures left are the arrector pili muscles (see Fig. 22.115). On occasions, the predominant pattern is that of foreign body granulomas distributed around the free hair shafts (Fig. 22.138).39,40 Other forms of
1098 Diseases of the hair
infundibular portion of the hair follicle.4 Linear deposition of immunoglobulin (usually IgG or IgA) restricted to the follicular epithelium has also been described.44 However, these immunofluorescence findings are not specific to lichen planopilaris and they may also be observed in other diseases with interface change and damage to the basal cell layer. Increased birefringence within the fibrous tracts is a frequent finding in lichen planopilaris but may occasionally be found in other scarring and nonscarring alopecias (see Fig. 22.113).45,46
scarring alopecia (including pseudopélade of Brocq and discoid lupus erythematosus) share this end-stage histologic appearance. In order to highlight the presence of scarring tissue, special stains to delineate elastic fibers are particularly useful. They allow distinction between normal dermis and scarred areas, as the latter lack elastic fibers. A perifollicular and superficial wedge-shaped scar with loss of the elastic sheath surrounding fibrous tracts is identified, although occasionally it may be seen in other scarring alopecias (Fig. 22.139).41–43
Immunofluorescence studies show staining of colloid bodies with IgM and IgA and linear deposits of fibrin along the basement membrane of the
Differential diagnosis The correct diagnosis may be reached in the majority of the cases by careful correlation of histopathological, clinical, and immunohistopathological findings. The most important entities to consider in the differential diagnosis are discoid lupus erythematosus and pseudopélade of Brocq.
In discoid lupus erythematosus, the typical findings include a superficial and deep perivascular lymphohistiocytic infiltrate, dermal mucin, and vacuolar interphase change affecting not only the follicles but also the intervening dermal–epidermal junction. In lichen planopilaris, the infiltrate is mainly seen around hair follicles, and interface change of the interfollicular epidermis is rarely present.
1099 Scarring alopecias
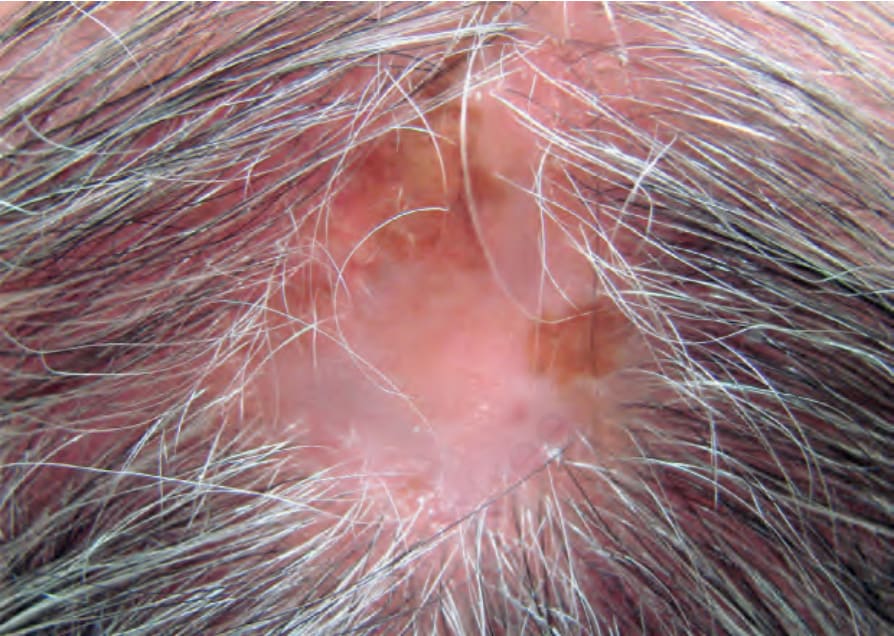
Fig. 22.110 Scarring alopecia, lichen planopilaris: there is a plaque of alopecia with hyper- and hypopigmentation, loss of follicular ostia, and follicular hyperkeratosis at the periphery. Courtesy of J. Gutiérrez, MD, Instituto de Ciencias de la Salud, Medellín, Colombia.
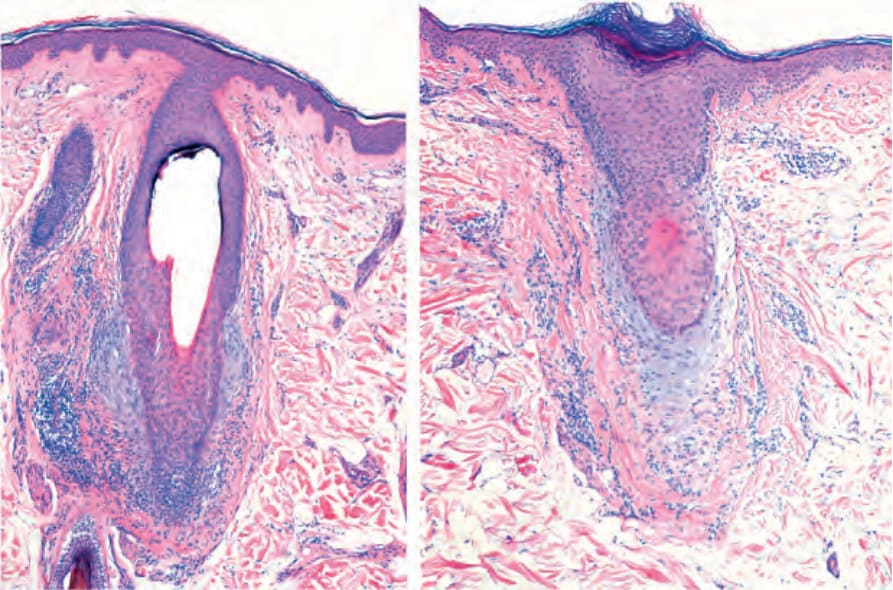
Fig. 22.111 Scarring alopecia, lichen planopilaris. Note the inflammatory infiltrate around the isthmus. There is perifollicular fibrosis, perifollicular mucin deposition and complete loss of sebaceous glands.
