Scarring alopecias
Scarring alopecias
The clinical appearance of lipedematous alopecia is characteristic. The hairs are thin, short, broken, and of less than 2 cm in length. A boggy and spongy thickened scalp is more evident on palpation than visually (Fig. 22.106). There may be pain and pruritus in the affected area. The diagnosis can be established by magnetic resonance imaging (MRI), computed tomography (CT) scan, and head ultrasound by demonstrating the irregular thickening of the subcutaneous tissue. The normal scalp thickness varies with age, between 4.8 ± 0.12 mm in women 20 to 39 years of age and 5.6 ± 0.15 mm in women 40 to 69 years of age.25 In lipedematous alopecia, the scalp thickness varied between 10 and 15 mm.16 With videodermoscopy, lipedematous scalp shows linear areas of telangiectasia within the scalp creases.9
A wide variety of follicular and nonfollicular scalp conditions including hereditary, developmental, and acquired disorders may result in scarring or permanent alopecia as a secondary phenomenon (Fig. 22.109).1 Permanent alopecia may also take place in the late stages of some nonscarring alopecias such as androgenetic alopecia, alopecia areata, psoriatic alopecia, and traction alopecia (‘transitional scarring or biphasic pattern’ alopecias).2,3
In this section, only those diseases that primarily affect the scalp or involve it secondarily with distinctive clinicopathological features will be described.
Scarring alopecia constitutes one of the most difficult and complex areas in the study of hair disease. It includes a wide variety of nosological entities
Pathogenesis and histologic features There has been speculation with regard to the role played by thickened adipose tissue, edema, and dilated lymphatic vessels in the development of hair loss. It has been speculated that obesity and hormonal factors may play a role as the majority of patients are women. Leptin may also play a role in the distribution of the fat tissue.26 At present, the exact pathogenesis of the disease is unknown.7,17
The scalp biopsy must be deep and include the whole thickness of the subcutaneous tissue, reaching the galea, as superficial biopsies may give a false impression of normality. The specimen must be processed with serial vertical sections. The histologic features consist of an increase of almost double the thickness of the scalp, with tissue edema, expansion of the subcutaneous fat, and infiltration of fat into the dermis (Fig. 22.107). In some cases, dilated lymphatic vessels have been observed.21 Mucin deposition is
1090 Diseases of the hair
(Fig. 22.110). The histopathological hallmark is usually the presence of an inflammatory infiltrate surrounding the bulge and isthmus and loss of sebaceous glands, later followed by the formation of a scar with the hair follicle being replaced by follicular fibrous tracts (Figs 22.111 and 22.112). These fibrous tracts clearly represent scarring and are different to the follicular stellae seen in androgenic alopecia and telogen effluvium. They extend from the epidermis to the deep dermis. They are easy to identify using polarized light (Fig. 22.113 and see Fig. 22.34).4 Histochemical stains including elastic stain and trichrome are useful to define the scarring areas and in the differential diagnosis with discoid lupus erythematosus, lichen planopilaris, and pseudopélade of Brocq (Fig. 22.114).1 Sometimes the only structure left of the hair follicle is the arrector pili muscle (Fig. 22.115).
with different etiologies and distinctive clinical features. However, the characteristic findings are usually only evident in the early stages, and as the disease progresses the clinical and pathological features of different diseases overlap, making categorization often impossible.
Scarring alopecias are characterized by irreversible loss and destruction of hair follicles and hair shafts. There is frequently, but not always, associated dermal fibrosis. Clinical examination reveals absence of follicular ostia (usually in a focal distribution), induration or atrophy of the skin, pigmentary alterations, follicular plugging, and occasionally, follicular pustules
From the point of view of clinical management, scarring alopecia represents a real ‘trichologic emergency’ because in a short period of time the hair follicles may be permanently destroyed.5 The resulting alopecia is irreversible and has a significant psychological impact. As the treatment is guided by the histopathologic findings, a scalp biopsy should be the first step in management.5,6
1091 Scarring alopecias
A
Scalp biopsies in cicatricial alopecia Scalp biopsy is the most important test to achieve the diagnosis in all cases of primary scarring alopecia. These should be taken from the active border. Multiple biopsies may be necessary to reach a definitive diagnosis. Ideally, vertical and horizontal sections should be examined stained with hematoxylin and eosin, PAS, and elastic tissue stains. The use of horizontal and vertical sections yields the higher results as it enables the pathologist to evaluate the type and location of the inflammatory infiltrate, the presence or absence of fibrosis, the morphology of the hair follicles, and their stage in the cycle (Fig. 22.116; see Fig. 22.112).7–9 In advanced cases in which only a scar without inflammatory infiltrate or hair follicles is present, direct immunofluorescence evaluation may be of great help in the differential diagnosis between discoid lupus erythematosus, lichen planopilaris, and pseudopélade of Brocq. For immunofluorescence studies, the second half of the punch biopsy submitted for vertical sections may be used (see Fig. 22.9).7,10,11
It is important not to forget that the evaluation of patients with scarring alopecia requires very close clinicopathological correlation, detailed clinical
B
history, and laboratory tests including serology for syphilis, direct Gram and PAS stains, and culture of the lesions.
Pathogenesis The pathophysiology of scarring is unclear and varies according to the different processes that result in permanent hair loss. However, some unifying generalizations concerning alterations on the stem cell-rich region in the bulge, the sebaceous gland, and the outer root sheath have emerged.12,13
1092 Diseases of the hair
In many of the diseases that cause scarring alopecia, the inflammatory infiltrate is concentrated around the upper part of the hair follicle, involving the bulge and, as a consequence, the stem cells (Fig. 22.117, see Fig. 22.111 and 22.112). This damages the regenerative capacity of the hair follicle. The damage may be physical or by inhibition of the function resulting in interference in the interaction between hair follicle mesenchymal cells and the bulge epithelium. The hair follicle cycle is abolished.14–16 The retained hair shaft bursts the bulb and lies free in the dermis, inducing a strong granulomatous inflammatory response with scarring (Figs 22.118 and 22.119). The only case in which the inflammatory infiltrate surrounds the bulge is in dissecting cellulitis of the scalp (perifolliculitis capitis abscedens et suffodiens), where the infiltrate is very deep at the limit between the dermis and the subcutaneous tissue.
Another common associated marker of scarring alopecia is early loss of sebaceous glands. This observation has been extensively studied in the asedia variant of mutant mice that lacks a gene to make sebum, has hypoplastic glands, and rapidly develops scarring alopecia.17–19 It appears therefore that the localization of the infiltrate at the upper part of the hair follicle, including the bulge, is crucial to the development of permanent damage.20,21,12
Lymphocytic Chronic cutaneous lupus erythematosus
Lichen planopilaris
Classic lichen planopilaris
Frontal fibrosing alopecia
Graham-Little syndrome
1093 Scarring alopecias
Classic pseudopelade (Brocq)
Central centrifugal cicatricial alopecia
Alopecia mucinosa
Keratosis follicularis spinulosa decalvans
Neutrophilic Folliculitis decalvans
Dissecting cellulitis/folliculitis (perifolliculitis capitis abscedens et suffodiens)
Mixed Folliculitis (acne) keloidalis
Folliculitis (acne) necrotica
Erosive pustular dermatosis
Nonspecific
*Olsen, E.A., Bergfeld, W.F., Cotsarelis, G. et al. (2003). Workshop on Cicatricial Alopecia. Summary of North American Hair Research Society (NAHRS)-sponsored Workshop on Cicatricial Alopecia. J Am Acad Dermatol, 48, 103–110.
