瘢痕性禿髮 (Scarring Alopecias)
脂水腫性禿髮 (lipedematous alopecia) 的臨床外觀具特徵性。毛髮纖細、短、易斷,且長度小於 2 cm。頭皮呈鬆軟海綿樣 (boggy and spongy) 增厚,觸診比目視更為明顯(圖 22.106)。受侵犯部位可能有疼痛與搔癢。診斷可藉由磁振造影 (magnetic resonance imaging, MRI)、電腦斷層掃描 (computed tomography, CT) 及頭部超音波 (head ultrasound),顯示皮下組織不規則增厚而確立。正常頭皮厚度隨年齡而異,20 至 39 歲女性為 4.8 ± 0.12 mm,40 至 69 歲女性為 5.6 ± 0.15 mm。在 lipedematous alopecia 中,頭皮厚度介於 10 至 15 mm。以視訊皮膚鏡 (videodermoscopy) 觀察,lipedematous 頭皮在頭皮皺褶內呈現線狀微血管擴張 (telangiectasia) 區域。
種類繁多的毛囊性與非毛囊性頭皮疾病,包括遺傳性、發育性及後天性疾患,皆可能造成瘢痕化 (scarring) 或永久性禿髮,作為一種次發性現象(圖 22.109)。永久性禿髮亦可能發生於某些非瘢痕性禿髮 (nonscarring alopecias) 的晚期,例如雄性禿 (androgenetic alopecia)、圓禿 (alopecia areata)、乾癬性禿髮 (psoriatic alopecia) 及牽引性禿髮 (traction alopecia)(即「過渡性瘢痕化或雙相型 (transitional scarring or biphasic pattern)」禿髮)。
在本節中,僅描述那些主要侵犯頭皮、或以具特徵性臨床病理特徵次發性侵犯頭皮的疾病。
瘢痕性禿髮 (scarring alopecia) 構成毛髮疾病研究中最困難且最複雜的領域之一。它包含種類繁多的疾病學實體 (nosological entities)。
致病機轉與組織學特徵 對於增厚的脂肪組織 (adipose tissue)、水腫及擴張的淋巴管 (dilated lymphatic vessels) 在毛髮脫落發展中所扮演的角色,一直存在推測。曾有推論認為肥胖與荷爾蒙因素可能扮演某種角色,因為大多數患者為女性。Leptin 亦可能在脂肪組織的分布上扮演角色。目前,本病的確切致病機轉仍屬未知。
頭皮切片必須夠深,並包含皮下組織的全層厚度,達到帽狀腱膜 (galea),因為淺層切片可能造成正常的假象。檢體必須以連續垂直切片 (serial vertical sections) 處理。其組織學特徵包括頭皮厚度增加近乎一倍,伴有組織水腫、皮下脂肪 (subcutaneous fat) 擴張,以及脂肪向真皮浸潤(圖 22.107)。在某些病例中曾觀察到擴張的淋巴管。亦有黏液蛋白沉積 (mucin deposition)
1090 Diseases of the hair
(圖 22.110)。組織病理上的標誌通常是環繞隆突部 (bulge) 與峽部 (isthmus) 的發炎浸潤,以及皮脂腺 (sebaceous glands) 的消失,其後接著形成瘢痕,毛囊被毛囊纖維束 (follicular fibrous tracts) 所取代(圖 22.111 與 22.112)。這些纖維束明確代表瘢痕化,與雄性禿 (androgenic alopecia) 及休止期落髮 (telogen effluvium) 所見的毛囊星狀體 (follicular stellae) 不同。它們從表皮延伸至深層真皮。以偏振光 (polarized light) 易於辨識(圖 22.113,並見圖 22.34)。組織化學染色,包括彈性纖維染色 (elastic stain) 與三色染色 (trichrome),對於界定瘢痕化區域,以及與盤狀紅斑性狼瘡 (discoid lupus erythematosus)、毛髮扁平苔癬 (lichen planopilaris) 及 Brocq 假性斑禿 (pseudopélade of Brocq) 的鑑別診斷皆有用(圖 22.114)。有時毛囊唯一殘留的結構僅是豎毛肌 (arrector pili muscle)(圖 22.115)。
它包含不同病因與獨特臨床特徵的疾病。然而,特徵性發現通常僅在早期才明顯,隨著疾病進展,不同疾病的臨床與病理特徵彼此重疊,往往使分類變得不可能。
瘢痕性禿髮的特徵為毛囊與毛幹的不可逆喪失與破壞。常伴隨(但非總是)有真皮纖維化 (dermal fibrosis)。臨床檢查顯示毛囊口 (follicular ostia) 消失(通常呈局灶性分布)、皮膚硬化 (induration) 或萎縮 (atrophy)、色素改變、毛囊角栓 (follicular plugging),偶爾可見毛囊膿皰 (follicular pustules)。
從臨床處置的角度來看,瘢痕性禿髮代表一種真正的「毛髮學急症 (trichologic emergency)」,因為在短時間內毛囊可能被永久破壞。所造成的禿髮是不可逆的,並有顯著的心理衝擊。由於治療是依組織病理發現來引導,頭皮切片應為處置的第一步。
1091 Scarring alopecias
A
瘢痕性禿髮中的頭皮切片 (Scalp biopsies in cicatricial alopecia) 頭皮切片是所有原發性瘢痕性禿髮 (primary scarring alopecia) 病例中達成診斷最重要的檢查。應取自活動性邊緣 (active border)。可能需要多處切片才能達到確定診斷。理想上,應檢查垂直與水平切片,並以 hematoxylin and eosin、PAS 及彈性組織染色 (elastic tissue stains)。同時使用水平與垂直切片可產生較高的結果,因為它使病理學家得以評估發炎浸潤的類型與位置、纖維化的有無、毛囊的形態,以及其所處的週期階段(圖 22.116;見圖 22.112)。在僅有瘢痕而無發炎浸潤或毛囊的晚期病例中,直接免疫螢光 (direct immunofluorescence) 評估在 discoid lupus erythematosus、lichen planopilaris 與 pseudopélade of Brocq 之間的鑑別診斷上可能極有幫助。用於免疫螢光研究時,可使用送交垂直切片之打孔切片 (punch biopsy) 的後半部(見圖 22.9)。
重要的是不可忘記,瘢痕性禿髮患者的評估需要非常緊密的臨床病理對照、詳盡的臨床
B
病史,以及實驗室檢查,包括梅毒血清學 (serology for syphilis)、直接革蘭氏染色 (direct Gram) 與 PAS 染色,以及病灶培養。
致病機轉 (Pathogenesis) 瘢痕化的病理生理學尚不明確,並依造成永久性毛髮脫落的不同過程而異。然而,已浮現出一些關於隆突部 (bulge) 富含幹細胞區域、皮脂腺及外毛根鞘 (outer root sheath) 改變的統合性通則。
1092 Diseases of the hair
在許多造成瘢痕性禿髮的疾病中,發炎浸潤集中於毛囊的上部,侵犯隆突部,並因而侵犯幹細胞(圖 22.117,見圖 22.111 與 22.112)。這損害了毛囊的再生能力。此種損害可能是物理性的,或藉由抑制功能而導致毛囊間質細胞 (mesenchymal cells) 與隆突部上皮 (bulge epithelium) 間交互作用的干擾。毛囊週期因而被廢止。滯留的毛幹脹破毛球 (bulb),游離於真皮中,誘發強烈的肉芽腫性發炎反應 (granulomatous inflammatory response) 伴隨瘢痕化(圖 22.118 與 22.119)。唯一發炎浸潤環繞隆突部的情況是頭皮剝離性蜂窩組織炎 (dissecting cellulitis of the scalp)(perifolliculitis capitis abscedens et suffodiens),其浸潤非常深,位於真皮與皮下組織交界處。
瘢痕性禿髮另一個常見的相關標記是皮脂腺的早期喪失。此一觀察已在 asedia 突變鼠變異株中被廣泛研究,該株缺乏製造皮脂 (sebum) 的基因、具有發育不全的腺體,並迅速發展出瘢痕性禿髮。因此看來,浸潤定位於毛囊上部(包括隆突部)對於永久性損害的發展至關重要。
淋巴球性 (Lymphocytic) 慢性皮膚紅斑性狼瘡 (Chronic cutaneous lupus erythematosus)
毛髮扁平苔癬 (Lichen planopilaris)
典型毛髮扁平苔癬 (Classic lichen planopilaris)
額部纖維化性禿髮 (Frontal fibrosing alopecia)
Graham-Little syndrome
1093 Scarring alopecias
典型假性斑禿 (Classic pseudopelade)(Brocq)
中央離心性瘢痕性禿髮 (Central centrifugal cicatricial alopecia)
黏液性禿髮 (Alopecia mucinosa)
脫髮性棘狀毛囊角化症 (Keratosis follicularis spinulosa decalvans)
嗜中性球性 (Neutrophilic) 脫髮性毛囊炎 (Folliculitis decalvans)
剝離性蜂窩組織炎/毛囊炎 (Dissecting cellulitis/folliculitis)(perifolliculitis capitis abscedens et suffodiens)
混合性 (Mixed) 瘢痕疙瘩性毛囊炎(痤瘡)(Folliculitis (acne) keloidalis)
壞死性毛囊炎(痤瘡)(Folliculitis (acne) necrotica)
侵蝕性膿皰性皮膚病 (Erosive pustular dermatosis)
非特異性 (Nonspecific)
*Olsen, E.A., Bergfeld, W.F., Cotsarelis, G. et al. (2003). Workshop on Cicatricial Alopecia. Summary of North American Hair Research Society (NAHRS)-sponsored Workshop on Cicatricial Alopecia. J Am Acad Dermatol, 48, 103–110.