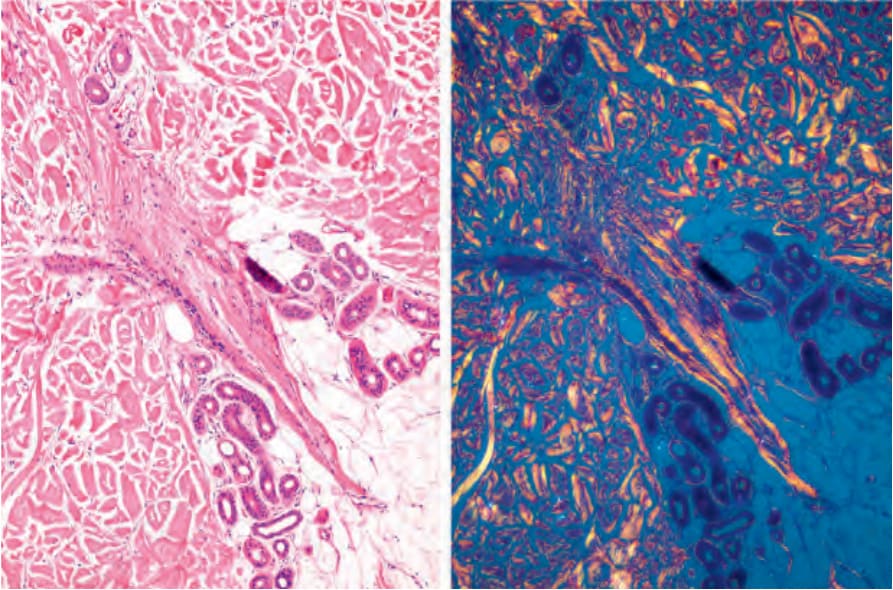
Fig. 22.113 Scarring alopecia, lichen planopilaris, follicular tracts. Note the birefringence of the collagen in the fibrous tract with polarized light.
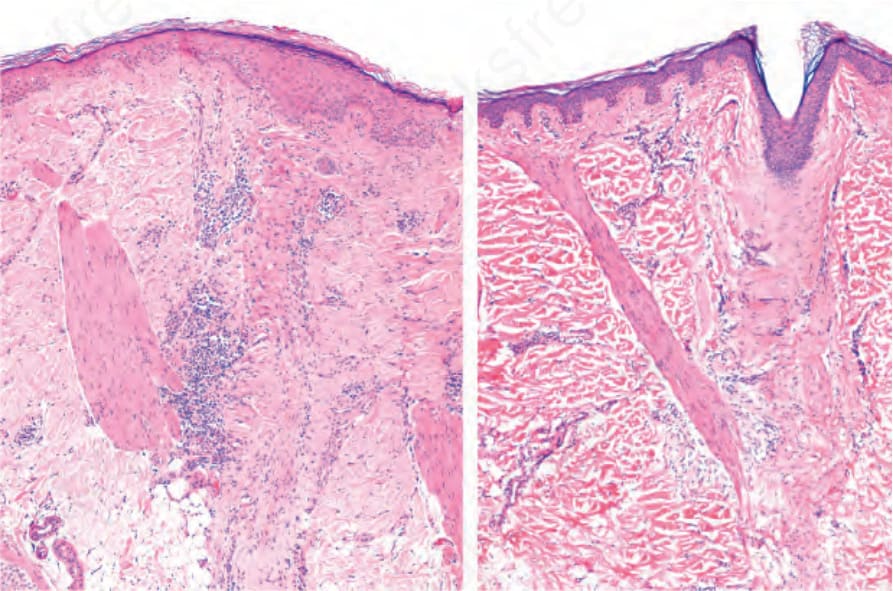
Fig. 22.115 Scarring alopecia, lichen planopilaris: the hair follicles have disappeared and been replaced by two vertical fibrous scars in which an arrector pili muscle is inserted.
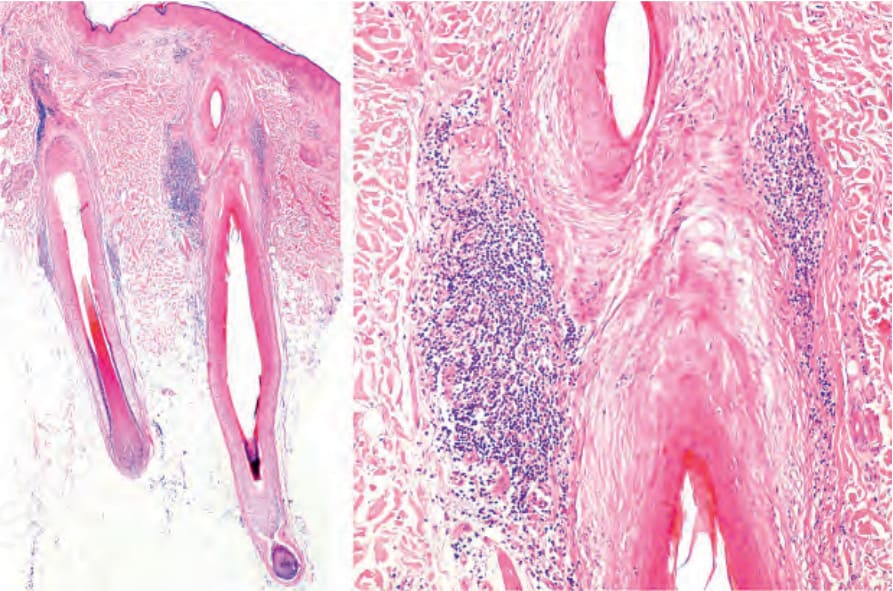
Fig. 22.117 Scarring alopecia, lichen planopilaris: note the lymphocytic infiltrate in the upper segment and in the area of insertion of the arrector pili muscle. In the figure on the right, note the loss of sebaceous glands and the premature shedding of the internal root sheath.