Classification of scarring alopecias There are as many classifications of scarring alopecias as there are authors who have written about the subject.22
In view of the fact that many primary scarring alopecias have clinical and histologic features in common, distinction between different clinical variants is often very difficult. Due to this, it has been proposed that primary cicatricial alopecia be separated in groups (lymphocytic, neutrophilic, mixed, and non-specific), based on the type of infiltrate that predominates within and around the affected hair follicles (Table 22.4).8
This classification was proposed at the first consensus meeting on cicatricial alopecia held at Duke University in North Carolina (2001) by the North American Hair Research Society (NAHRS). It has gained wide acceptance and thus, it will be taken as the basis for this chapter.2,5,8,12,23–27
Lymphocyte-associated primary cicatricial alopecias This group of scarring alopecias is characterized by a lymphocyte infiltrate that always affects the superior segment of the follicle around the bulge. In general, the infiltrate does not change unless the follicle ruptures, giving place to a granulomatous reaction. There is loss of the sebaceous glands and fusion of hair follicles in numbers of two to a maximum of three. This fusion must be differentiated from that frequently observed in normal hair follicles at the infundibular level, hence the evaluation of a scarring alopecia must be done at the level of the isthmus or deeper (Fig. 22.120; see also Figs 22.17 and 22.46).1,2
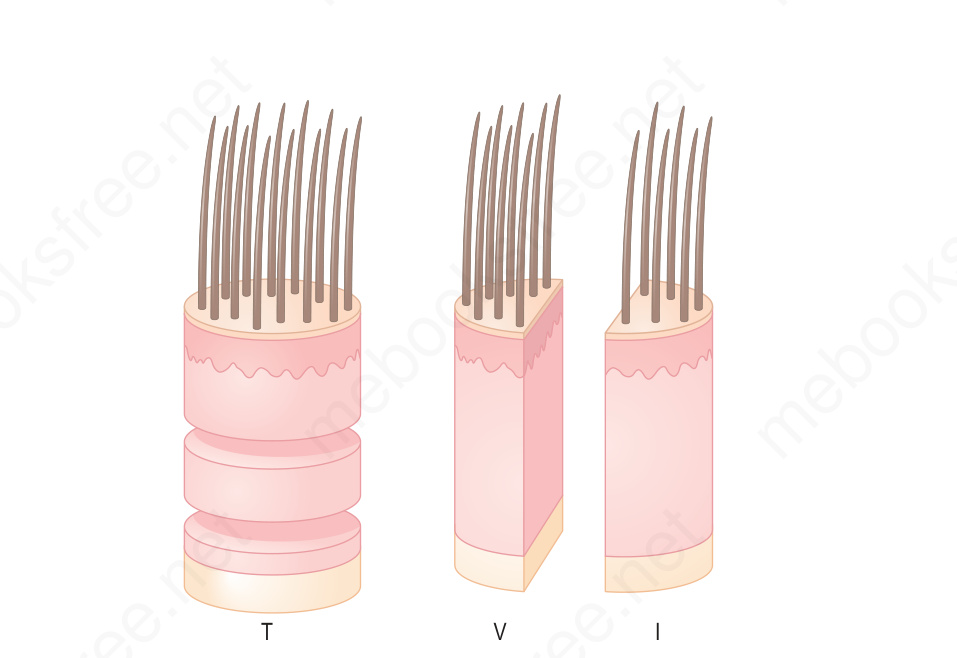
Fig. 22.9 Hair biopsy, transversal (T) and vertical (V) sections: ideally, two biopsies should be obtained. One of them is sectioned horizontally at different levels and the second can be vertically divided in two halves, one for routine histology and the other for immunofluorescence (I), electron microscopy, cultures and other techniques. Vertical sections are useful in cases that do not require comparison or follicle quantification; for example, in scarring alopecias. This type of sections must not be used in nonscarring alopecias, electron microscopy, cultures and other techniques. Vertical sections are useful in cases that do not require comparison or follicle quantification; for example, in scarring alopecias. This type of sections must not be used in nonscarring alopecias.
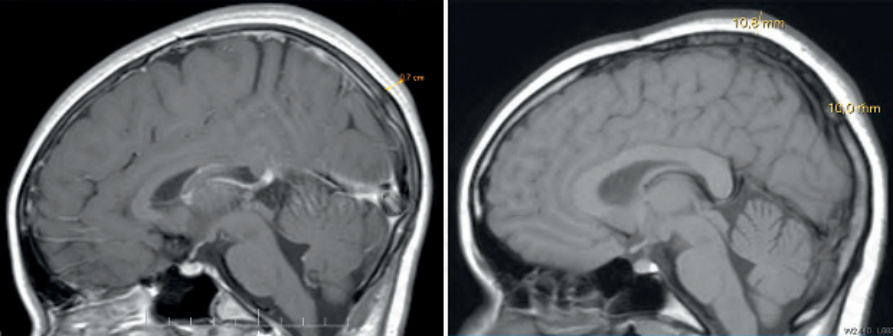
Fig. 22.106 Lipedematous alopecia: note the difference between the normal thickness of the scalp on the left and the increased thickness of the scalp on the right in a case of lipedematous alopecia. Courtesy of T. González, MD, CES, Medellín, Colombia.
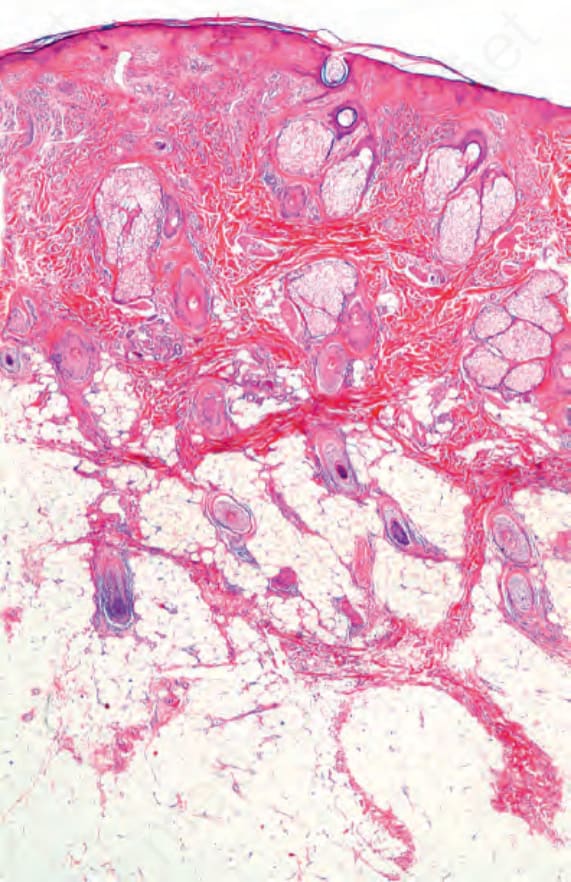
Fig. 22.107 Lipedematous alopecia. The subcutaneous tissue is thickened, in the absence of mucin deposition.

Fig. 22.108 Cutis verticis gyratum. Convoluted folds and furrows formed from thickened skin of the scalp in a cerebriform pattern. Courtesy of N. Valderrama, MD, Cali, Colombia.

Fig. 22.109 Scarring alopecia secondary to folliculotropic mycosis fungoides. There is total loss of hair in the occipital and posterior parietal regions. Courtesy of Y. Corredoira Salum, MD, Universidad de Chile, Santiago, Chile.
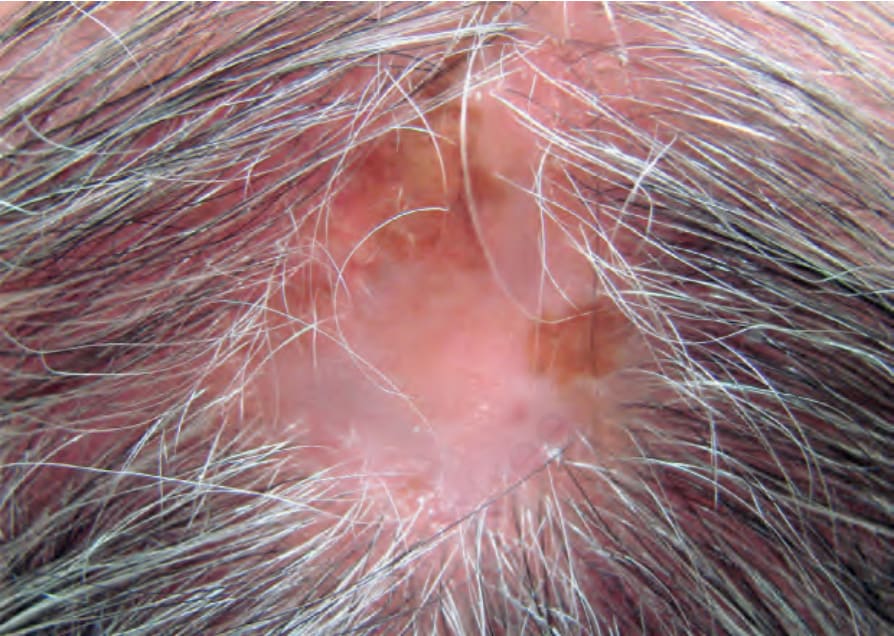
Fig. 22.110 Scarring alopecia, lichen planopilaris: there is a plaque of alopecia with hyper- and hypopigmentation, loss of follicular ostia, and follicular hyperkeratosis at the periphery. Courtesy of J. Gutiérrez, MD, Instituto de Ciencias de la Salud, Medellín, Colombia.
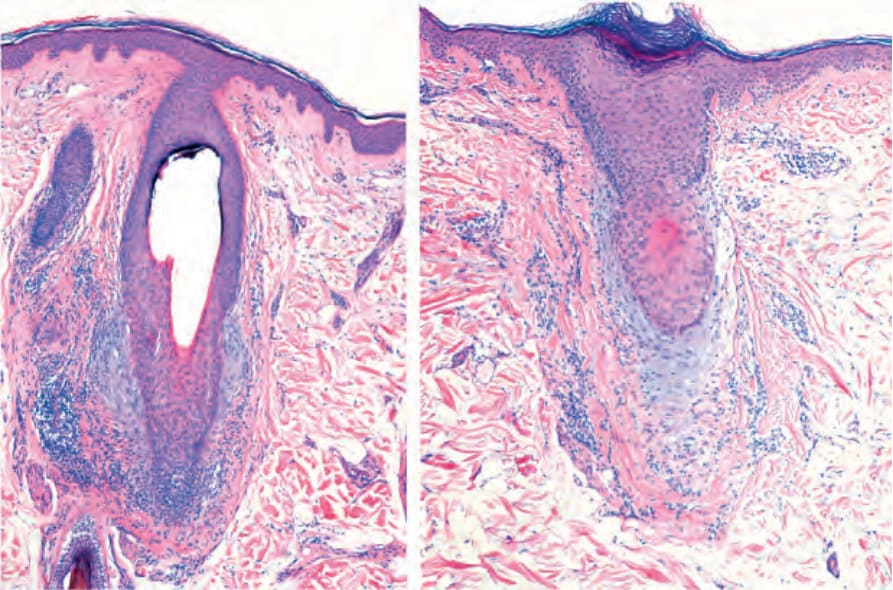
Fig. 22.111 Scarring alopecia, lichen planopilaris. Note the inflammatory infiltrate around the isthmus. There is perifollicular fibrosis, perifollicular mucin deposition and complete loss of sebaceous glands.