瘢痕性禿髮的分類 (Classification of scarring alopecias) 關於瘢痕性禿髮的分類,有多少位撰文討論此主題的作者,就有多少種分類。
鑑於許多原發性瘢痕性禿髮具有共同的臨床與組織學特徵,不同臨床變異型之間的區分往往非常困難。因此,有人提議將原發性瘢痕性禿髮 (primary cicatricial alopecia) 依據在受侵犯毛囊內及周圍占優勢的浸潤類型,分成數組(淋巴球性、嗜中性球性、混合性及非特異性)(表 22.4)。
此分類是由北美毛髮研究學會 (North American Hair Research Society, NAHRS) 於北卡羅萊納州 Duke University 舉行的第一次瘢痕性禿髮共識會議(2001)所提出。它已獲廣泛接受,因此將作為本章的基礎。
淋巴球相關性原發性瘢痕性禿髮 (Lymphocyte-associated primary cicatricial alopecias) 這一組瘢痕性禿髮的特徵為淋巴球浸潤,其總是侵犯毛囊隆突部周圍的上段。一般而言,除非毛囊破裂引發肉芽腫性反應,否則此浸潤不會改變。會有皮脂腺的喪失,以及毛囊融合,融合數目為二至最多三個。此種融合必須與正常毛囊在毛漏斗 (infundibular) 層常見的融合相區別,因此瘢痕性禿髮的評估必須在峽部 (isthmus) 層或更深處進行(圖 22.120;亦見圖 22.17 與 22.46)。
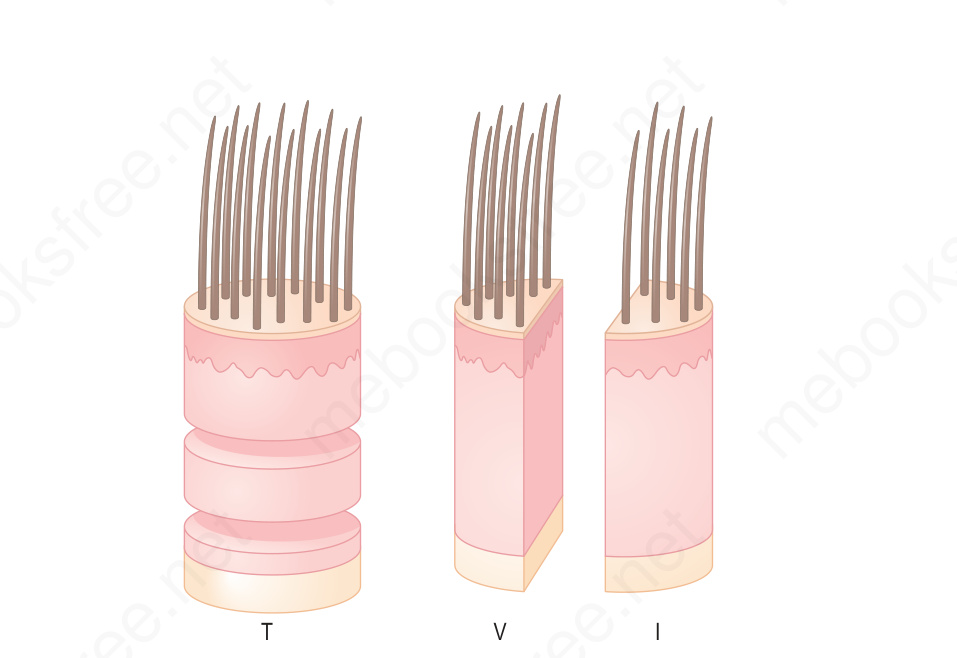
圖 22-9:毛髮切片,橫向 (T) 與垂直 (V) 切片:理想上應取得兩處切片。其中一處在不同層面作水平切片,第二處可垂直分為兩半,一半作常規組織學,另一半作免疫螢光 (I)、電子顯微鏡、培養及其他技術。垂直切片適用於不需比較或毛囊計數的病例,例如瘢痕性禿髮。此型切片不可用於非瘢痕性禿髮、電子顯微鏡、培養及其他技術。垂直切片適用於不需比較或毛囊計數的病例,例如瘢痕性禿髮。此型切片不可用於非瘢痕性禿髮。 (Hair biopsy, transversal (T) and vertical (V) sections)
Fig. 22.9 Hair biopsy, transversal (T) and vertical (V) sections: ideally, two biopsies should be obtained. One of them is sectioned horizontally at different levels and the second can be vertically divided in two halves, one for routine histology and the other for immunofluorescence (I), electron microscopy, cultures and other techniques. Vertical sections are useful in cases that do not require comparison or follicle quantification; for example, in scarring alopecias. This type of sections must not be used in nonscarring alopecias, electron microscopy, cultures and other techniques. Vertical sections are useful in cases that do not require comparison or follicle quantification; for example, in scarring alopecias. This type of sections must not be used in nonscarring alopecias.
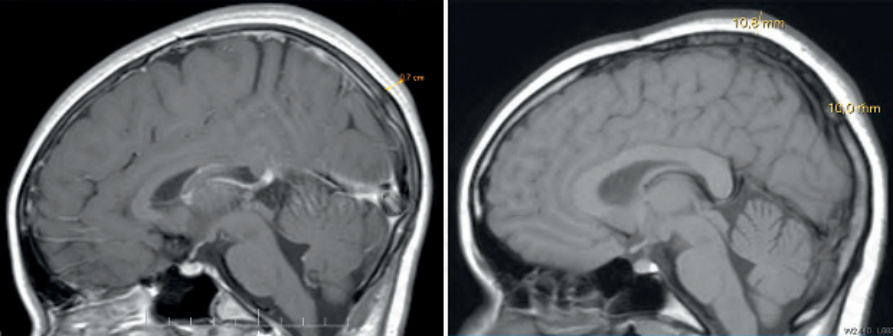
圖 22-106:脂水腫性禿髮 (lipedematous alopecia):注意左側正常頭皮厚度與右側 lipedematous alopecia 病例中頭皮厚度增加之間的差異。Courtesy of T. González, MD, CES, Medellín, Colombia。 (Lipedematous alopecia)
Fig. 22.106 Lipedematous alopecia: note the difference between the normal thickness of the scalp on the left and the increased thickness of the scalp on the right in a case of lipedematous alopecia. Courtesy of T. González, MD, CES, Medellín, Colombia.
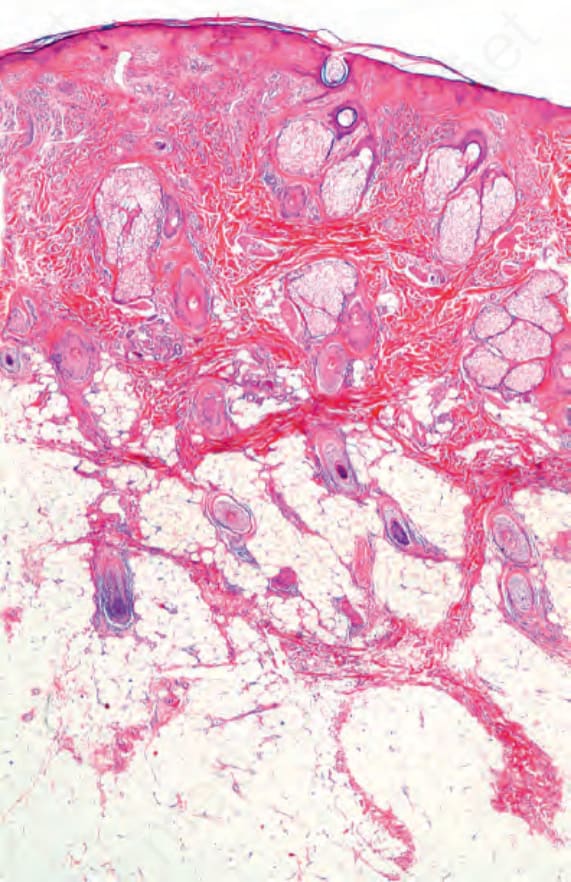
圖 22-107:脂水腫性禿髮 (lipedematous alopecia)。皮下組織增厚,無黏液蛋白沉積 (mucin deposition)。 (Lipedematous alopecia)
Fig. 22.107 Lipedematous alopecia. The subcutaneous tissue is thickened, in the absence of mucin deposition.

圖 22-108:迴狀頭皮 (cutis verticis gyratum)。由增厚的頭皮形成的迂迴皺褶與溝紋,呈腦回狀 (cerebriform) 型態。Courtesy of N. Valderrama, MD, Cali, Colombia。 (Cutis verticis gyratum)
Fig. 22.108 Cutis verticis gyratum. Convoluted folds and furrows formed from thickened skin of the scalp in a cerebriform pattern. Courtesy of N. Valderrama, MD, Cali, Colombia.

圖 22-109:續發於親毛囊性蕈狀肉芽腫 (folliculotropic mycosis fungoides) 的瘢痕性禿髮。枕部與後頂部區域毛髮完全喪失。Courtesy of Y. Corredoira Salum, MD, Universidad de Chile, Santiago, Chile。 (Scarring alopecia secondary to folliculotropic mycosis fungoides)
Fig. 22.109 Scarring alopecia secondary to folliculotropic mycosis fungoides. There is total loss of hair in the occipital and posterior parietal regions. Courtesy of Y. Corredoira Salum, MD, Universidad de Chile, Santiago, Chile.
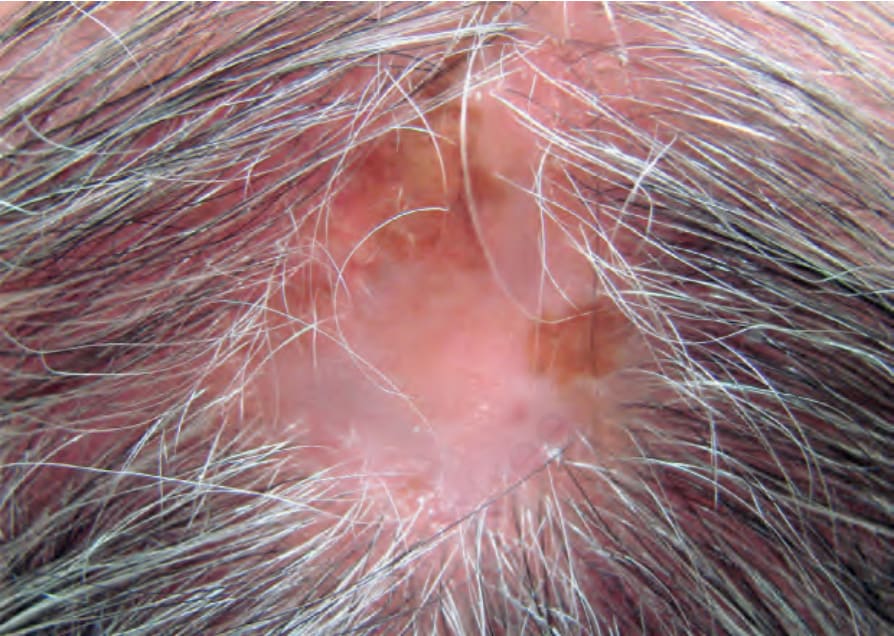
圖 22-110:瘢痕性禿髮,毛髮扁平苔癬 (lichen planopilaris):有一塊禿髮斑塊,伴有過度與低度色素沉著、毛囊口喪失,以及周邊的毛囊過度角化 (follicular hyperkeratosis)。Courtesy of J. Gutiérrez, MD, Instituto de Ciencias de la Salud, Medellín, Colombia。 (Scarring alopecia, lichen planopilaris)
Fig. 22.110 Scarring alopecia, lichen planopilaris: there is a plaque of alopecia with hyper- and hypopigmentation, loss of follicular ostia, and follicular hyperkeratosis at the periphery. Courtesy of J. Gutiérrez, MD, Instituto de Ciencias de la Salud, Medellín, Colombia.