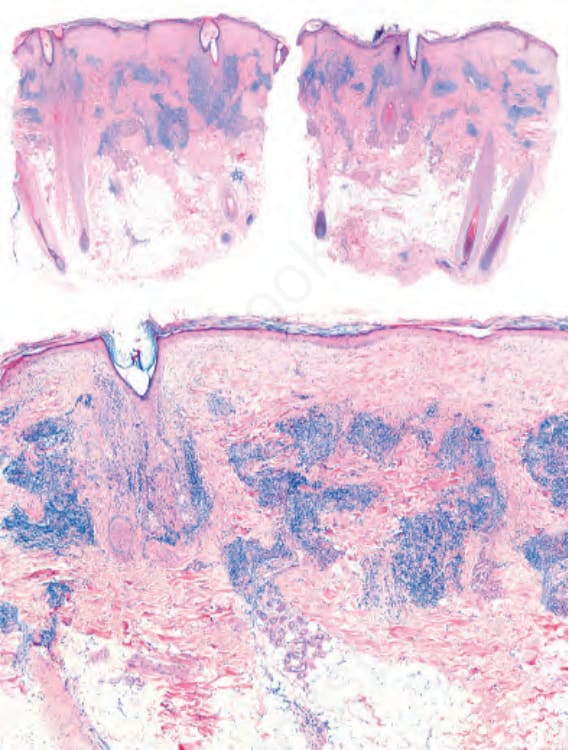
Fig. 22.130 Discoid lupus erythematosus: Prominent inflammatory cell infiltrate located around the upper segment of the hair follicles and also in a perivascular location.

Fig. 22.132 Lichen planopilaris: atrophic patch with loss of follicular orifices, perifollicular erythema, and scaling. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
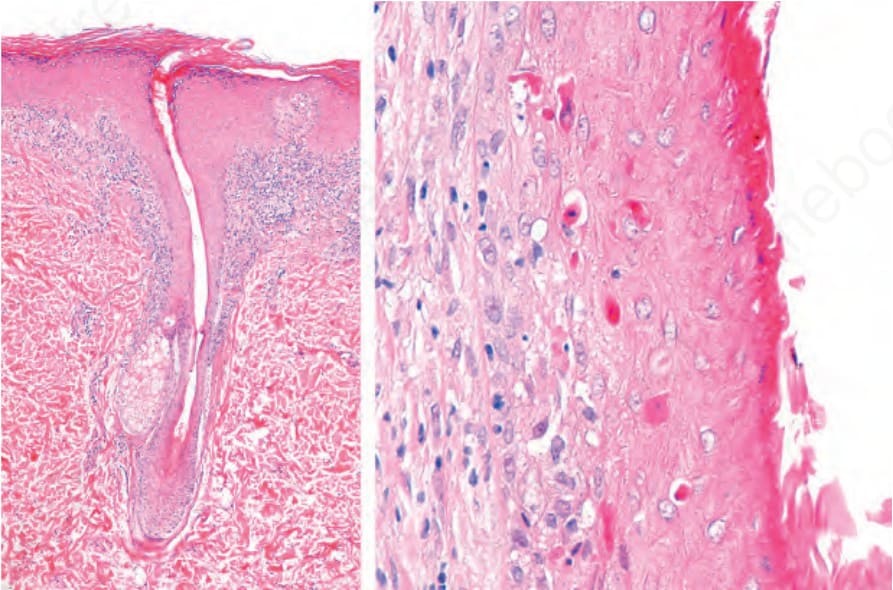
Fig. 22.133 Lichen planopilaris, vertical sections. Left: the inflammatory cell infiltrate surrounds the superior segment without involving the inferior segment. There is complete loss of sebaceous glands. In these cases, an infrequent finding is the subepidermal bandlike inflammatory cell infiltrate. Right: numerous apoptotic bodies are seen in the outer root sheath. There is shedding of the internal root sheath.
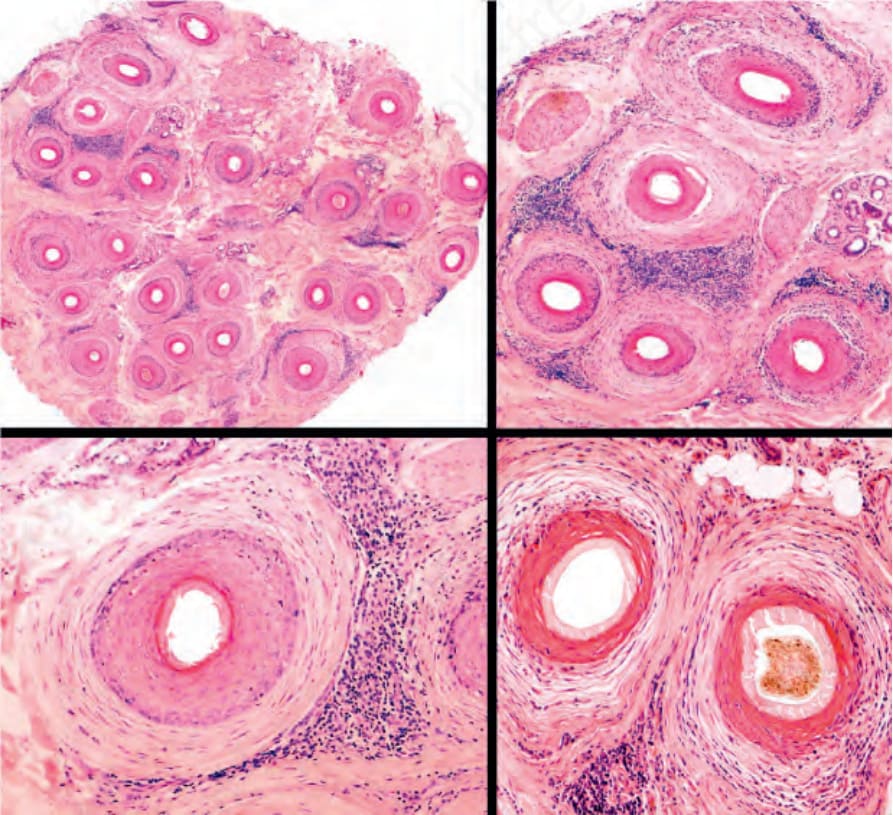
Fig. 22.134 Lichen planopilaris, horizontal sections: in this biopsy, there are no sebaceous glands and all the follicles show a perifollicular mononuclear inflammatory cell infiltrate. Most hair follicles show lamellar fibroplasia separating the lymphocytic infiltrate from the outer root sheath. In the right panel, upper and lower images, an ‘owl eye’ appearance is appreciated.