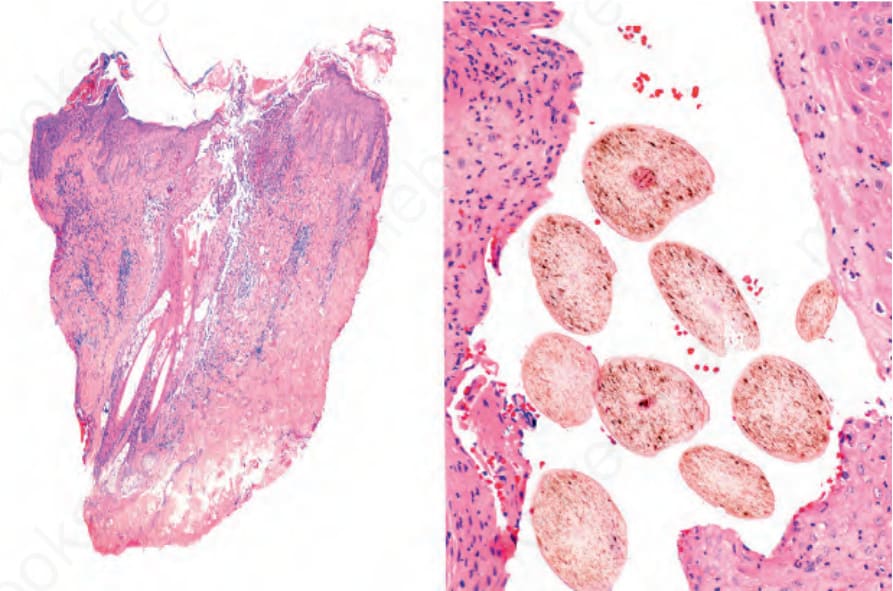
Fig. 22.112 Scarring alopecia, folliculitis decalvans. Vertical and horizontal sections. The destruction of hair follicles and sebaceous glands is associated with peri and interfollicular fibrosis. On the right side, fusion of follicles with numerous hair shafts associated with a single infundibulum (tufted folliculitis).
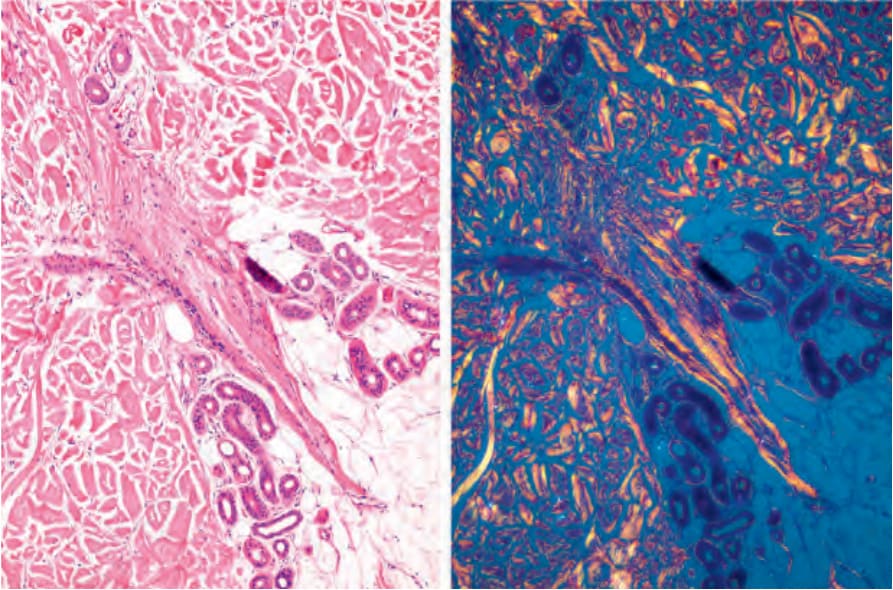
Fig. 22.113 Scarring alopecia, lichen planopilaris, follicular tracts. Note the birefringence of the collagen in the fibrous tract with polarized light.
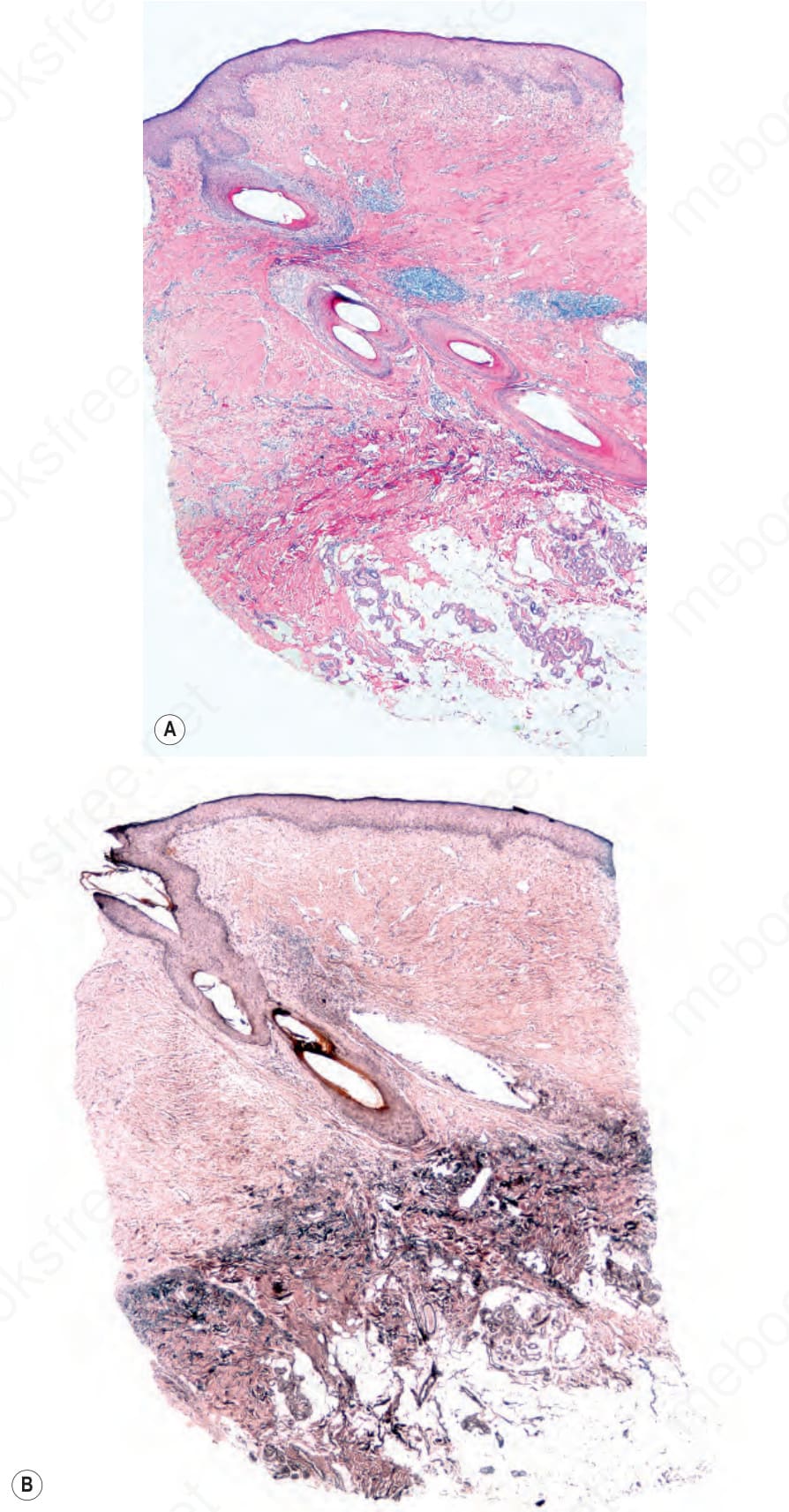
Fig. 22.114 Scarring alopecia, end-stage lupus erythematosus. (A) There are several fused follicles with an inflammatory cell infiltrate and absent sebaceous glands. (B) Elastic stain shows absence of staining in the dermis that surrounds the upper part of the hair follicle due to extensive loss of elastic fibers and scarring.