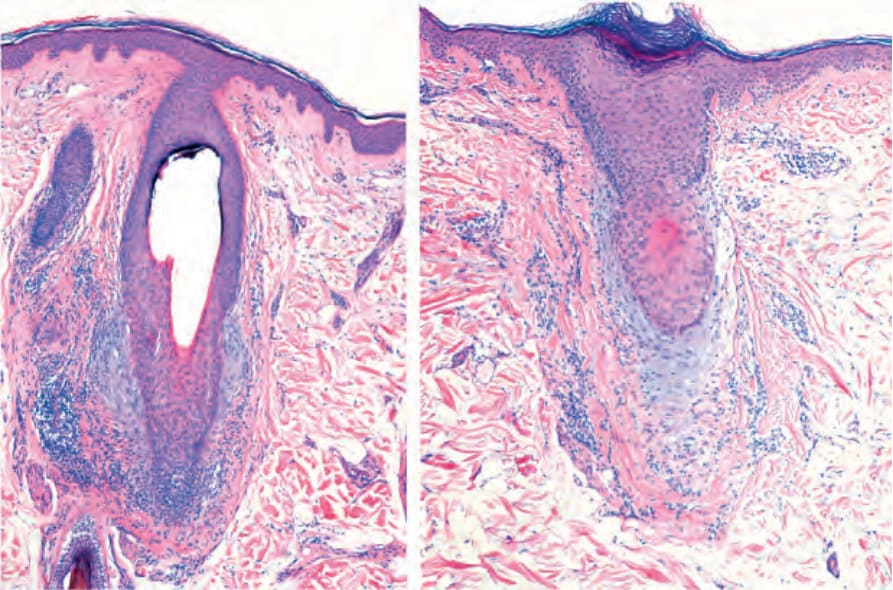
圖 22-111:瘢痕性禿髮,毛髮扁平苔癬 (lichen planopilaris)。注意峽部 (isthmus) 周圍的發炎浸潤。有毛囊周圍纖維化 (perifollicular fibrosis)、毛囊周圍黏液蛋白沉積,以及皮脂腺完全喪失。 (Scarring alopecia, lichen planopilaris)
Fig. 22.111 Scarring alopecia, lichen planopilaris. Note the inflammatory infiltrate around the isthmus. There is perifollicular fibrosis, perifollicular mucin deposition and complete loss of sebaceous glands.
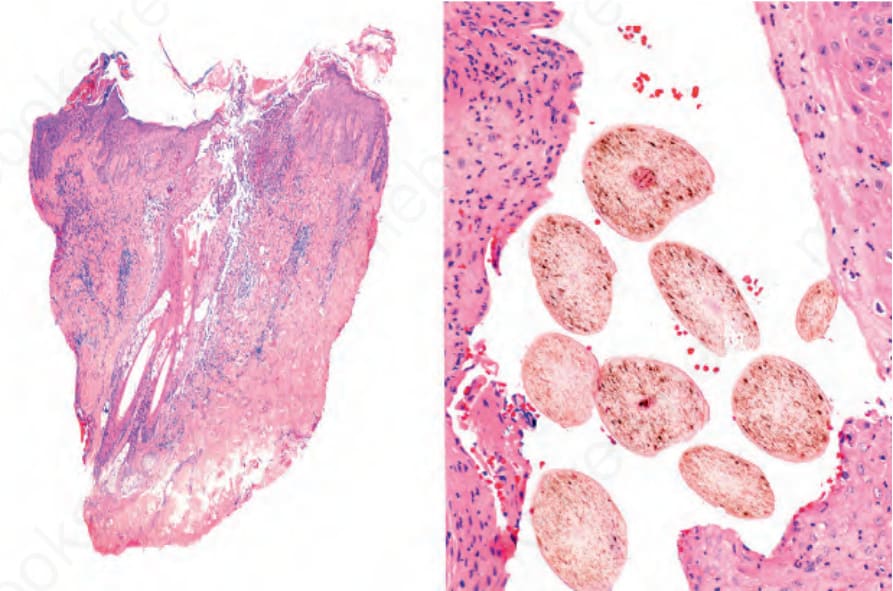
圖 22-112:瘢痕性禿髮,脫髮性毛囊炎 (folliculitis decalvans)。垂直與水平切片。毛囊與皮脂腺的破壞伴隨毛囊周圍與毛囊間纖維化。右側可見毛囊融合,多根毛幹與單一毛漏斗 (infundibulum) 相連(叢狀毛囊炎,tufted folliculitis)。 (Scarring alopecia, folliculitis decalvans)
Fig. 22.112 Scarring alopecia, folliculitis decalvans. Vertical and horizontal sections. The destruction of hair follicles and sebaceous glands is associated with peri and interfollicular fibrosis. On the right side, fusion of follicles with numerous hair shafts associated with a single infundibulum (tufted folliculitis).
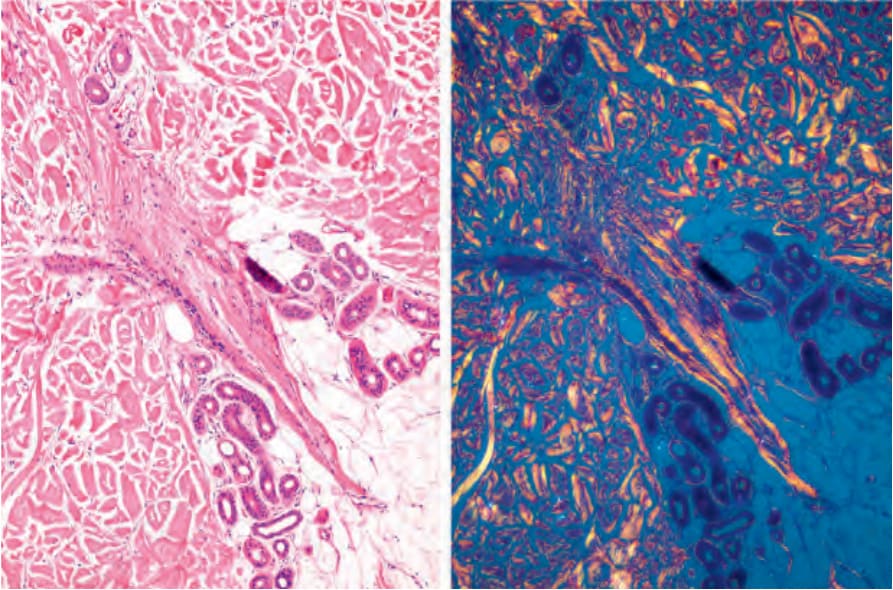
圖 22-113:瘢痕性禿髮,毛髮扁平苔癬 (lichen planopilaris),毛囊束 (follicular tracts)。注意偏振光下纖維束內膠原蛋白的雙折射 (birefringence)。 (Scarring alopecia, lichen planopilaris, follicular tracts)
Fig. 22.113 Scarring alopecia, lichen planopilaris, follicular tracts. Note the birefringence of the collagen in the fibrous tract with polarized light.
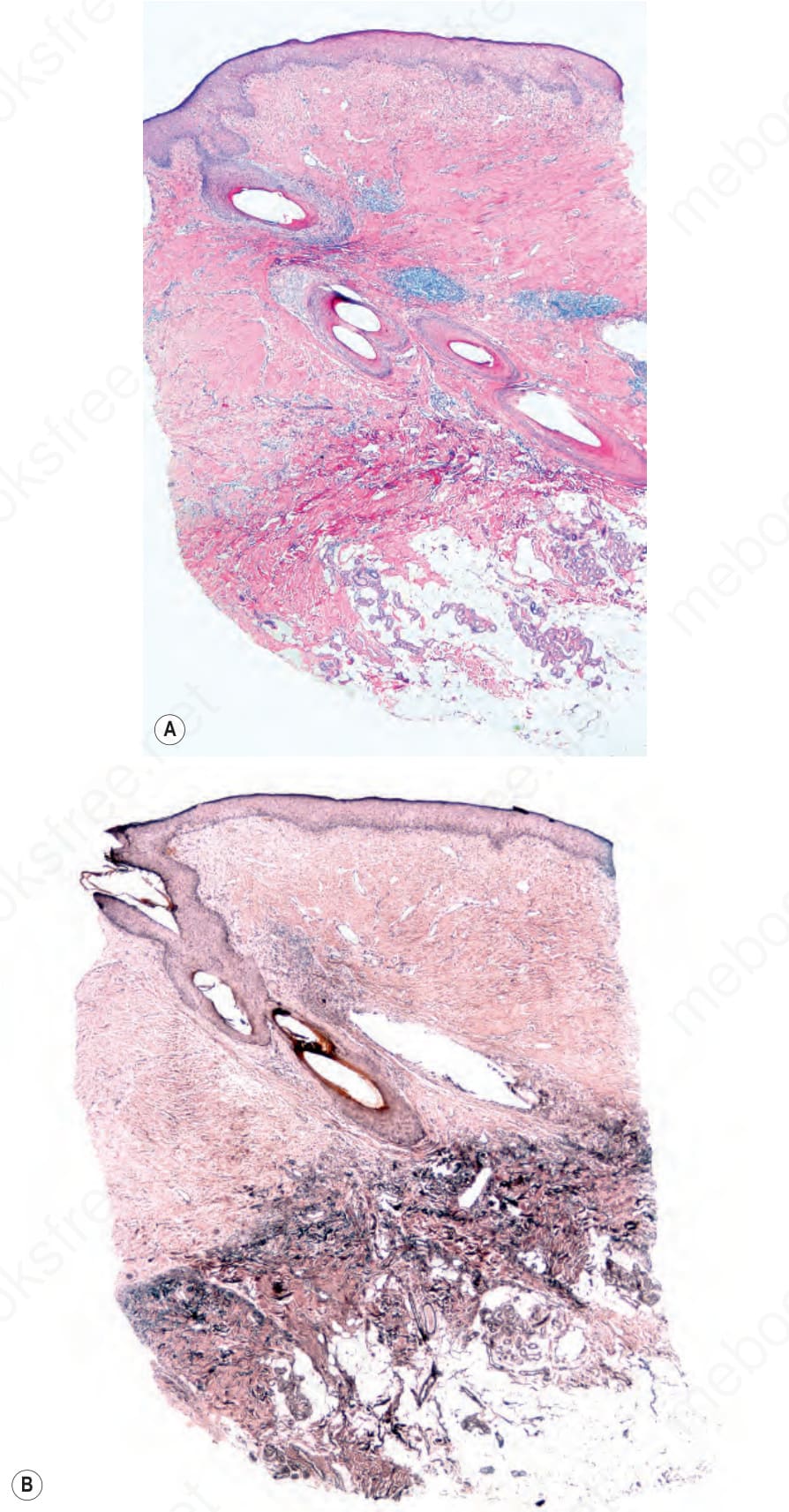
圖 22-114:瘢痕性禿髮,末期紅斑性狼瘡 (end-stage lupus erythematosus)。(A) 有數個融合的毛囊伴發炎細胞浸潤,皮脂腺缺如。(B) 彈性纖維染色 (elastic stain) 顯示環繞毛囊上部的真皮無染色,係因彈性纖維 (elastic fibers) 廣泛喪失與瘢痕化所致。 (Scarring alopecia, end-stage lupus erythematosus)
Fig. 22.114 Scarring alopecia, end-stage lupus erythematosus. (A) There are several fused follicles with an inflammatory cell infiltrate and absent sebaceous glands. (B) Elastic stain shows absence of staining in the dermis that surrounds the upper part of the hair follicle due to extensive loss of elastic fibers and scarring.