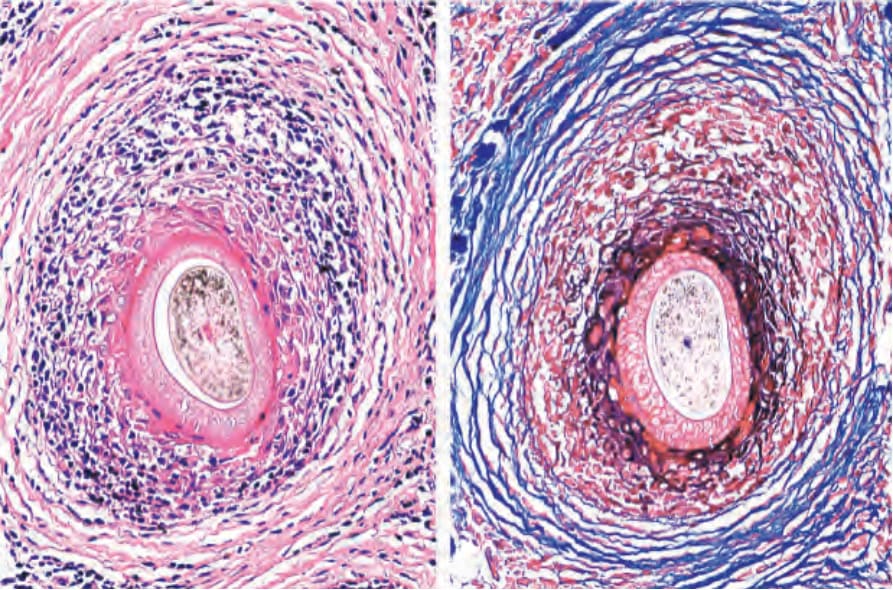
Fig. 22.135 Lichen planopilaris, frontal fibrosing alopecia type: horizontal sections. Left: the destruction of the outer root sheath is evident with interface change, fibrosis and lymphocytic inflammation. Right: with the Mason trichrome staining, the lamellar fibrosis around the mononuclear cell infiltrate is apparent.
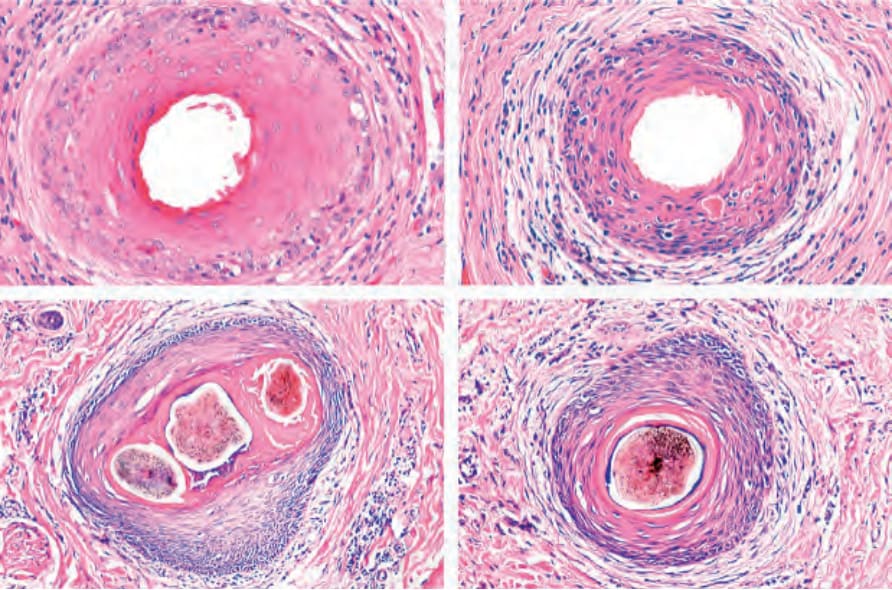
Fig. 22.136 Lichen planopilaris, horizontal sections: photographic composition of the typical changes. (Top) Initial changes with apoptosis and loss of internal root sheath. (Bottom) Advanced changes with fusion of follicles and thinning of the outer root sheath.
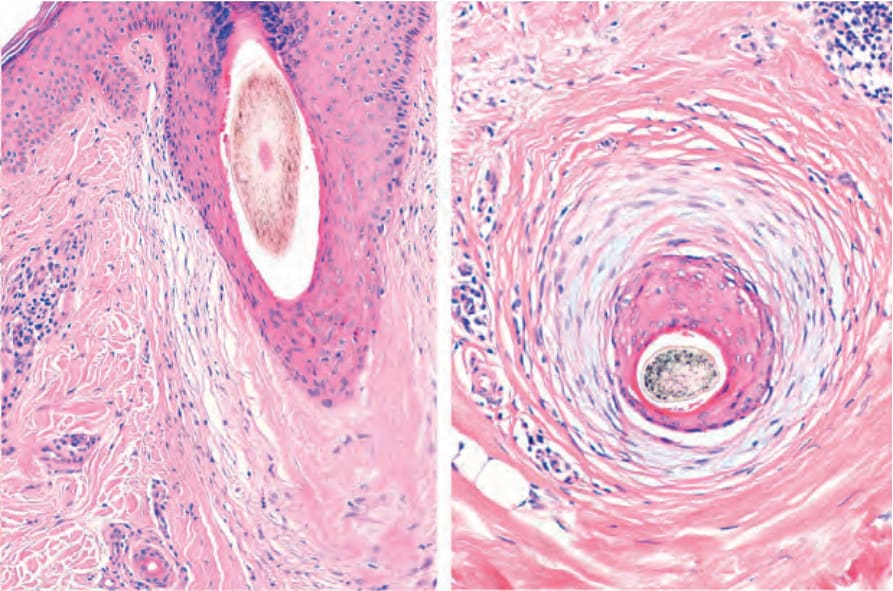
Fig. 22.137 Lichen planopilaris, vertical and horizontal sections: there is mucinous perifollicular fibroplasia.