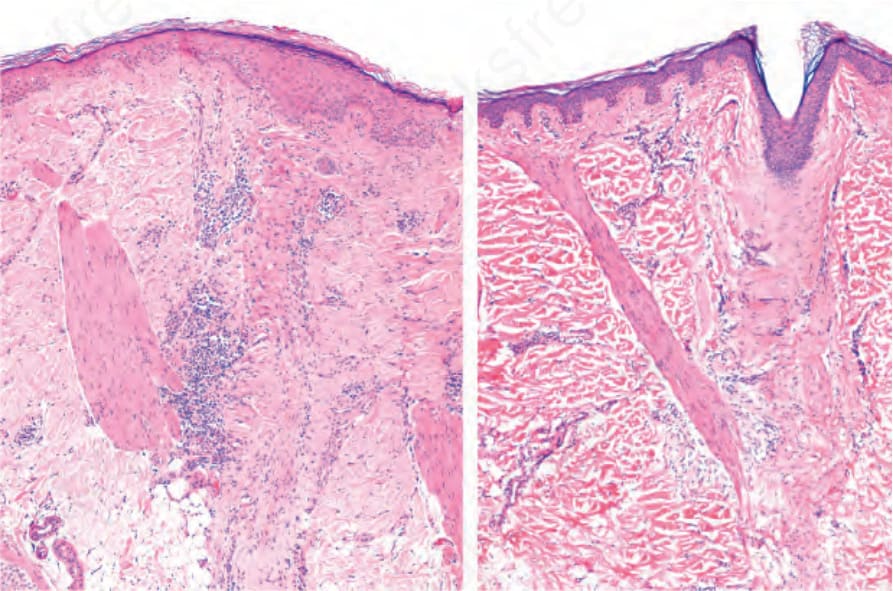
Fig. 22.115 Scarring alopecia, lichen planopilaris: the hair follicles have disappeared and been replaced by two vertical fibrous scars in which an arrector pili muscle is inserted.
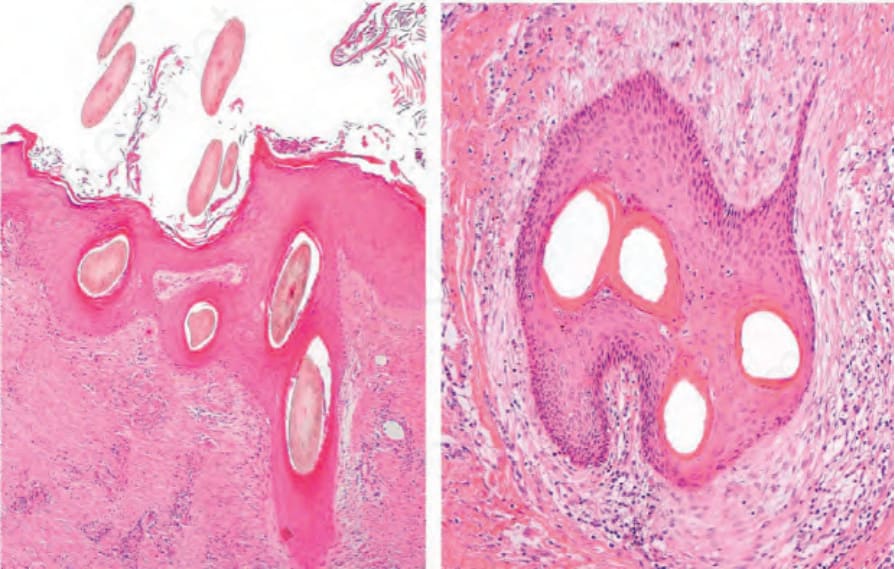
Fig. 22.116 Scarring alopecia, vertical and horizontal sections: this biopsy has been cut in two planes allowing a complementary view of tufted folliculitis (polytrichia) with hair follicle fusion into a single follicular structure which contains multiple hair shafts emerging at the surface through a single ostium.
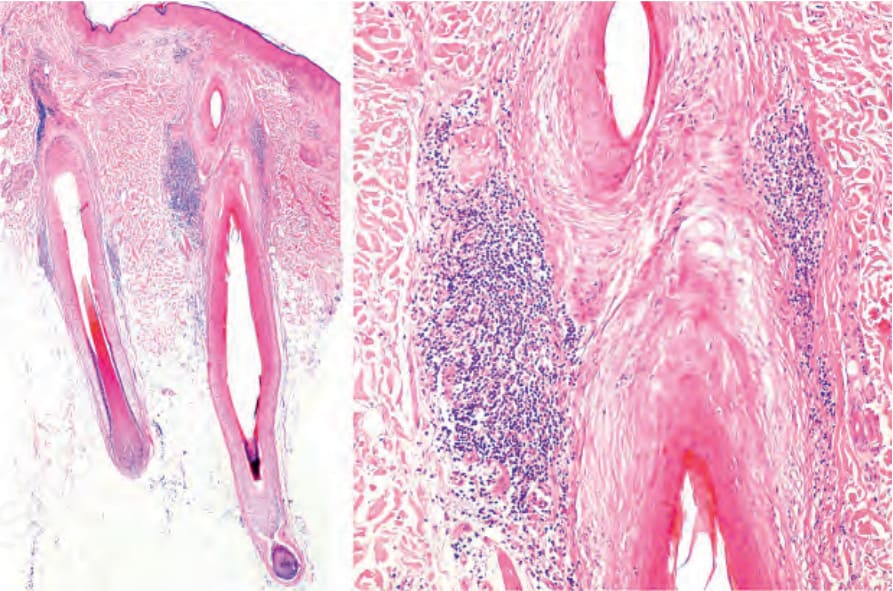
Fig. 22.117 Scarring alopecia, lichen planopilaris: note the lymphocytic infiltrate in the upper segment and in the area of insertion of the arrector pili muscle. In the figure on the right, note the loss of sebaceous glands and the premature shedding of the internal root sheath.
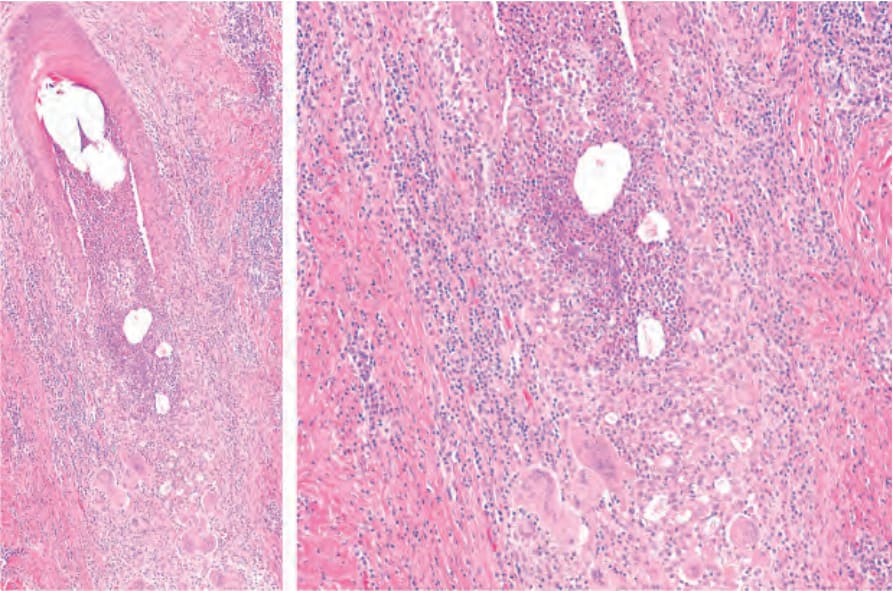
Fig. 22.118 Folliculitis decalvans: the hair follicle has ruptured and the intrafollicular neutrophils spill into the dermis inducing a strong granulomatous inflammatory response.
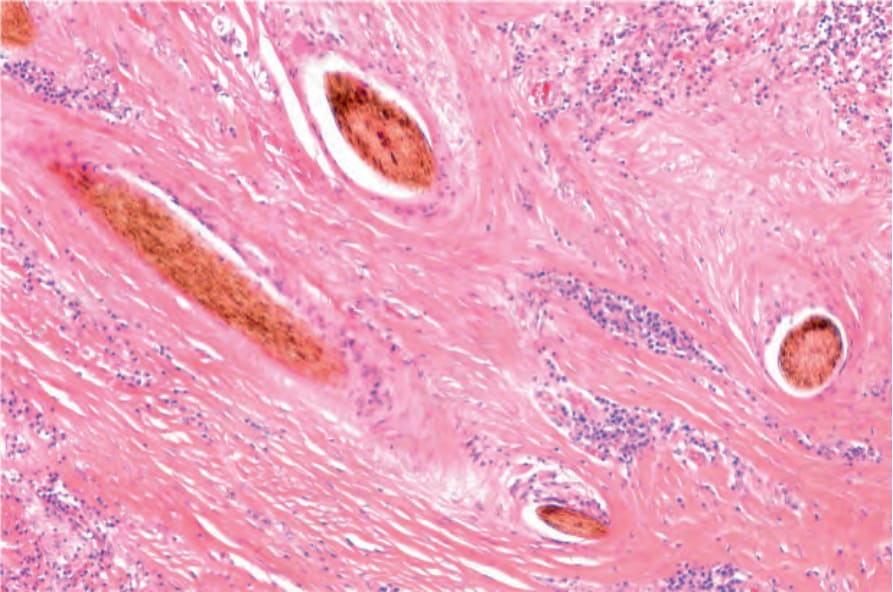
Fig. 22.119 Acne keloidalis nuchae. Multiple free hair shafts in the dermis surrounded by dense scarring.