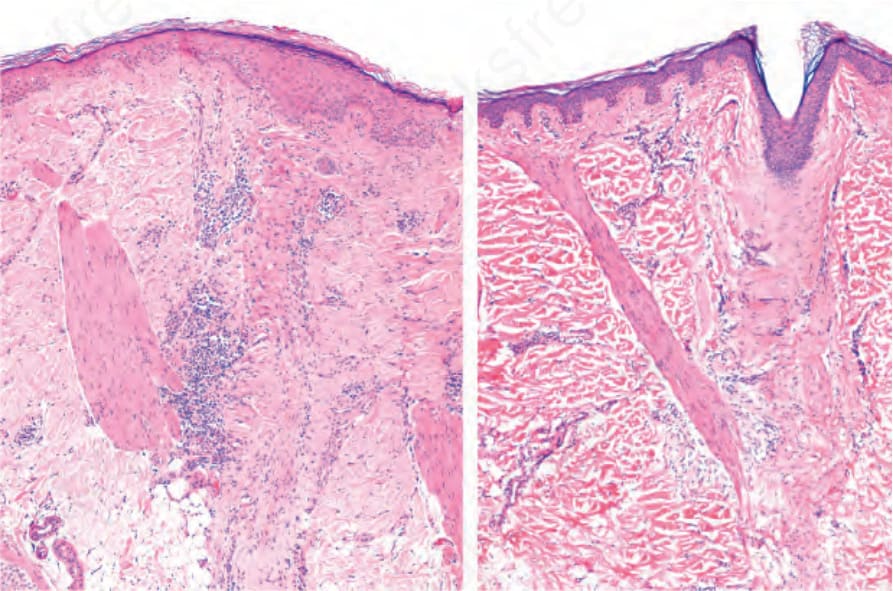
圖 22-115:瘢痕性禿髮,毛髮扁平苔癬 (lichen planopilaris):毛囊已消失,被兩條垂直纖維性瘢痕所取代,其中嵌入一條豎毛肌 (arrector pili muscle)。 (Scarring alopecia, lichen planopilaris)
Fig. 22.115 Scarring alopecia, lichen planopilaris: the hair follicles have disappeared and been replaced by two vertical fibrous scars in which an arrector pili muscle is inserted.
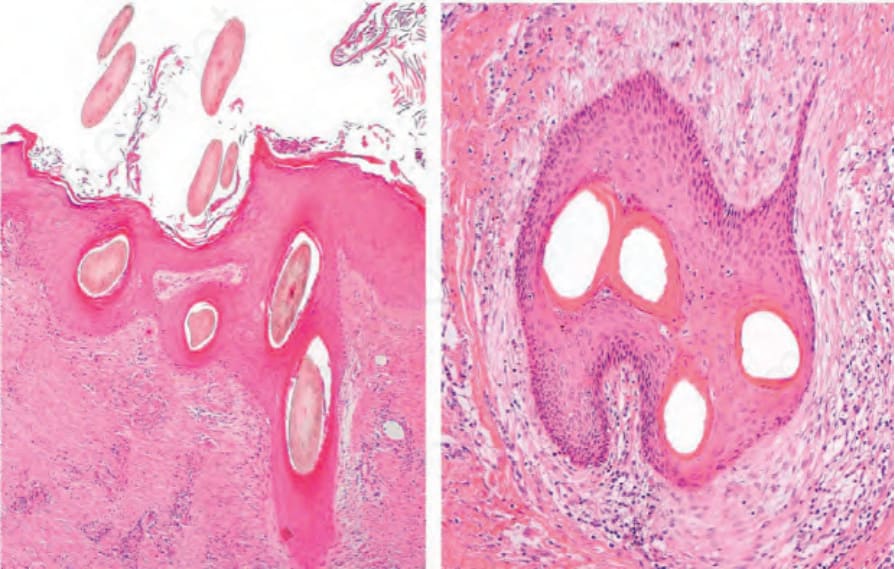
圖 22-116:瘢痕性禿髮,垂直與水平切片:此切片以兩個平面切開,提供叢狀毛囊炎(多毛症,polytrichia)的互補視野,毛囊融合為單一毛囊結構,內含多根毛幹經由單一毛囊口 (ostium) 由表面伸出。 (Scarring alopecia, vertical and horizontal sections)
Fig. 22.116 Scarring alopecia, vertical and horizontal sections: this biopsy has been cut in two planes allowing a complementary view of tufted folliculitis (polytrichia) with hair follicle fusion into a single follicular structure which contains multiple hair shafts emerging at the surface through a single ostium.
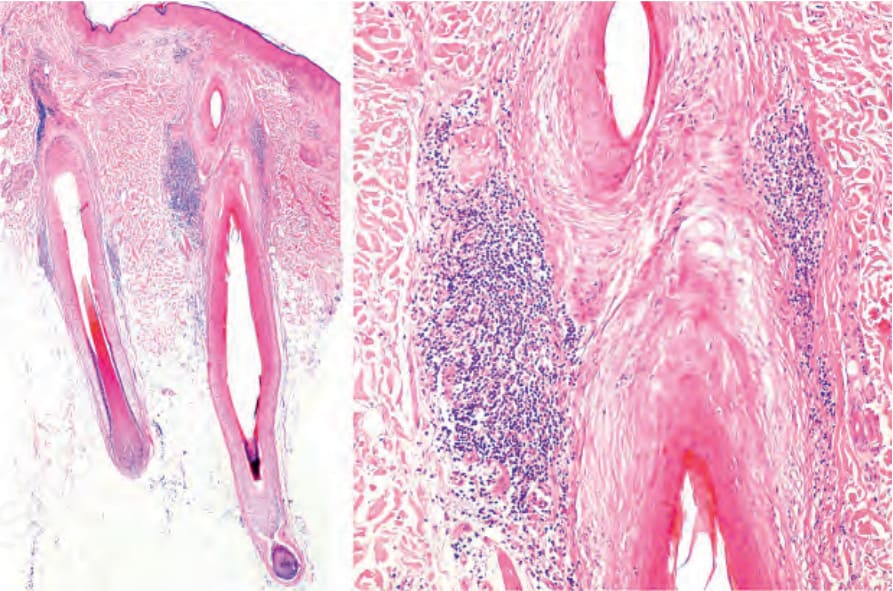
圖 22-117:瘢痕性禿髮,毛髮扁平苔癬 (lichen planopilaris):注意上段及豎毛肌 (arrector pili muscle) 嵌入區域的淋巴球浸潤。在右側圖中,注意皮脂腺的喪失及內毛根鞘 (internal root sheath) 的過早脫落。 (Scarring alopecia, lichen planopilaris)
Fig. 22.117 Scarring alopecia, lichen planopilaris: note the lymphocytic infiltrate in the upper segment and in the area of insertion of the arrector pili muscle. In the figure on the right, note the loss of sebaceous glands and the premature shedding of the internal root sheath.
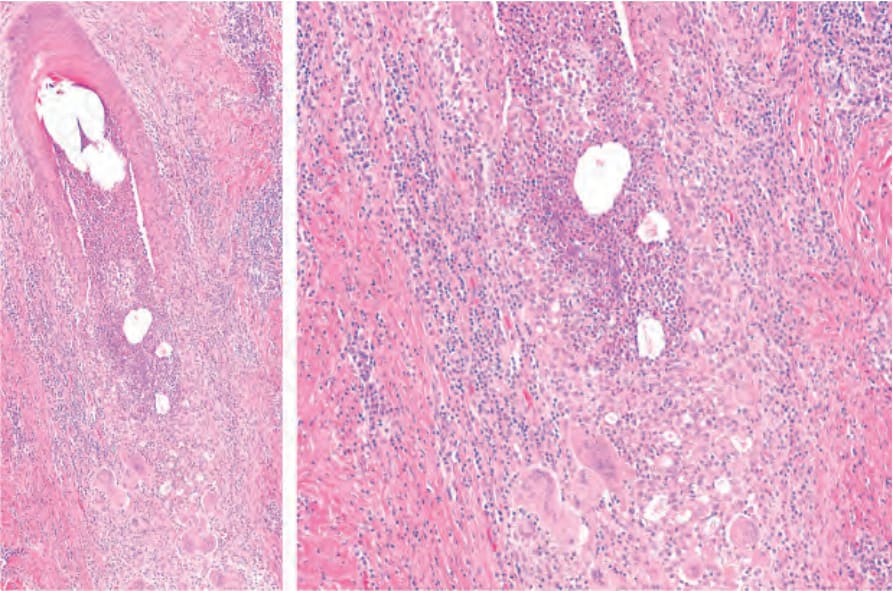
圖 22-118:脫髮性毛囊炎 (folliculitis decalvans):毛囊已破裂,毛囊內的嗜中性球溢入真皮,誘發強烈的肉芽腫性發炎反應。 (Folliculitis decalvans)
Fig. 22.118 Folliculitis decalvans: the hair follicle has ruptured and the intrafollicular neutrophils spill into the dermis inducing a strong granulomatous inflammatory response.
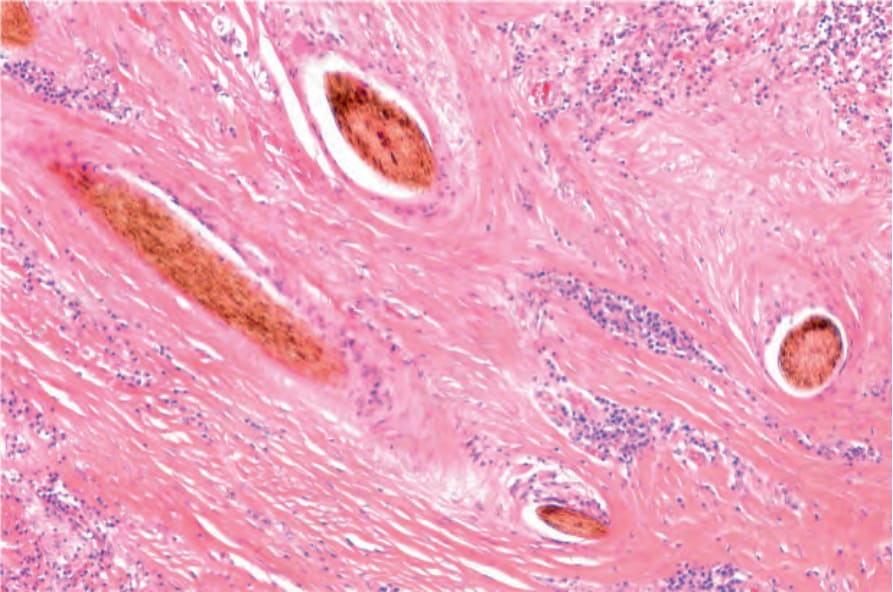
圖 22-119:頸部瘢痕疙瘩性痤瘡 (acne keloidalis nuchae)。真皮中多根游離毛幹,被緻密瘢痕所環繞。 (Acne keloidalis nuchae)
Fig. 22.119 Acne keloidalis nuchae. Multiple free hair shafts in the dermis surrounded by dense scarring.