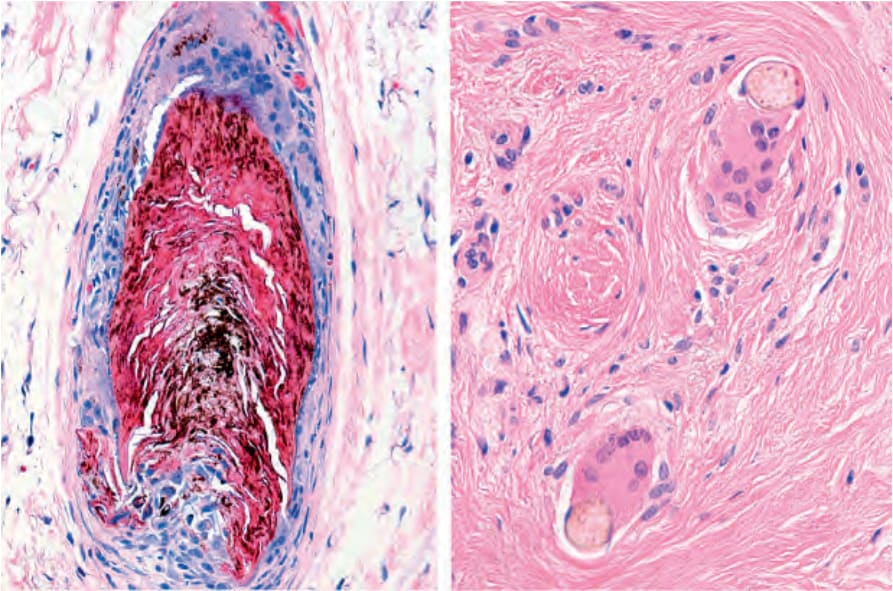
Fig. 22.138 Lichen planopilaris: there are numerous giant and epithelioid cells surrounding the free hair shafts in the dermis.
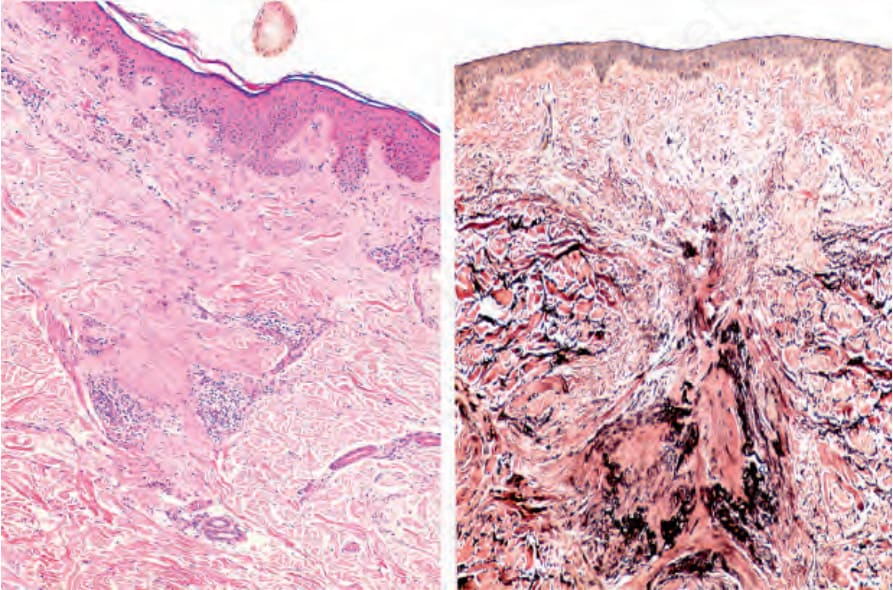
Fig. 22.139 Lichen planopilaris. Left: follicular scar extending from the epidermis to the deep dermis. Right: With the elastic stain loss of elastic fibers in triangular shape with the base toward the epidermis is observed. The follicular scarring shows condensation of elastic fibers with a vertical orientation.
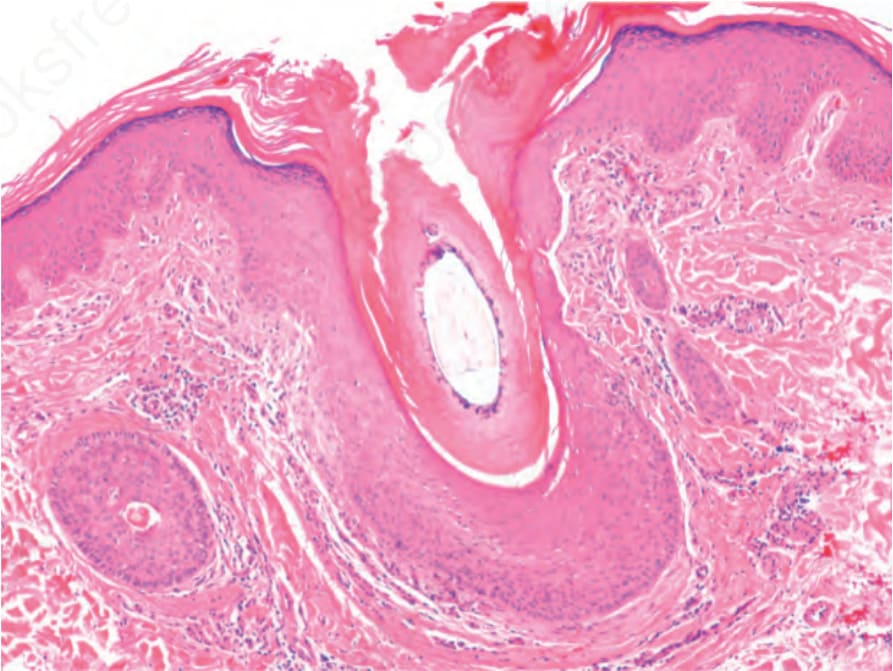
Fig. 22.146 Graham-Little syndrome: dilated infundibulum with hyperkeratosis, mild perifollicular inflammation and fibrosis.
Pseudopélade of Brocq presents as progressive patches of scarring alopecia, and histologically the changes are essentially those of marked scarring with no interface change. It is possible that pseudopélade of Brocq represents a late stage of various forms of scarring alopecia, including lichen planopilaris.