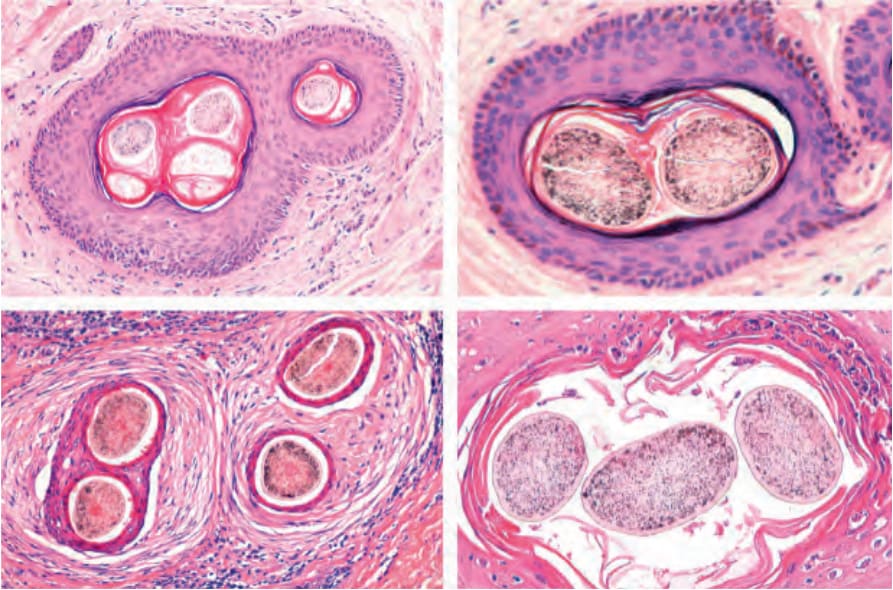
Fig. 22.120 Compound follicles. Upper panel, compound normal follicles transversally cut at the level of the infundibulum. Note the granular cell layer and discrete perifollicular fibrotic layer and minimal lymphocytic infiltrate. Lower panel, compound follicles in scarring alopecia. Horizontal sections at the level of the isthmus. There is extensive perifollicular fibrosis and an inflammatory infiltrate. The follicles on the left lower panel are from a case of acne keloidalis nuchae and those on the right panel from a case of folliculitis decalvans.
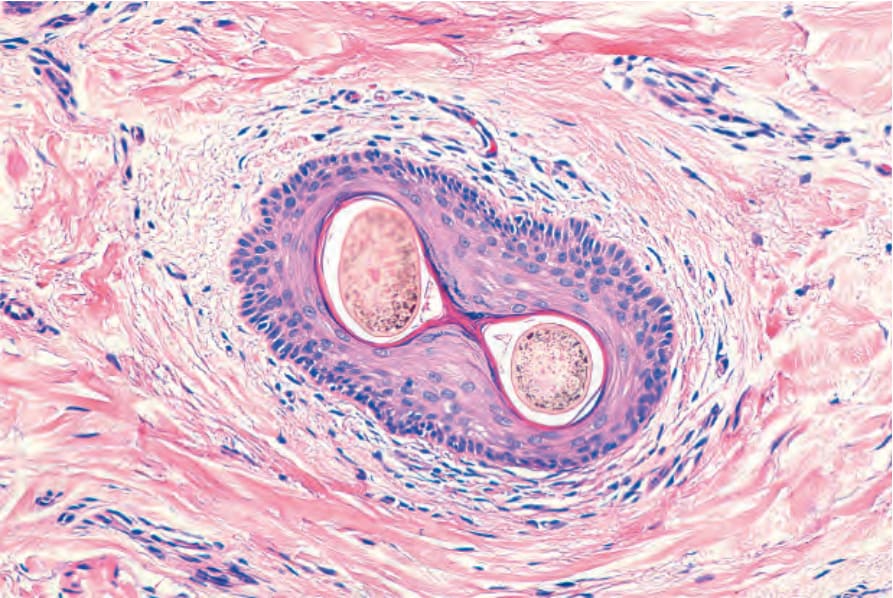
Fig. 22.17 Infundibulum. Horizontal section. The wall is made up of squamous stratified keratinized epithelium. The surrounding dermis is infiltrated by some lymphocytes. There are two hair shafts emerging from a single ostium.
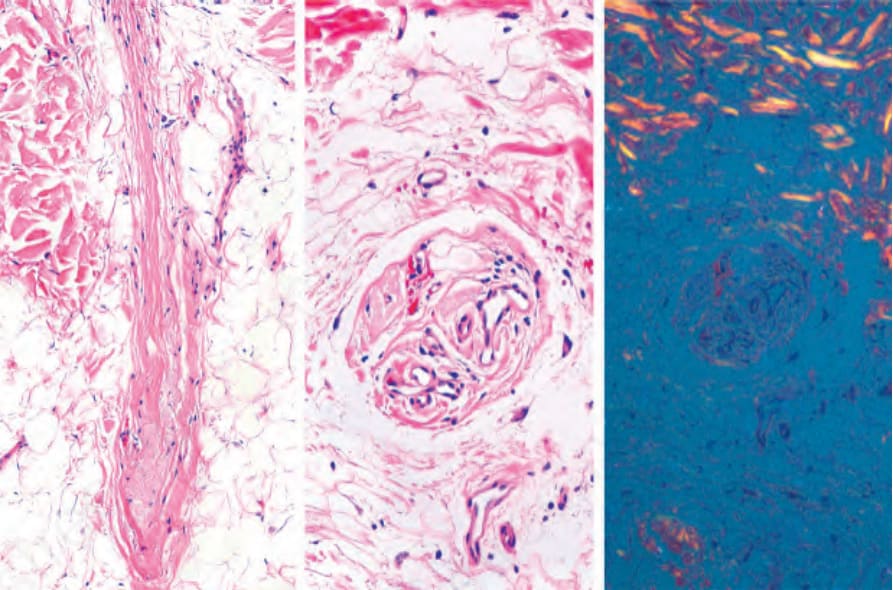
Fig. 22.34 Follicular stella: note the fibrovascular stella composed of collagen fibers, fibroblasts, and blood vessels in vertical and horizontal sections. The elastotic material is apparent between the collagen fibers. With polarized light, there is no birefringence of the follicular stellae.
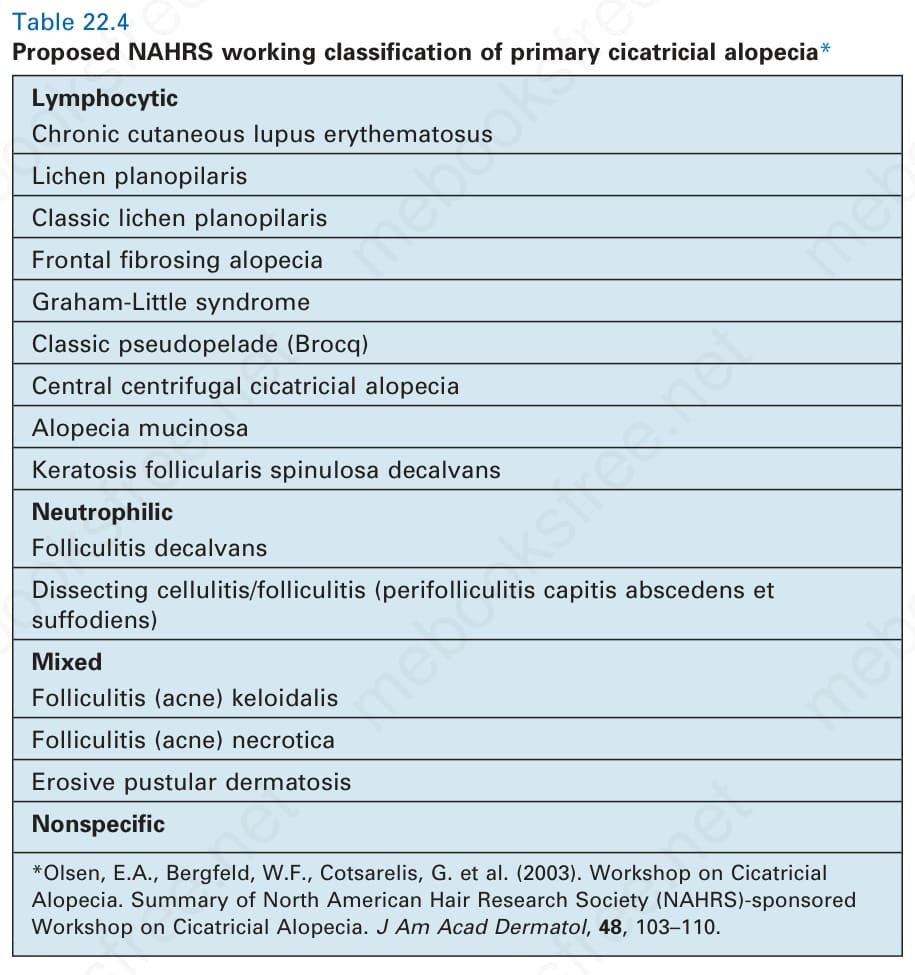
Table 22.4 Proposed NAHRS working classification of primary cicatricial alopecia*
The alopecia associated with lupus erythematosus may manifest as nonscarring and scarring forms. The nonscarring form has two variants: the first shows clinical and histologic features similar to those of common telogen effluvium,7 whereas the second presents with patchy areas of hair loss that can simulate alopecia areata or syphilitic alopecia and occurs in patients who usually have severe SLE.6,8 Clinically, erythema and edema in the involved areas are sometimes evident. These two nonscarring variants of alopecia are reversible when the primary illness is treated. The scarring form of lupus erythematosus-associated alopecia is typically seen in patients with the discoid variant and frequently occurs in adults, particularly women. Although it may also occur in SLE, this is infrequent. Scalp involvement is similar to that seen at other sites and consists of erythema, atrophy, follicular plugging, hyper- and hypopigmentation, and hair loss (Fig. 22.121). Contrary to other types of scarring alopecia, these changes are observed in both the periphery and the center of the lesion (Fig. 22.122).9 The lesions, which can be solitary or multiple, small or confluent large plaques, may progressively affect extensive areas of the scalp (Fig. 22.123).