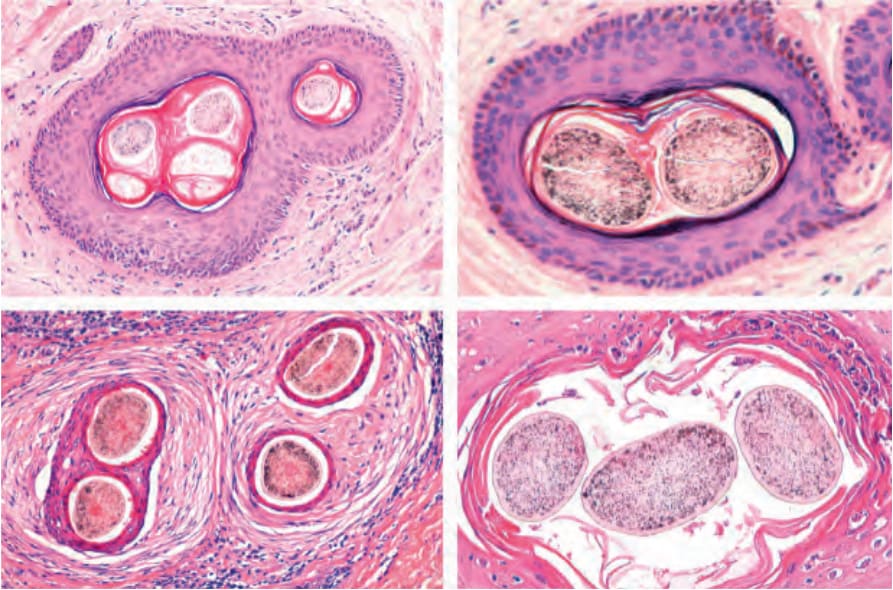
圖 22-120:複合毛囊 (compound follicles)。上方圖:正常複合毛囊於毛漏斗 (infundibulum) 層作橫向切片。注意顆粒細胞層及不明顯的毛囊周圍纖維層與極少量的淋巴球浸潤。下方圖:瘢痕性禿髮中的複合毛囊。於峽部 (isthmus) 層作水平切片。有廣泛的毛囊周圍纖維化與發炎浸潤。左下圖的毛囊來自一例頸部瘢痕疙瘩性痤瘡 (acne keloidalis nuchae),右圖的毛囊來自一例脫髮性毛囊炎 (folliculitis decalvans)。 (Compound follicles)
Fig. 22.120 Compound follicles. Upper panel, compound normal follicles transversally cut at the level of the infundibulum. Note the granular cell layer and discrete perifollicular fibrotic layer and minimal lymphocytic infiltrate. Lower panel, compound follicles in scarring alopecia. Horizontal sections at the level of the isthmus. There is extensive perifollicular fibrosis and an inflammatory infiltrate. The follicles on the left lower panel are from a case of acne keloidalis nuchae and those on the right panel from a case of folliculitis decalvans.
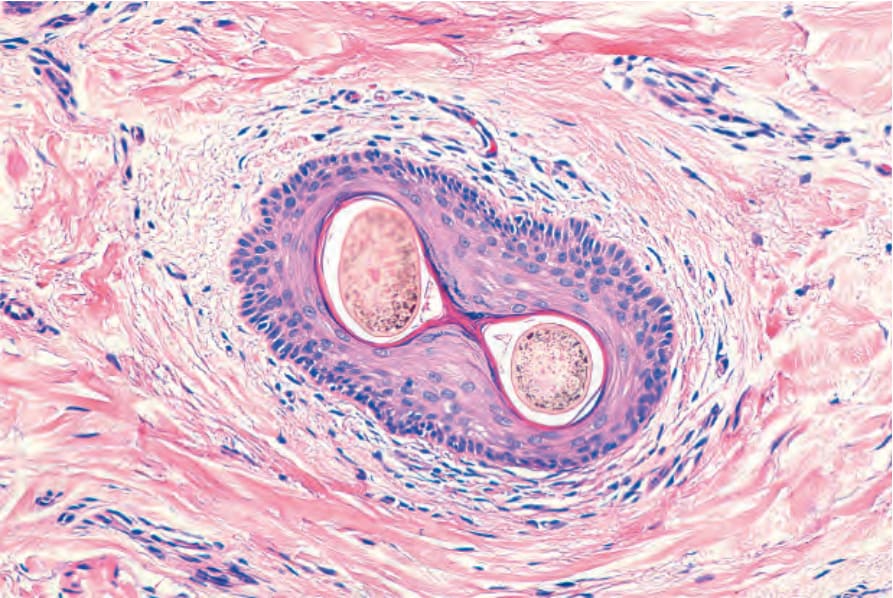
圖 22-17:毛漏斗 (infundibulum)。水平切片。其壁由鱗狀複層角化上皮 (squamous stratified keratinized epithelium) 構成。周圍真皮被一些淋巴球浸潤。有兩根毛幹由單一毛囊口 (ostium) 伸出。 (Infundibulum)
Fig. 22.17 Infundibulum. Horizontal section. The wall is made up of squamous stratified keratinized epithelium. The surrounding dermis is infiltrated by some lymphocytes. There are two hair shafts emerging from a single ostium.
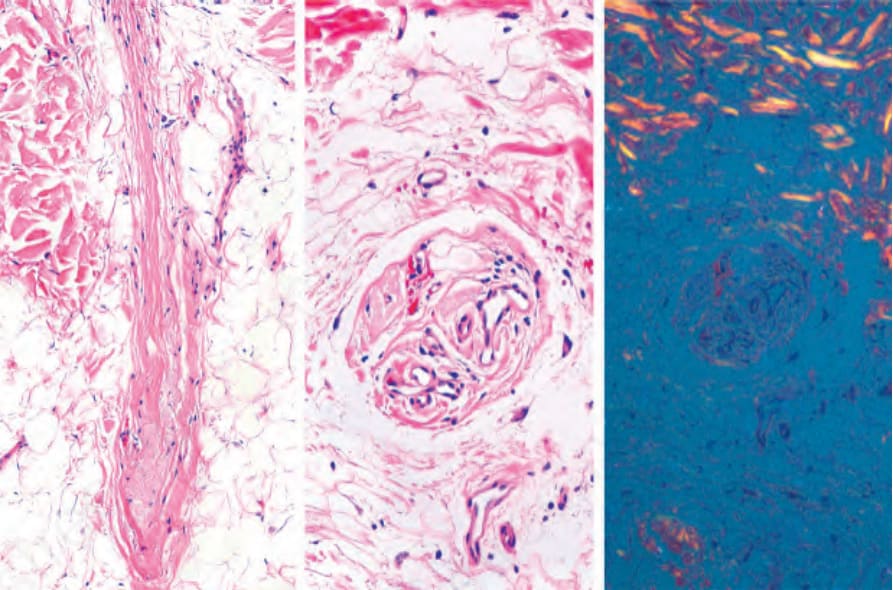
圖 22-34:毛囊星狀體 (follicular stella):注意垂直與水平切片中由膠原纖維 (collagen fibers)、纖維母細胞 (fibroblasts) 及血管組成的纖維血管性星狀體。膠原纖維之間可見彈性變性物質 (elastotic material)。在偏振光下,毛囊星狀體無雙折射 (birefringence)。 (Follicular stella)
Fig. 22.34 Follicular stella: note the fibrovascular stella composed of collagen fibers, fibroblasts, and blood vessels in vertical and horizontal sections. The elastotic material is apparent between the collagen fibers. With polarized light, there is no birefringence of the follicular stellae.