In the end stages of the disease, it may be impossible to differentiate lichen planopilaris from pseudopélade of Brocq and discoid lupus erythematosus. The presence of a band of fibrosis in the papillary dermis accompanied by fibrous tracts in the reticular dermis following the path of destroyed follicles appears to be a valuable pointer toward ‘burn-out’ lesions of lichen planopilaris.47
Clinical features Frontal fibrosing alopecia Kossard first described frontal fibrosing alopecia in 1994 as a variant of scarring alopecia closely related to lichen planus and affecting mainly postmenopausal women (postmenopausal frontal fibrosing alopecia).1,2 However, some cases have been reported in premenopausal women as well as on the
sideburns and beard in males and in patients of African descent.3–10 Furthermore, some cases in children and adolescents have also been described.11,12
It presents with progressive and symmetric recession of the frontal hairline associated with smooth and pale skin. Sometimes perifollicular erythema, follicular keratinization, and extension onto the temporal and parietal zones may be observed (Fig. 22.140). In addition, there is loss or reduction of the hair follicles of the eyebrows, the rest of the face, and also of the extremities, axillae, trunk, and pubis (Fig. 22.141). 13,14 Eyebrow alopecia is thought to precede the scalp alopecia.15
Progression is unpredictable, but the disease becomes stable in almost all patients.16 Clinically, the disease does not present with the multifocal areas of hair loss typically seen in lichen planus or pseudopélade of Brocq. There are usually no manifestations of lichen planus elsewhere although isolated cases have shown typical lichen planus in the skin or mucosae, particularly in pigmented lichen planus.17–21 In some patients, diffuse hair loss has been described. 7,22
1100 Diseases of the hair
A B
Other cases have been associated with some components of Piccardi- Lassueur-Graham-Little syndrome, Sjögren syndrome, bilateral oophorectomy, hair repigmentation close to a patch of frontal fibrosing alopecia, hair transplantation for androgenetic alopecia, increased scalp sweating, and scalp vitiligo.23–29
Pathogenesis and histologic features The pathogenesis of frontal fibrosing alopecia is unknown.30 Some cases of family groupings that share HLA-D have been observed, but it is not a consistent finding.31–34 The disease is considered a frontal variant of lichen planopilaris since the histologic findings are similar.25,35–41 Nevertheless, other studies have found differences in respect to the type of hair follicles affected, emphasizing the selective compromise of vellus-like and indeterminate hair follicles in this disease.42,43 Similar to lichen planopilaris, the histologic changes are not necessarily restricted to the scalp but may be observed on the eyebrows, face, and upper limbs even in asymptomatic patients.44–47
The best biopsies to diagnose fibrous frontal alopecia are those that have been taken guided by dermoscopy and interpreted with horizontal sections. The histologic study shows a decrease in the number of hair follicles, which are replaced by fibrous tracts. There is a lymphocytic infiltrate in a lichenoid pattern, accompanied by perifollicular lamellar fibrosis (Fig. 22.142). The disease in its initial state shows a tendency to simultaneously affect terminal, indeterminate, and vellus hair follicles in all phases of the cycle including telogen. As the disease progresses, the involvement is more restricted to terminal hair follicles.44,48 Sometimes, apoptosis is prominent (Fig. 22.143, see Fig. 22.135). The interfollicular epidermis is not involved.40 The immunofluorescence pattern is similar to that of other more conventional variants of lichen planus.
alopecia, the inflammatory infiltrate is minimal and the histologic picture is dominated by follicular miniaturization. Traction alopecia can be easily differentiated on the basis of physical examination and history of hair traction.
Differential diagnosis The differential diagnoses include female pattern hair loss, androgenetic alopecia, alopecia areata in a ‘sisaipho’ pattern (ophiasis inversus), and marginal traction alopecia.
Female pattern hair loss and androgenetic alopecia are not associated with perifollicular erythema, and female pattern hair loss is not related to frontal hair recession. In alopecia areata, a noninflammatory alopecic band with preservation of follicular orifices and presence of exclamation mark hairs is observed. Dermoscopy could be a helpful diagnostic tool as the yellow dots typically seen in alopecia areata are absent in frontal fibrosing alopecia.49 Histologically, in frontal fibrosing alopecia the infiltrate is found around the isthmus and in alopecia areata the infiltrate is seen around the peribulbar area.50 In cases of female pattern hair loss and androgenetic
Finally, without adequate clinical information, distinction from conventional lichen planopilaris is not possible.
Clinical features Fibrosing alopecia in a pattern distribution Fibrosing alopecia in a pattern distribution was described by Zinkernagel and Trüeb as a form of alopecia that shares similar characteristics with androgenic alopecia and lichen planopilaris. It affects both women and men.1–3 It is clinically characterized by progressive miniaturization of the hairs of the central scalp, perifollicular erythema, and follicular hyperkeratosis leading to complete loss of follicular ostia and scarring (Fig. 22.144).1–3
Pathogenesis and histologic features The pathogenesis of fibrosing alopecia in a pattern distribution is unknown. Histologic features consist of hair follicle miniaturization with a lymphocytic
1101 Scarring alopecias
inflammatory cell infiltrate in the region of the isthmus and the infundibulum (Fig. 22.145). Late lesions are characterized by perifollicular lamellar fibrosis and fibrous follicular tracts.
Differential diagnosis The differential diagnosis includes androgenetic alopecia, lichen planopilaris, and frontal fibrosing alopecia. Although in androgenetic alopecia a peri-infundibular lymphocytic inflammatory cell infiltrate may be seen (see Figs 22.17 and Fig. 22.46), this infiltrate does not concentrate around the isthmus and there is no apoptosis, loss of sebaceous glands, or lamellar fibrosis. Lichen planus is associated with all the latter features, but there is no involvement of vellus hairs by inflammation and there is a lack of miniaturization of hair follicles. In the initial stages of frontal fibrosing alopecia, there may be a predominant involvement of vellus hairs. In these cases, close clinicopathological correlation is necessary.
affects atopic individuals. It is characterized by patchy alopecia of the scalp, eyebrows, and eyelashes. The clinical course is unpredictable: some cases regress during puberty and others progress with variable intensity.

Fig. 22.140 Frontal fibrosing alopecia: bandlike recession of the frontotemporal hairline associated with lateral eyebrow thinning. Note the solitary hairs in the frontal scalp. Courtesy of L.M. Gómez, MD, Universidad Pontificia Bolivariana, Medellín, Colombia.