Chronic cutaneous lupus erythematosus (discoid lupus erythematosus)
Clinical features About 30–50% of patients with discoid lupus erythematosus present with scalp involvement.1,2 Women are more frequently affected than men, and the disease rarely progresses to SLE.3 Patients with SLE have cutaneous involvement in approximately 70% of cases. Of these, a high percentage show some degree of scalp involvement with alopecia during the course of the illness.4–6
1094 Diseases of the hair
As the illness progresses, the similarity to pseudopélade of Brocq and lichen planopilaris becomes more pronounced (Fig. 22.124). Discoid lupus erythematosus may present with loss of the eyebrows or eyelashes (madarosis) in the absence of involvement of the scalp.10,11 In patients with discoid lupus erythematosus the incidence of alopecia areata is increased and, in longstanding disease, squamous cell carcinoma may rarely ensue.12,13
Scalp involvement by lupus erythematosus equally affects the hair follicle and the epidermis at the dermal–epidermal junction. For this reason, vertical sections are preferred in the histologic study of the condition. However, if two biopsies can be obtained, a combination of vertical and horizontal sections for histologic interpretation and direct immunofluorescence is ideal.22
A rare form of lupus panniculitis with involvement of the lower part of the hair follicle and a transitory form of alopecia similar to alopecia areata have been documented.14 Another rare form of linear alopecia related to lupus erythematosus profundus following the lines of Blaschko has been recognized.15 Lipedematous alopecia has been associated with discoid lupus erythematosus.16 The disease has also been associated with chronic granulomatous disease, frontal fibrosing alopecia, Parry-Romberg syndrome, and cutaneous horns.17–20
Pathogenesis and histologic features The pathogenesis of lupus affecting the scalp is identical to that occurring at other sites of the body. The most appropriate site for the biopsy is best selected through dermoscopy of the affected areas of the scalp.21
The histologic appearances of alopecia in lupus erythematosus are as varied as the clinical forms.
In the nonscarring variants, the chronic telogen effluvium-like form shows features identical to common telogen effluvium. The biopsy and trichogram both show a net increase in the number of telogen hair follicles.
In the variant with patchy alopecia, the histologic findings are very similar to those seen in alopecia areata and syphilitic alopecia except that the inflammatory infiltrate is generally more prominent and deep in lupus erythematosus (Fig. 22.125). Furthermore, other findings more typical of lupus erythematosus, including dermal mucin deposition and focal hydropic degeneration of the follicular epithelium, are often present.23,24 The diagnosis in patients with systemic disease is generally straightforward, as symptoms and signs of systemic disease and typical laboratory findings are usually evident.
1095 Scarring alopecias
A
B
membrane, highlighted with the PAS stain with or without diastase, telangiectasia, and edema (Fig. 22.129). An inflammatory infiltrate within the fibrous stellae deep to the hair follicles may sometimes be present simulating alopecia areata and syphilitic alopecia.
In the scarring variant, the microscopic findings differ little from those found in cutaneous discoid lupus presenting elsewhere. The degree of perifollicular inflammation, however, tends to be more intense than that seen in discoid lesions at other cutaneous sites (Fig. 22.126, see Fig. 22.7). In some cases, there may be intense hydropic degeneration of basal cells with minimal inflammation, whereas in others the features are those of a typical lichenoid dermatitis (Fig. 22.127). Colloid bodies are often present but they are less abundant than in lichen planopilaris. The presence of mucin and an infiltrate of plasma cells in a perivascular or periadnexal location are strong pointers toward a diagnosis of discoid lupus erythematosus (Fig. 22.128). Other histologic features that may also be seen include epidermal atrophy with hyperkeratosis and follicular plugging, thickening of the basement
As is typical of other scarring alopecias, the inflammatory cell infiltrate in discoid lupus is particularly prominent around the mid portion of the hair follicle at the level of the sebaceous glands, which eventually disappear (Fig. 22.130). The location is important because of the resulting reduction in the number of stem cells. Nevertheless, in longstanding lesions the inflammatory cell infiltrate may almost completely disappear, leaving only fibrosis and atrophy (Fig. 22.131).25 In these cases, staining for elastic fibers will underscore the loss of elastic tissue within the broad scarred areas of the dermis and destruction of the elastic sheath surrounding the fibrous tracts (see Fig. 22.114).26
Differential diagnosis The two most important differential diagnoses include lichen planopilaris and pseudopélade of Brocq.
Clinically, in lichen planopilaris hyperkeratotic lesions are located at the periphery of the areas of alopecia as opposed to lupus erythematosus where
1096 Diseases of the hair
consists of granular deposits of IgG, C3, and C1q at the level of the basement membrane, both at the dermal–epidermal junction and at the junction between the follicular epithelium and the dermis.31 A negative result does not completely exclude the possibility of discoid lupus erythematosus.32 In lichen planopilaris, direct immunofluorescence shows globular deposition, particularly of IgM at the junction between the follicular epithelium and the dermis, highlighting apoptotic bodies. Linear deposition of Ig along the follicular basement membrane region, however, may also be seen. Direct immunofluorescence in pseudopélade of Brocq is usually negative. It seldom shows finely granular IgM deposition along the follicular infundibular basement membrane.33,34 Finally, another recent important finding that may help in the differential diagnosis is the presence of groups of CD123+ plasmocytoid dendritic cells (defined as clusters of at least five cells) in discoid lupus whereas in lichen planopilaris these cells are arranged as single interstitial cells.35,36
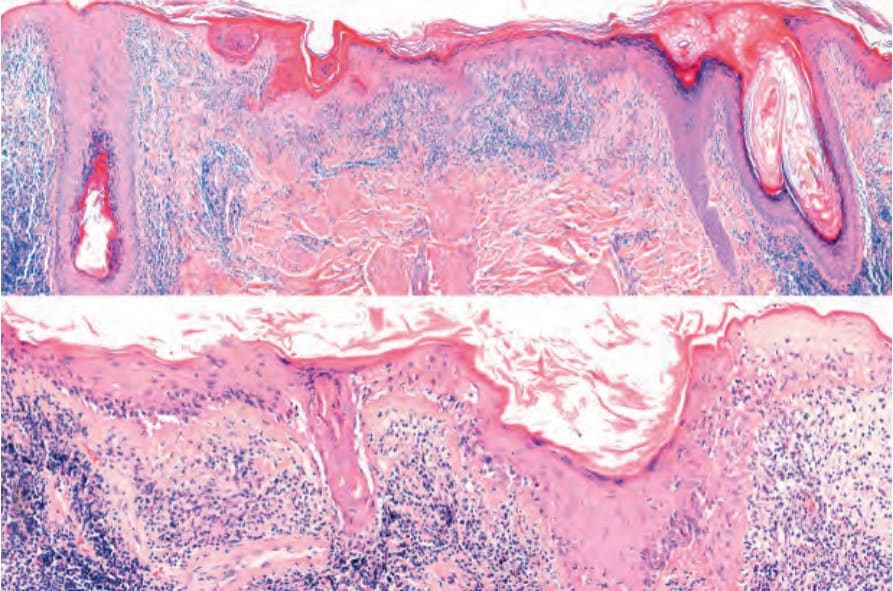
Fig. 22.7 Scalp biopsy, vertical section. Discoid lupus erythematosus: the section follows the plane of the hair follicles. The thickened basement membrane at the dermal– epidermal junction is clearly seen, as well as the distribution of the inflammatory cell infiltrate.