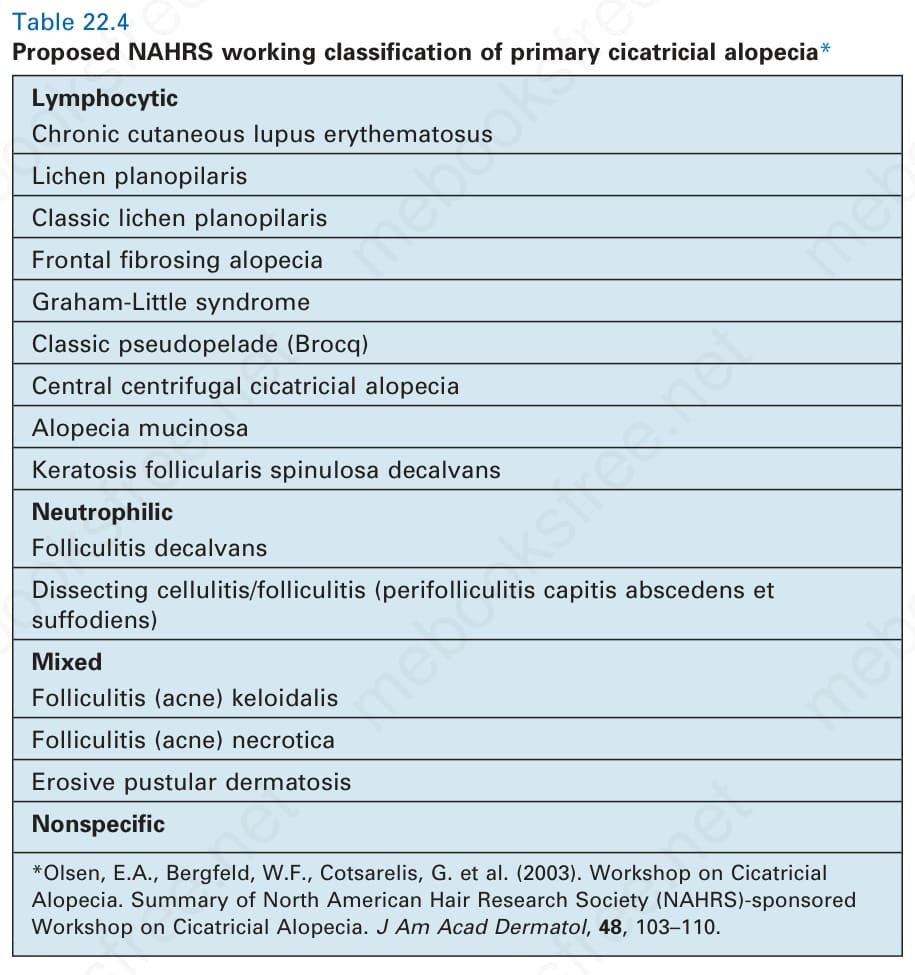
表 22-4:NAHRS 提議之原發性瘢痕性禿髮工作分類 (Proposed NAHRS working classification of primary cicatricial alopecia)。
Table 22.4 Proposed NAHRS working classification of primary cicatricial alopecia*
與紅斑性狼瘡 (lupus erythematosus) 相關的禿髮可表現為非瘢痕性與瘢痕性兩種形式。非瘢痕性形式有兩種變異型:第一種顯示與常見休止期落髮 (common telogen effluvium) 相似的臨床與組織學特徵,而第二種則表現為斑塊狀毛髮脫落區域,可模擬圓禿 (alopecia areata) 或梅毒性禿髮 (syphilitic alopecia),發生於通常患有嚴重 SLE 的患者。臨床上,受侵犯區域有時可見紅斑與水腫。當原發疾病獲得治療時,這兩種非瘢痕性禿髮變異型是可逆的。紅斑性狼瘡相關禿髮的瘢痕性形式典型見於盤狀變異型 (discoid variant) 患者,並常發生於成人,尤其是女性。雖然它亦可能發生於 SLE,但此屬罕見。頭皮侵犯與其他部位所見相似,包括紅斑、萎縮、毛囊角栓 (follicular plugging)、過度與低度色素沉著,以及毛髮脫落(圖 22.121)。與其他類型的瘢痕性禿髮相反,這些變化同時見於病灶的周邊與中央(圖 22.122)。病灶可為單發或多發、小型或融合性大斑塊,可能進行性侵犯頭皮的廣泛區域(圖 22.123)。
慢性皮膚紅斑性狼瘡 (Chronic cutaneous lupus erythematosus)(盤狀紅斑性狼瘡,discoid lupus erythematosus)
臨床特徵 (Clinical features) 約 30–50% 的盤狀紅斑性狼瘡 (discoid lupus erythematosus) 患者有頭皮侵犯。女性比男性更常受侵犯,且本病罕見進展為 SLE。SLE 患者約 70% 的病例有皮膚侵犯。其中,高比例在病程中顯示某種程度的頭皮侵犯伴禿髮。
1094 Diseases of the hair
隨著疾病進展,與 pseudopélade of Brocq 及 lichen planopilaris 的相似性變得更為顯著(圖 22.124)。Discoid lupus erythematosus 可能在無頭皮侵犯的情況下,表現為眉毛或睫毛脫落(madarosis)。在 discoid lupus erythematosus 患者中,圓禿 (alopecia areata) 的發生率增加,而在長期病程中,鱗狀細胞癌 (squamous cell carcinoma) 罕見地可能隨之發生。
紅斑性狼瘡對頭皮的侵犯同等地影響毛囊與真皮-表皮交界處 (dermal–epidermal junction) 的表皮。因此,垂直切片在本病的組織學研究中較受偏好。然而,若能取得兩處切片,則組合垂直與水平切片以供組織學判讀,以及直接免疫螢光 (direct immunofluorescence),是最理想的。
一種罕見形式的狼瘡脂膜炎 (lupus panniculitis),侵犯毛囊的下部,以及一種類似圓禿的短暫性禿髮形式,曾被記載。另一種罕見形式的線狀禿髮 (linear alopecia),與深部紅斑性狼瘡 (lupus erythematosus profundus) 相關且沿 Blaschko 線 (lines of Blaschko) 分布,亦已被認識。Lipedematous alopecia 曾與 discoid lupus erythematosus 相關聯。本病亦曾與慢性肉芽腫病 (chronic granulomatous disease)、frontal fibrosing alopecia、Parry-Romberg syndrome 及皮角 (cutaneous horns) 相關聯。
致病機轉與組織學特徵 (Pathogenesis and histologic features) 侵犯頭皮之狼瘡的致病機轉與發生於身體其他部位者相同。最適切的切片部位最好透過受侵犯頭皮區域的皮膚鏡 (dermoscopy) 來選擇。
紅斑性狼瘡禿髮的組織學外觀與其臨床形式同樣多樣。
在非瘢痕性變異型中,慢性休止期落髮樣 (chronic telogen effluvium-like) 形式顯示與常見休止期落髮相同的特徵。切片與毛髮圖 (trichogram) 兩者皆顯示休止期 (telogen) 毛囊數目的淨增加。
在斑塊狀禿髮的變異型中,組織學發現與圓禿及梅毒性禿髮所見者非常相似,惟在紅斑性狼瘡中發炎浸潤通常更為顯著且深層(圖 22.125)。此外,更典型於紅斑性狼瘡的其他發現,包括真皮黏液蛋白沉積 (dermal mucin deposition) 與毛囊上皮的局灶性水腫變性 (hydropic degeneration),常存在。患有全身性疾病之患者的診斷一般很直接,因為全身性疾病的症狀與徵象以及典型的實驗室發現通常很明顯。
1095 Scarring alopecias
A
B
膜,以 PAS 染色(加或不加 diastase)凸顯、微血管擴張及水腫(圖 22.129)。毛囊深部纖維性星狀體 (fibrous stellae) 內有時可見發炎浸潤,模擬圓禿與梅毒性禿髮。
在瘢痕性變異型中,顯微鏡下發現與發生於他處的皮膚盤狀狼瘡 (cutaneous discoid lupus) 所見差異甚微。然而,毛囊周圍發炎的程度往往比其他皮膚部位的盤狀病灶所見更為強烈(圖 22.126,見圖 22.7)。在某些病例中,可能有強烈的基底細胞水腫變性 (hydropic degeneration) 伴極少發炎,而在其他病例中,其特徵則為典型的苔癬樣皮膚炎 (lichenoid dermatitis)(圖 22.127)。膠樣小體 (colloid bodies) 常存在,但較 lichen planopilaris 為少。黏液蛋白的存在及血管周圍或附屬器周圍 (periadnexal) 位置的漿細胞 (plasma cells) 浸潤,是強烈指向 discoid lupus erythematosus 診斷的線索(圖 22.128)。其他亦可見的組織學特徵包括表皮萎縮伴過度角化與毛囊角栓、基底
如其他瘢痕性禿髮的典型表現,盤狀狼瘡的發炎細胞浸潤特別顯著於毛囊中段、皮脂腺層,皮脂腺最終消失(圖 22.130)。此位置之所以重要,是因為所造成的幹細胞數目減少。然而,在長期病灶中,發炎細胞浸潤可能幾乎完全消失,僅留下纖維化與萎縮(圖 22.131)。在這些病例中,彈性纖維染色將凸顯真皮廣泛瘢痕區域內彈性組織的喪失,以及環繞纖維束的彈性鞘 (elastic sheath) 的破壞(見圖 22.114)。
鑑別診斷 (Differential diagnosis) 兩個最重要的鑑別診斷包括 lichen planopilaris 與 pseudopélade of Brocq。
臨床上,在 lichen planopilaris 中過度角化病灶位於禿髮區域的周邊,相對於紅斑性狼瘡
1096 Diseases of the hair
則由 IgG、C3 及 C1q 的顆粒狀沉積構成,位於基底膜層,同時見於真皮-表皮交界處與毛囊上皮和真皮間的交界處。陰性結果並不能完全排除 discoid lupus erythematosus 的可能性。在 lichen planopilaris 中,直接免疫螢光顯示球狀沉積,尤其是 IgM,位於毛囊上皮與真皮間的交界處,凸顯凋亡小體 (apoptotic bodies)。然而,沿毛囊基底膜區域的 Ig 線狀沉積亦可能可見。pseudopélade of Brocq 的直接免疫螢光通常為陰性。它很少顯示沿毛囊毛漏斗基底膜的細顆粒狀 IgM 沉積。最後,另一項可能有助於鑑別診斷的近期重要發現,是在 discoid lupus 中存在成群的 CD123+ 漿細胞樣樹突細胞 (plasmocytoid dendritic cells)(定義為至少五個細胞的聚集),而在 lichen planopilaris 中這些細胞則以單個間質細胞排列。
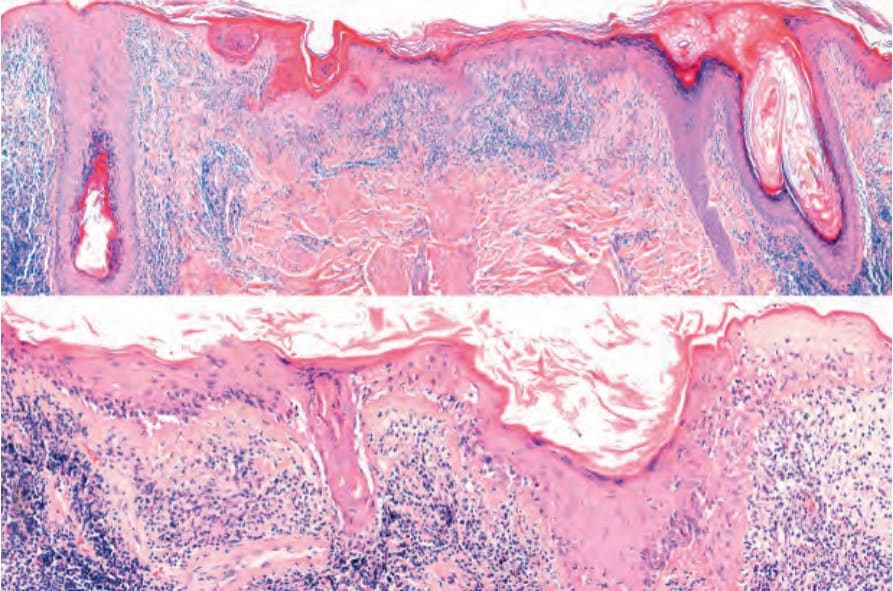
圖 22-7:頭皮切片,垂直切片。盤狀紅斑性狼瘡 (discoid lupus erythematosus):切片沿毛囊平面。真皮-表皮交界處增厚的基底膜清晰可見,發炎細胞浸潤的分布亦然。 (Discoid lupus erythematosus)
Fig. 22.7 Scalp biopsy, vertical section. Discoid lupus erythematosus: the section follows the plane of the hair follicles. The thickened basement membrane at the dermal– epidermal junction is clearly seen, as well as the distribution of the inflammatory cell infiltrate.