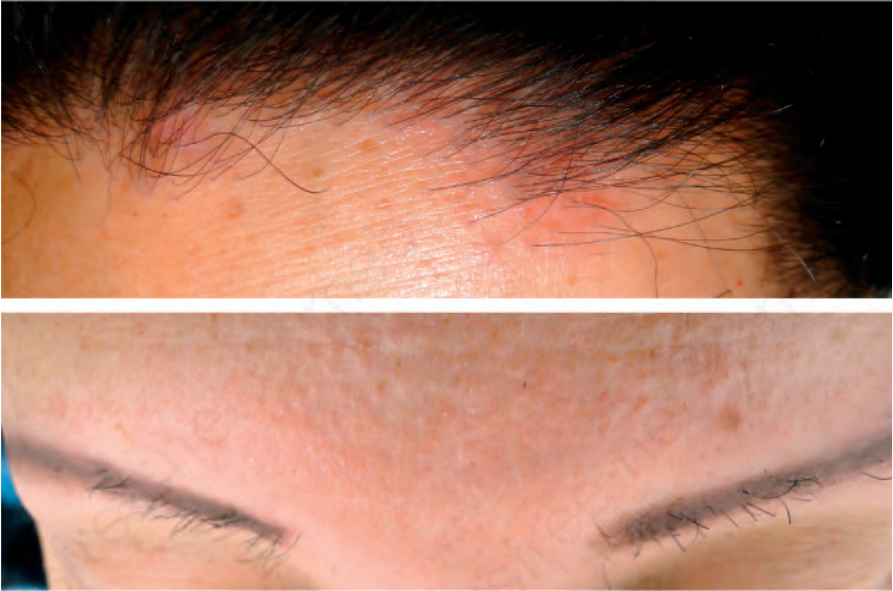
Fig. 22.141 Frontal fibrosing alopecia. Above: there is hair loss on the frontal scalp. The skin shows perifollicular erythema. Below: the skin appears mildly scarred with prominence of the follicles and inflammation. There is almost total absence of eyebrows.
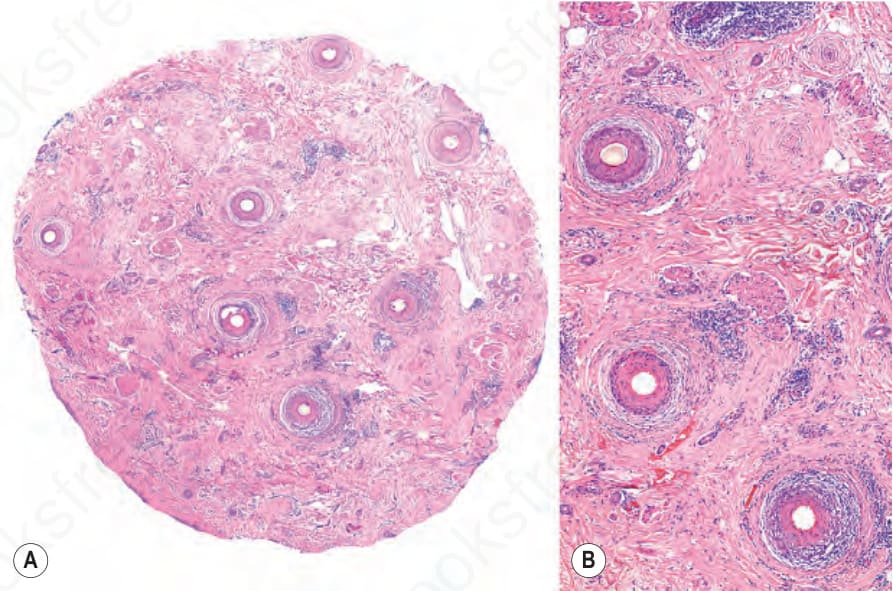
Fig. 22.142 Frontal fibrosing alopecia, horizontal section. (A) In this scanning magnification, there is absence of sebaceous glands, loss of hair follicles, and perifollicular fibrosis. (B) Lichenoid interface dermatitis of the outer root sheath, with vacuolar change, lymphocytic inflammation and perifollicular lamellar fibrosis.
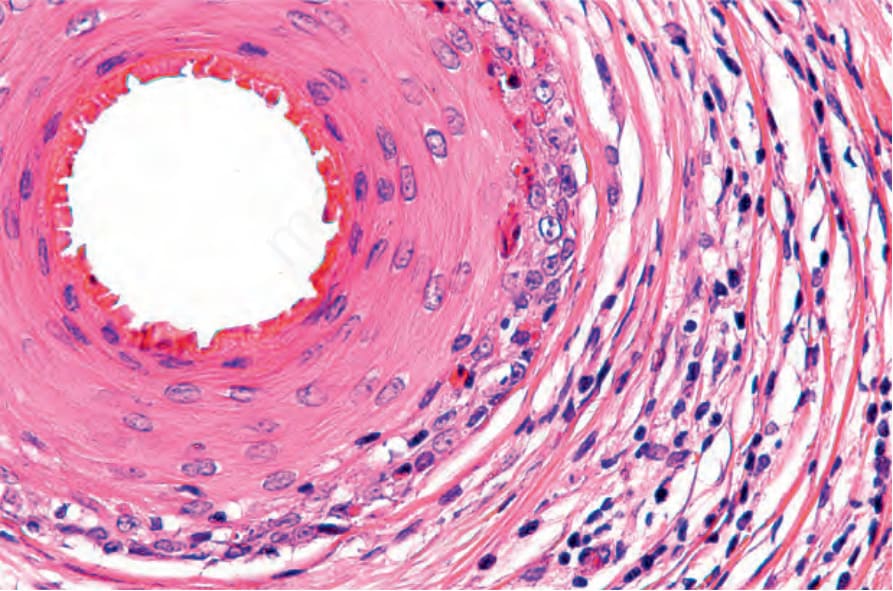
Fig. 22.143 Frontal fibrosing alopecia, horizontal section. The destruction of the outer root sheath is evident with interface change, numerous apoptotic bodies, fibrosis, and lymphocytic inflammation.