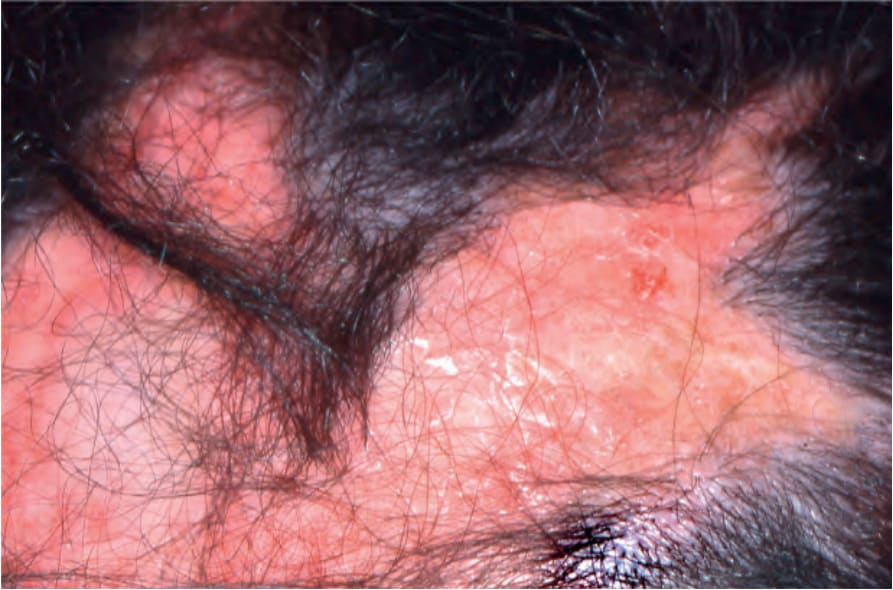
Fig. 22.121 Discoid lupus erythematosus: note the erythema, scaling, follicular plugging and scarring alopecia. Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.

Fig. 22.122 Discoid lupus erythematosus. In this plaque, of alopecia, inflammatory activity is present at the periphery as well as in the center and there is crusting and erythema. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
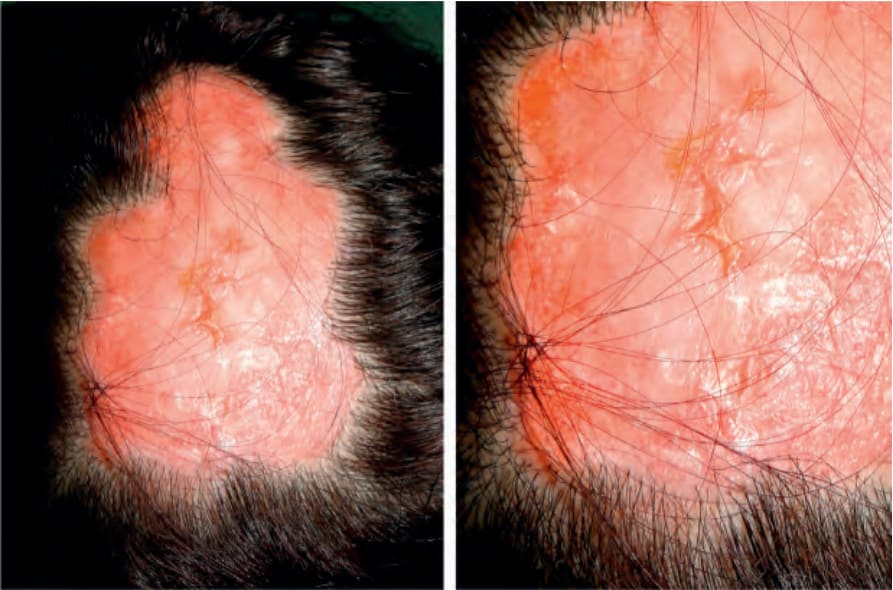
Fig. 22.123 Discoid lupus erythematosus: large erythematous plaque with telangiectasia, scarring, atrophy, and loss of hair, in the interparietal area. Courtesy of C. Velázquez, MD, CES, Medellín, Colombia.

Fig. 22.124 Discoid lupus erythematosus: atrophic plaque with scarring, and loss of hair. Courtesy of A. Londoño, MD, CES, Medellín, Colombia.
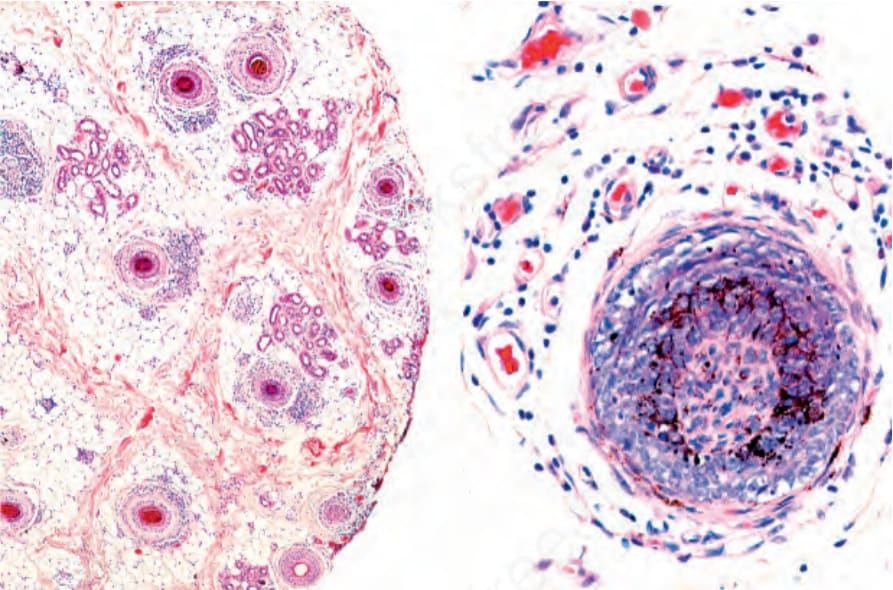
Fig. 22.125 Discoid lupus erythematosus: focal alopecia variant. The inflammatory infiltrate surrounding hair follicles is prominent. Note the similarity with alopecia areata or syphilitic alopecia.
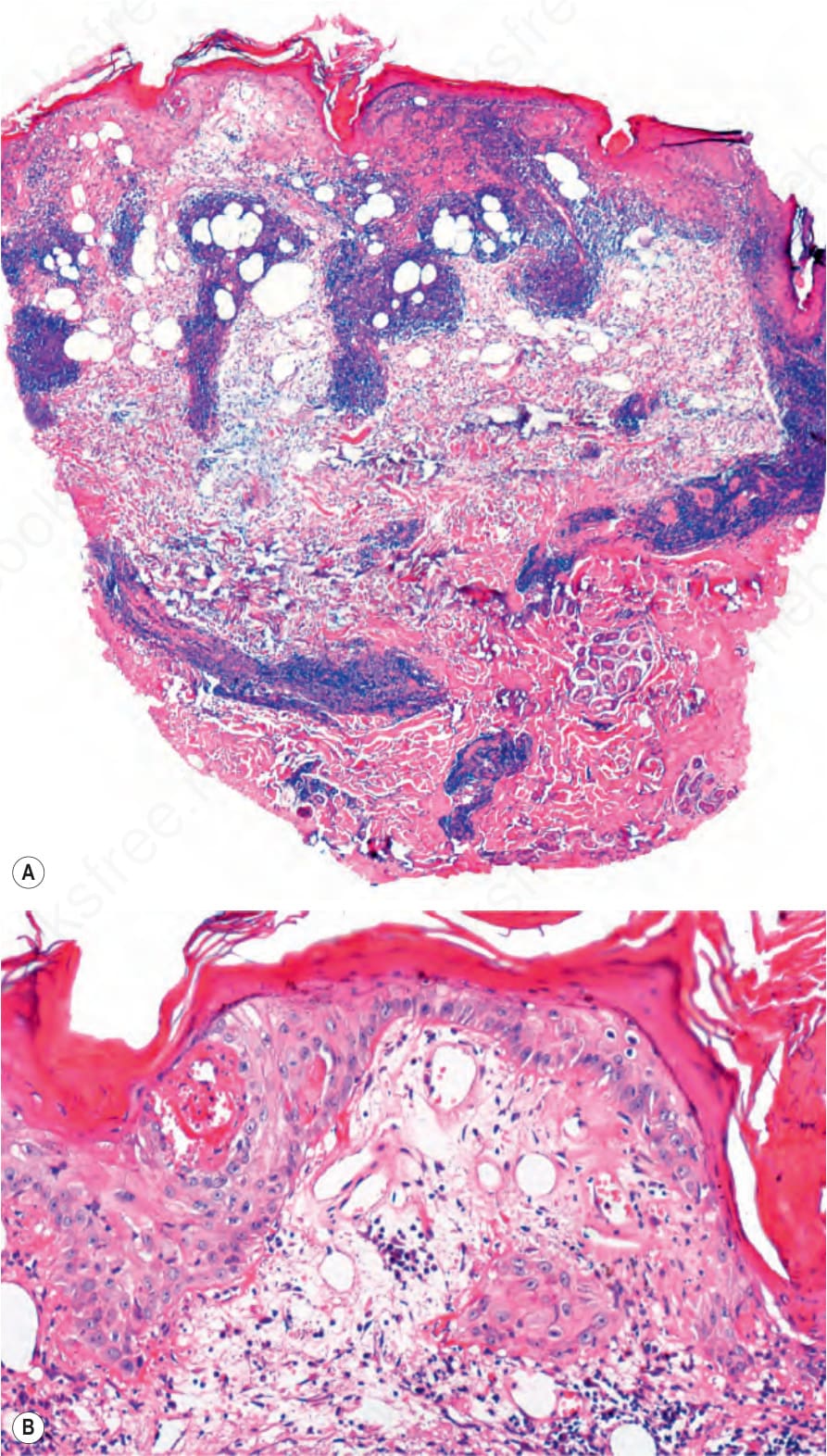
Fig. 22.126 Discoid lupus erythematosus: (A) there is loss of all the hair follicles and sebaceous glands with an intense lymphocytic infiltrate around superficial and deep blood vessels; (B) the epidermis shows dilated follicular infundibula with keratinous debris, hyperkeratosis. Also note epidermal atrophy, dermal edema, and telangiectasia.