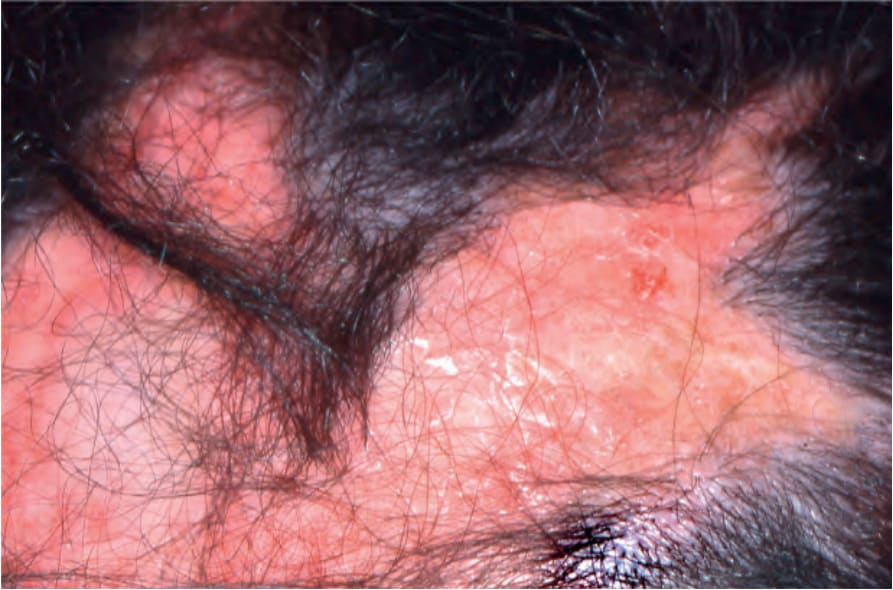
圖 22-121:盤狀紅斑性狼瘡 (discoid lupus erythematosus):注意紅斑、脫屑、毛囊角栓 (follicular plugging) 與瘢痕性禿髮。Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France。 (Discoid lupus erythematosus)
Fig. 22.121 Discoid lupus erythematosus: note the erythema, scaling, follicular plugging and scarring alopecia. Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.

圖 22-122:盤狀紅斑性狼瘡 (discoid lupus erythematosus)。在此禿髮斑塊中,發炎活動同時存在於周邊與中央,並有結痂與紅斑。Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia。 (Discoid lupus erythematosus)
Fig. 22.122 Discoid lupus erythematosus. In this plaque, of alopecia, inflammatory activity is present at the periphery as well as in the center and there is crusting and erythema. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
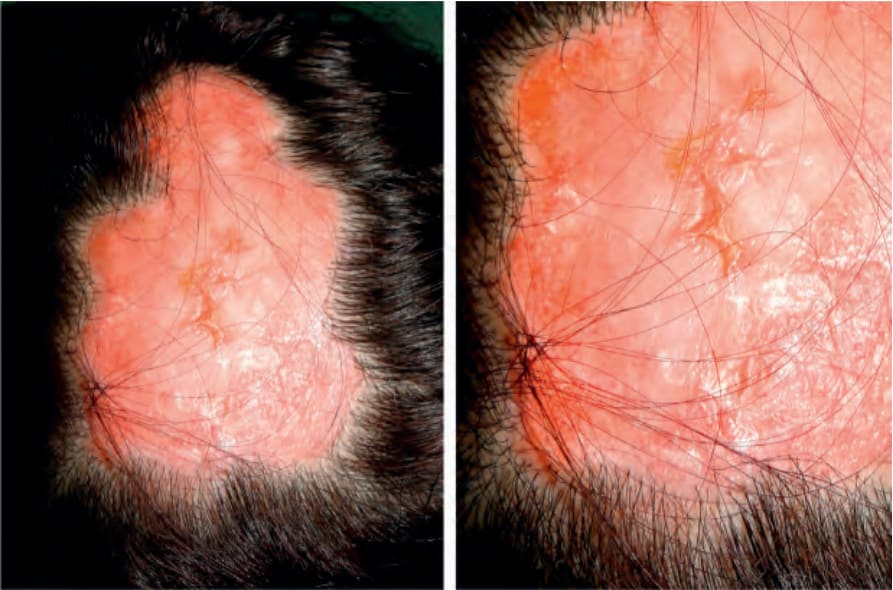
圖 22-123:盤狀紅斑性狼瘡 (discoid lupus erythematosus):頂間區域的大型紅斑性斑塊,伴有微血管擴張、瘢痕化、萎縮及毛髮喪失。Courtesy of C. Velázquez, MD, CES, Medellín, Colombia。 (Discoid lupus erythematosus)
Fig. 22.123 Discoid lupus erythematosus: large erythematous plaque with telangiectasia, scarring, atrophy, and loss of hair, in the interparietal area. Courtesy of C. Velázquez, MD, CES, Medellín, Colombia.

圖 22-124:盤狀紅斑性狼瘡 (discoid lupus erythematosus):萎縮性斑塊伴瘢痕化及毛髮喪失。Courtesy of A. Londoño, MD, CES, Medellín, Colombia。 (Discoid lupus erythematosus)
Fig. 22.124 Discoid lupus erythematosus: atrophic plaque with scarring, and loss of hair. Courtesy of A. Londoño, MD, CES, Medellín, Colombia.
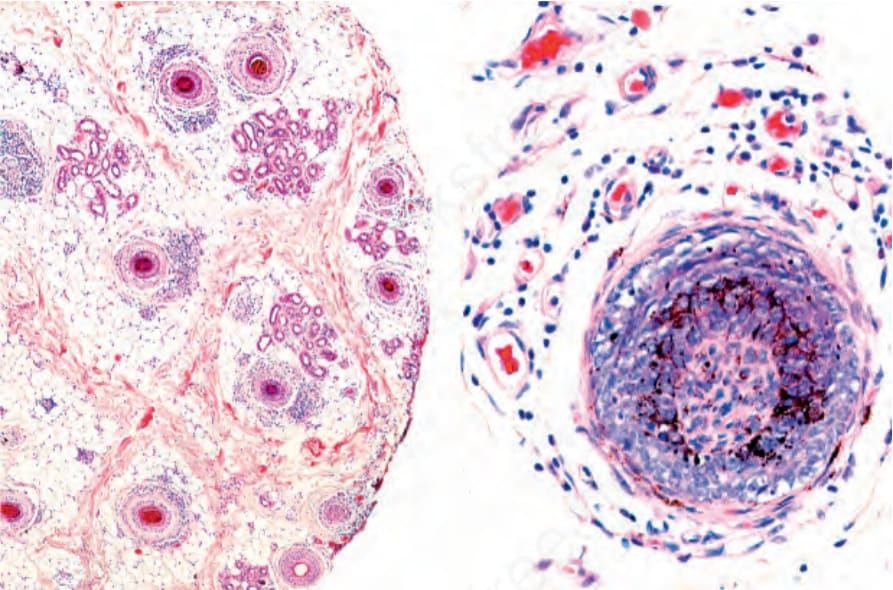
圖 22-125:盤狀紅斑性狼瘡 (discoid lupus erythematosus):局灶性禿髮變異型。環繞毛囊的發炎浸潤顯著。注意與圓禿或梅毒性禿髮的相似性。 (Discoid lupus erythematosus)
Fig. 22.125 Discoid lupus erythematosus: focal alopecia variant. The inflammatory infiltrate surrounding hair follicles is prominent. Note the similarity with alopecia areata or syphilitic alopecia.
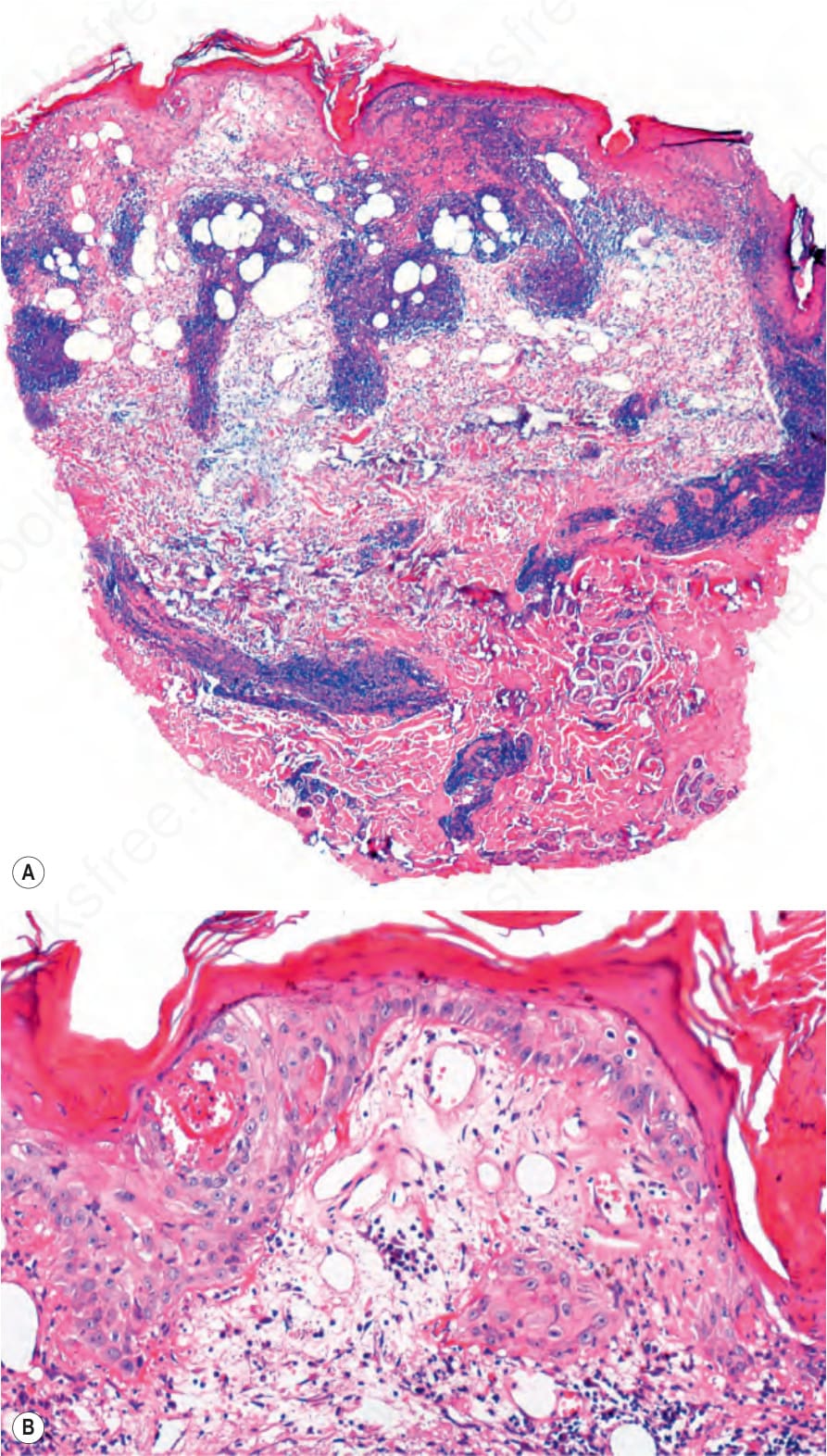
圖 22-126:盤狀紅斑性狼瘡 (discoid lupus erythematosus):(A) 所有毛囊與皮脂腺喪失,淺層與深層血管周圍有強烈的淋巴球浸潤;(B) 表皮顯示毛漏斗擴張伴角質碎屑、過度角化。亦注意表皮萎縮、真皮水腫及微血管擴張。 (Discoid lupus erythematosus)
Fig. 22.126 Discoid lupus erythematosus: (A) there is loss of all the hair follicles and sebaceous glands with an intense lymphocytic infiltrate around superficial and deep blood vessels; (B) the epidermis shows dilated follicular infundibula with keratinous debris, hyperkeratosis. Also note epidermal atrophy, dermal edema, and telangiectasia.