Fig. 22.144 Lichen planopilaris, fibrosing alopecia in a pattern distribution. Left: note the absence of follicular orifices with pigment alteration in the pattern of androgenetic alopecia. Right: a male patient with androgenetic alopecia and follicular inflammation. Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.
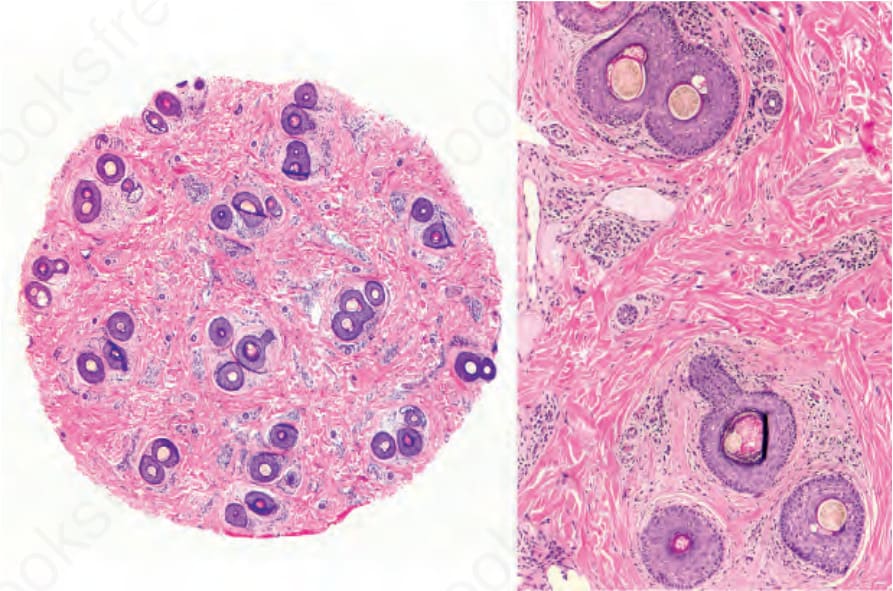
Fig. 22.145 Lichen planopilaris, fibrosing alopecia in a pattern distribution: horizontal section. Extensive miniaturization with loss of sebaceous glands, discrete fibrosis and perifollicular lymphocyte inflammation. Courtesy of Y. Corredoira Salum, MD, Universidad de Chile, Santiago, Chile.
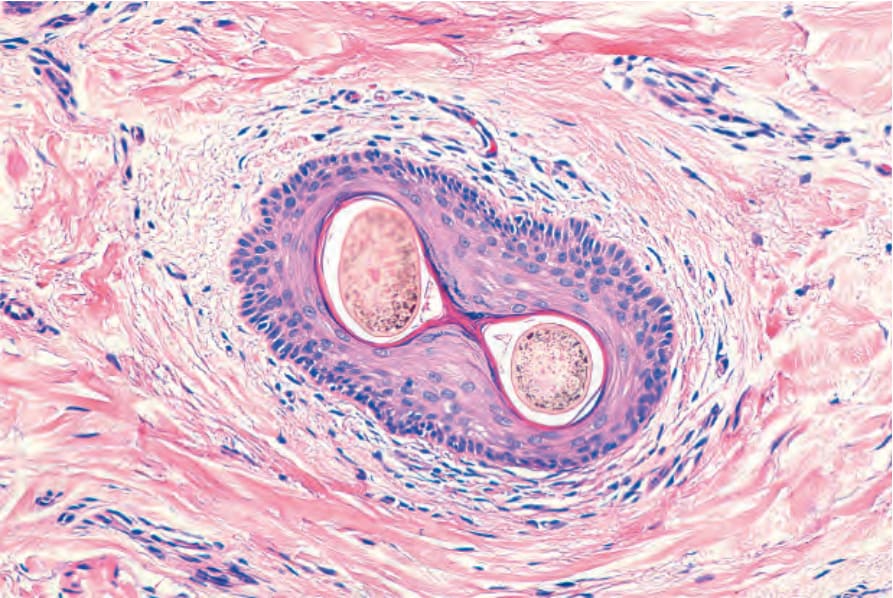
Fig. 22.17 Infundibulum. Horizontal section. The wall is made up of squamous stratified keratinized epithelium. The surrounding dermis is infiltrated by some lymphocytes. There are two hair shafts emerging from a single ostium.
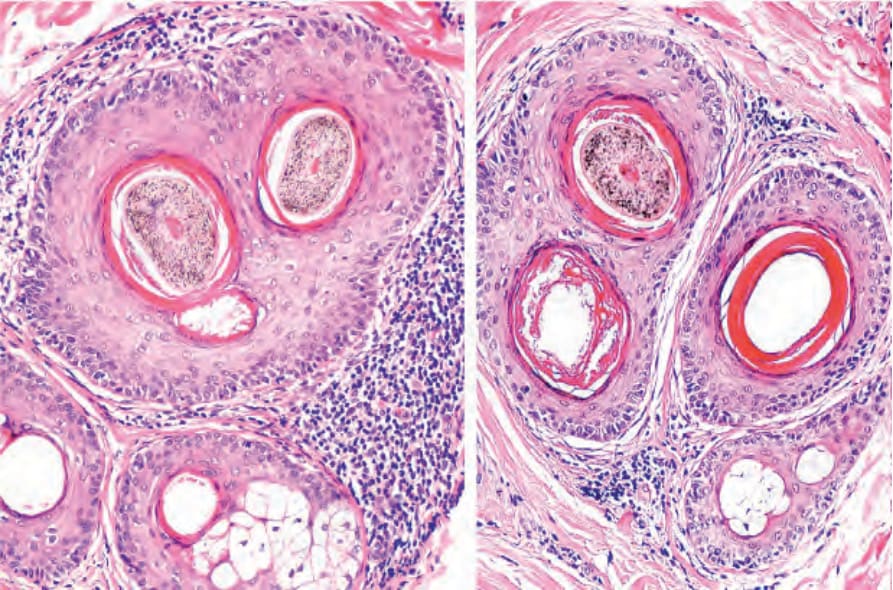
Fig. 22.46 Compound hair infundibulum surrounded by a lymphocytic infiltrate and mild concentric fibrosis in a patient with androgenetic alopecia.