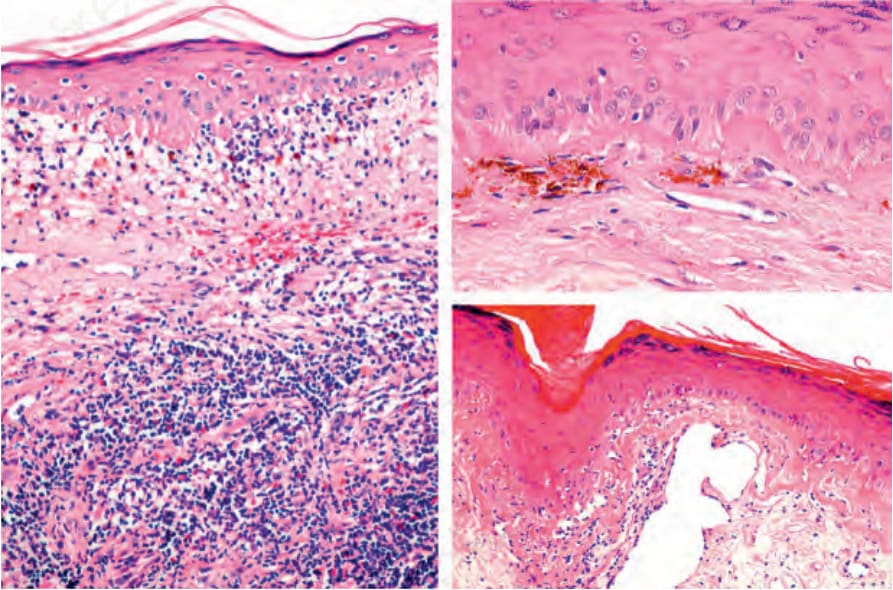
Fig. 22.127 Discoid lupus erythematosus. This image shows the typical histologic features of lupus erythematosus. Note the marked interface change and vacuolar degeneration of basal keratinocytes. In the dermis, there is a mononuclear inflammatory infiltrate with edema. The basement membrane is thickened.
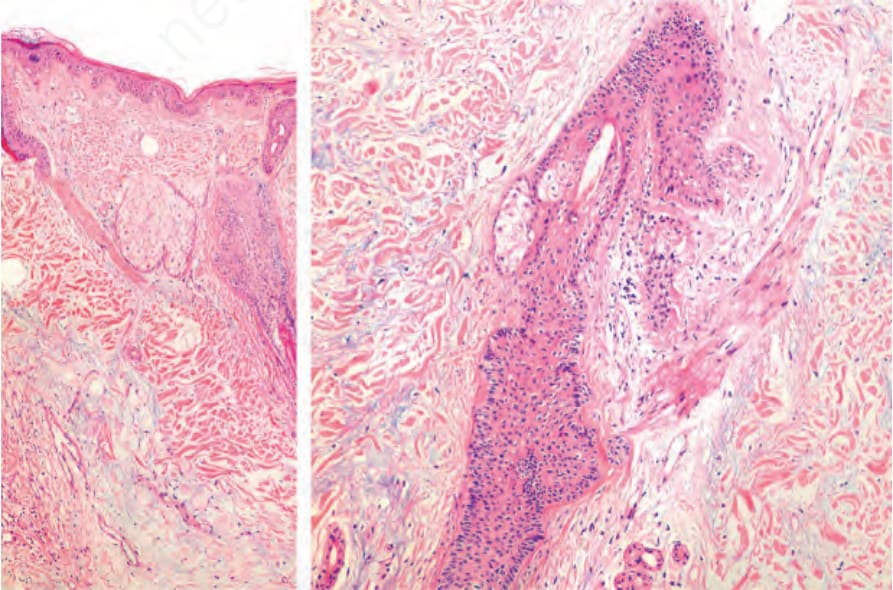
Fig. 22.128 Tumid lupus erythematosus: view of the dermis showing abundant mucin in this case with scalp involvement.
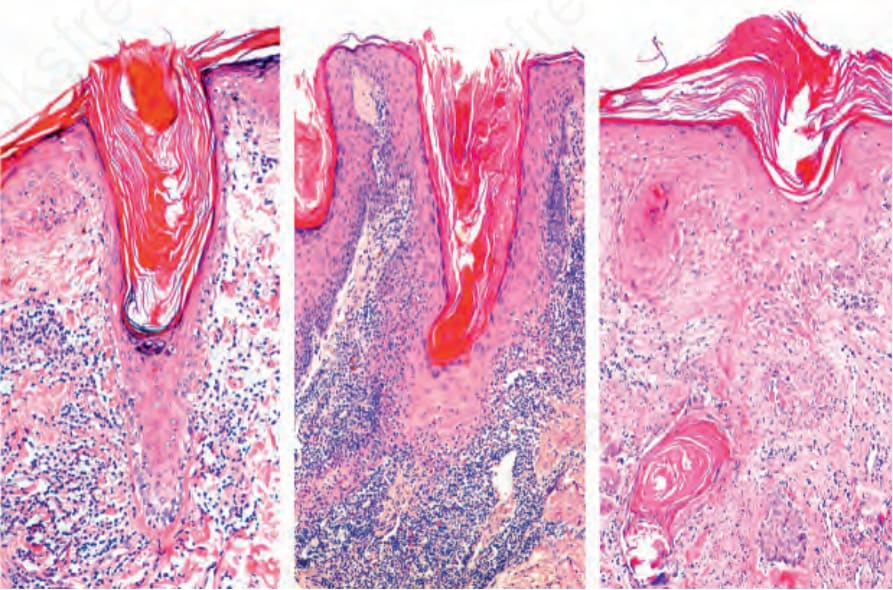
Fig. 22.129 Discoid lupus erythematosus: follicular plugging with almost complete involution of the hair follicles. There is sclerosis of the papillary and upper reticular dermis.
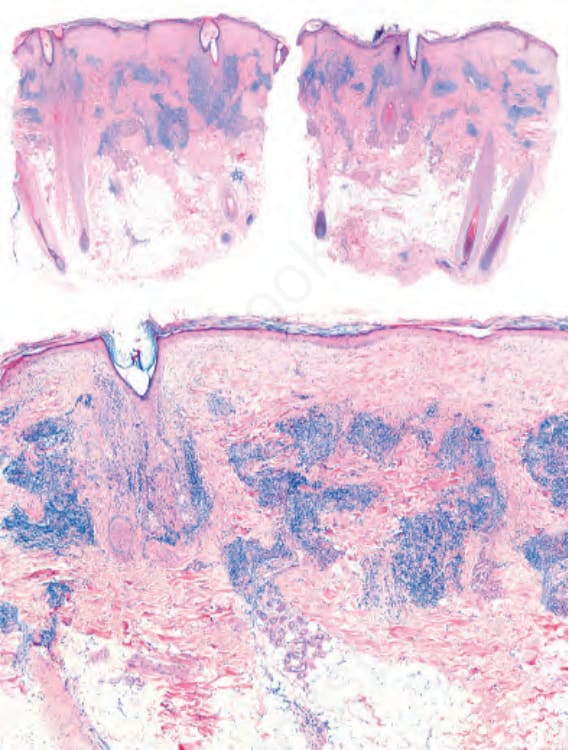
Fig. 22.130 Discoid lupus erythematosus: Prominent inflammatory cell infiltrate located around the upper segment of the hair follicles and also in a perivascular location.
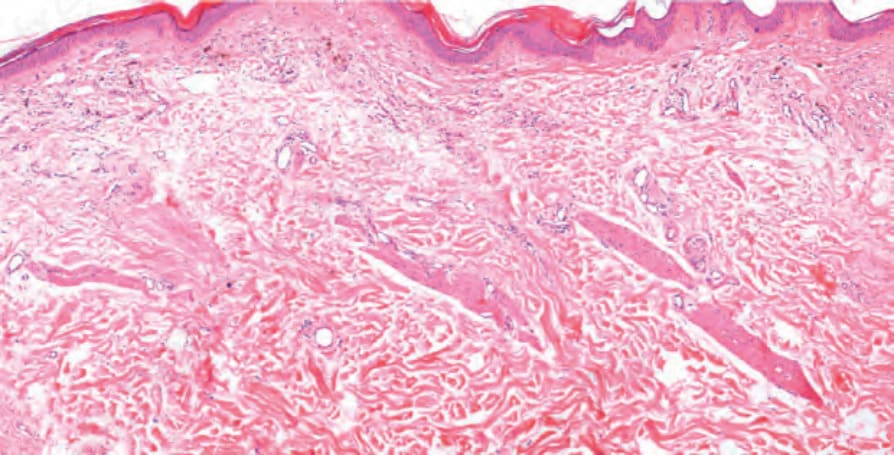
Fig. 22.131 Discoid lupus erythematosus, late stage: the hair follicles have completely disappeared, leaving follicular stellae and arrector pili muscles. In the papillary dermis, there are melanophages, and telangiectasia is evident. The inflammatory cell infiltrate is minimal.