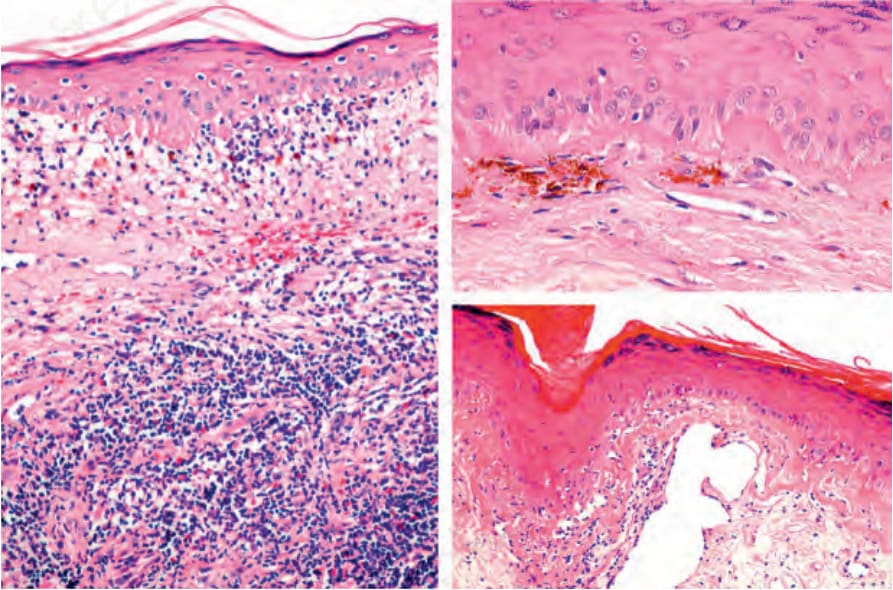
圖 22-127:盤狀紅斑性狼瘡 (discoid lupus erythematosus)。此影像顯示紅斑性狼瘡的典型組織學特徵。注意顯著的介面變化 (interface change) 與基底角質細胞 (basal keratinocytes) 的空泡變性 (vacuolar degeneration)。在真皮中,有單核發炎浸潤伴水腫。基底膜增厚。 (Discoid lupus erythematosus)
Fig. 22.127 Discoid lupus erythematosus. This image shows the typical histologic features of lupus erythematosus. Note the marked interface change and vacuolar degeneration of basal keratinocytes. In the dermis, there is a mononuclear inflammatory infiltrate with edema. The basement membrane is thickened.
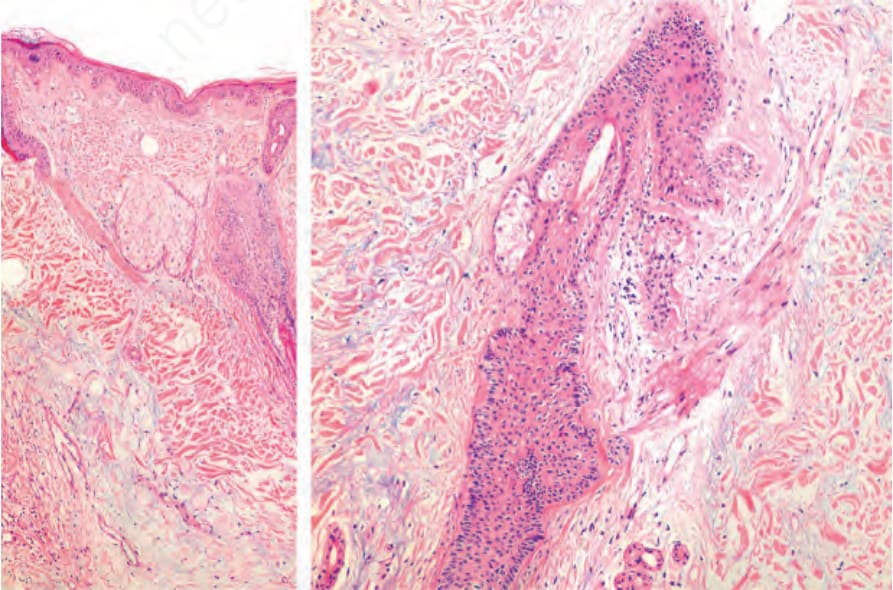
圖 22-128:腫脹性紅斑性狼瘡 (tumid lupus erythematosus):此例伴頭皮侵犯,真皮視野顯示豐富的黏液蛋白 (mucin)。 (Tumid lupus erythematosus)
Fig. 22.128 Tumid lupus erythematosus: view of the dermis showing abundant mucin in this case with scalp involvement.
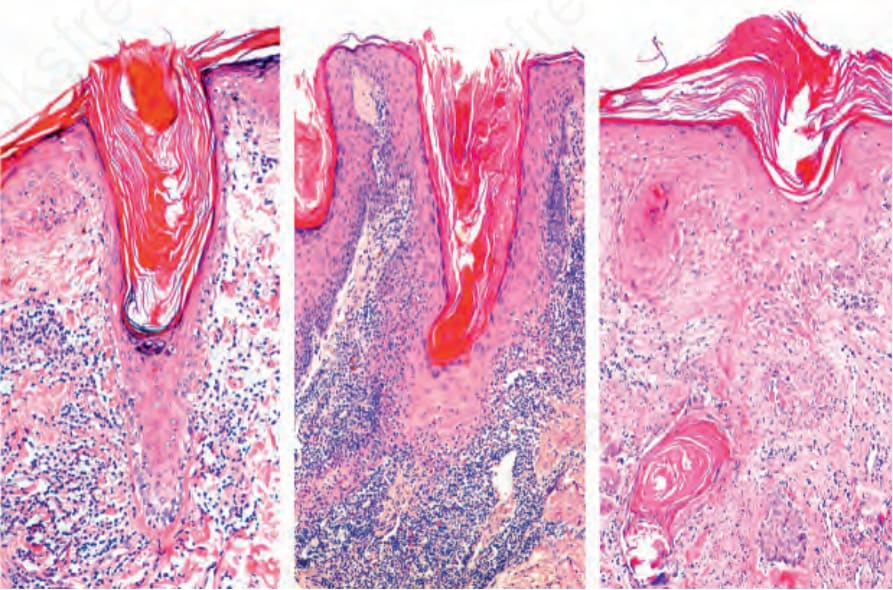
圖 22-129:盤狀紅斑性狼瘡 (discoid lupus erythematosus):毛囊角栓 (follicular plugging) 伴毛囊近乎完全的退化。乳頭層與上方網狀層真皮有硬化 (sclerosis)。 (Discoid lupus erythematosus)
Fig. 22.129 Discoid lupus erythematosus: follicular plugging with almost complete involution of the hair follicles. There is sclerosis of the papillary and upper reticular dermis.
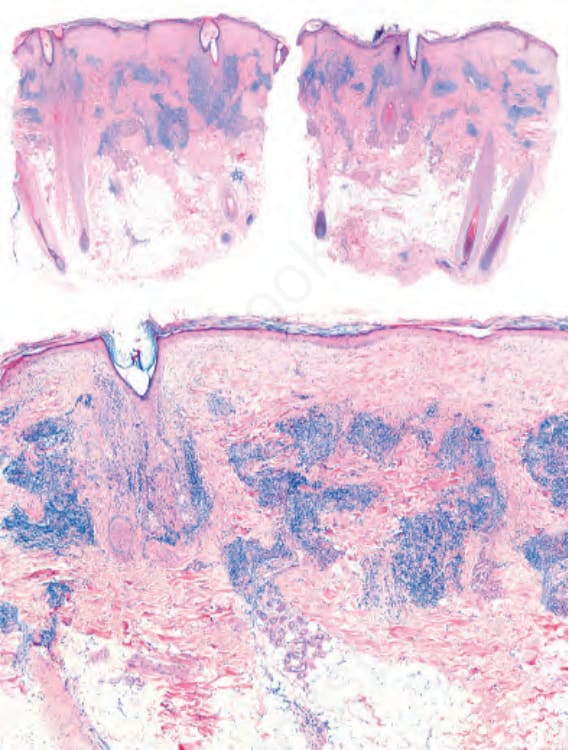
圖 22-130:盤狀紅斑性狼瘡 (discoid lupus erythematosus):顯著的發炎細胞浸潤位於毛囊上段周圍,亦位於血管周圍位置。 (Discoid lupus erythematosus)
Fig. 22.130 Discoid lupus erythematosus: Prominent inflammatory cell infiltrate located around the upper segment of the hair follicles and also in a perivascular location.
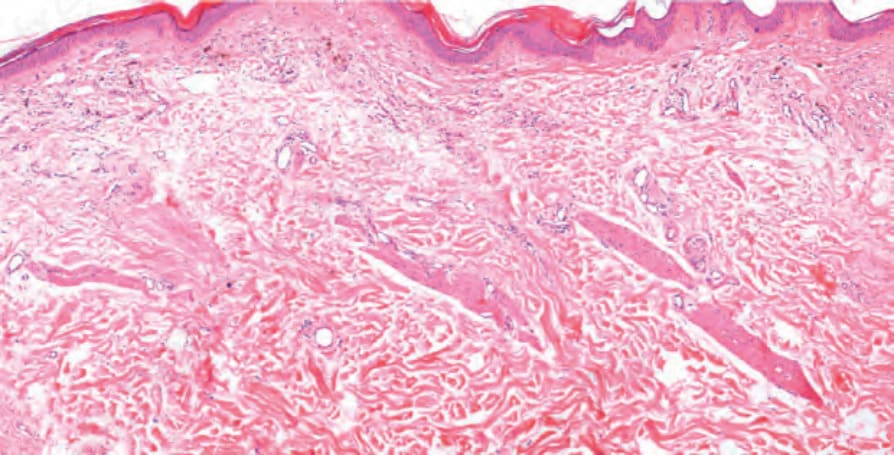
圖 22-131:盤狀紅斑性狼瘡 (discoid lupus erythematosus),晚期:毛囊已完全消失,留下毛囊星狀體 (follicular stellae) 與豎毛肌。在乳頭層真皮中有噬黑色素細胞 (melanophages),並明顯可見微血管擴張。發炎細胞浸潤極少。 (Discoid lupus erythematosus, late stage)
Fig. 22.131 Discoid lupus erythematosus, late stage: the hair follicles have completely disappeared, leaving follicular stellae and arrector pili muscles. In the papillary dermis, there are melanophages, and telangiectasia is evident. The inflammatory cell infiltrate is minimal.