休止期脫髮 (Telogen effluvium)
臨床特徵 (Clinical Features)
休止期脫髮 (telogen effluvium) 是女性最常見的瀰漫性脫髮型態之一。一般而言,此術語適用於那些 anagen 期 (生長期) 提早結束、許多毛髮進展至 catagen 期 (退行期) 並隨後進入 telogen 期 (休止期) 的病例。
Telogen effluvium 最早由 Kligman 於 1961 年描述,用以指稱在不同病程中 telogen 毛髮脫落增加的現象,並未指涉任何特定疾病。Telogen effluvium 的特徵為瀰漫性掉髮。臨床上有兩種表現型:一為急性、自限性的表現,持續少於 6 個月,通常由可辨識的事件所誘發;另一為病程較長、病因不明的慢性表現。
急性 telogen effluvium 可由極廣泛的事件與疾病所誘發,例如:
- 生理性過程,如新生兒與產後 (postpartum) 的 telogen effluvium、嚴重心理壓力、極端節食 (crash diets),
- 病理性事件,包括脊髓損傷、劇烈發燒 (malaria、yellow fever 與 typhoid fever)、嚴重全身性疾病、大手術、麻醉、敗血症 (septicemia)、HIV-1 感染、正顎手術 (orthognathic surgery) 後、早期 androgenetic alopecia (雄性禿)、hypothyroidism (甲狀腺功能低下)、hyperthyroidism (甲狀腺功能亢進)、iron-deficiency anemia (缺鐵性貧血)、eosinophilia-myalgia syndrome、Hodgkin lymphoma、頭皮的接觸性皮膚炎,以及飲食障礙 (eating disorders)。
亦有數種藥物被認為與之相關。其中最重要者包括 antihyperlipidemic agents、retinoids、anticoagulants、antithyroid medications、anticonvulsants、heavy metals、propranolol、nadolol、metoprolol、minoxidil、oral contraceptives、heparin、clofibrate、salicylates、gentamicin、nicotinic acid、nitrofurantoin、vitamin A、albendazole、IFN-α2b、imiquimod,以及 dopamine agonist pramipexole。與 telogen effluvium 相關的藥物清單持續增加,可參閱專門的參考資料。藥物誘發的脫髮通常可逆,並可呈現多種形式,如 telogen effluvium、anagen effluvium,或兩者兼具。
臨床上已觀察到季節性掉髮增加的現象 (seasonal alopecia)。
大多數患者為成人,主要為女性,但此過程在兒童與青少年中也相當常見。亦有合併 trichodynia (頭皮疼痛) 的記載。
檢查時,患者呈現累及整個頭皮的瀰漫性、非發炎性脫髮 (Figs 22.91 與 22.92)。脫髮約在誘發事件後 3–4 個月開始,雖然可能相當明顯,但從不會觀察到禿頭 (baldness) (Fig. 22.93)。Telogen effluvium 可與 androgenetic alopecia 重疊。
某些研究發現,患有 telogen effluvium、androgenetic alopecia 與 alopecia areata 的女性,其 ferritin 與血清 iron 濃度下降。這些發現的臨床與治療意義仍不明確,因為其他研究並未發現缺鐵與脫髮之間有任何關聯。目前,在缺乏提示貧血的臨床情境 (月經期女性、素食者,以及有貧血病史的女性) 時,尚無足夠證據建議對脫髮患者普遍篩檢缺鐵。
Hair-pull test (拉髮試驗) 與 trichogram (毛髮圖) 顯示 telogen 毛髮數量明顯增加 (見 Figs 22.3 與 22.4)。Telogen 毛髮的數量因人而異,也因疾病演變階段而異。在初期,trichogram 中的 telogen 毛髮計數偏高,但到病程結束時可能發現近乎正常的計數。Telogen 毛髮的正常上限被認為是 terminal hairs 的 15%。介於 15% 至 20% 之間提示 effluvium telogen,然而此計數在慢性 effluvium telogen 中最為常見。超過 20% 即可確定此疾病。Hair-pull test 在頭皮的所有區域皆為陽性 (Fig. 22.94)。
由於大量疾病皆可表現為 telogen effluvium,因此需要詳盡的臨床病史。同時也需要診斷檢查以辨識疾病的病因與原因。進行實驗室檢查以排除或確認亞臨床疾病 (subclinical illness),如 hypothyroidism、systemic lupus erythematosus (SLE) 或 syphilis,往往是審慎之舉。
某些患者,特別是中年停經後女性,可能出現一種慢性型的 telogen effluvium,持續超過 6 個月、病因不明、病程起伏不定,並以瀰漫性的毛髮稀疏與脫髮為特徵,常合併雙顳側退縮 (bitemporal recession) (chronic telogen effluvium)。切片通常顯示介於無變化的切片與低強度 telogen effluvium 之間的臨界 (borderline) 表現。不會發展為禿頭,因為脫落的毛髮會迅速被取代。此疾病似乎為自限性,但某些患者持續經歷慢性瀰漫性 telogen 掉髮,且無自發性改善或發展為 female pattern hair loss (女性型脫髮) 的傾向。一例罕見的男性病例曾被記載。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
Telogen effluvium 是由毛髮週期的擾亂所引起,導致 telogen 掉髮。已有人提出 telogen effluvium 是毛囊中五種不同功能變化的結果:
- immediate anagen release (發燒、壓力或藥物的發作),
- delayed anagen release (產後),
- short anagen syndrome (chronic telogen effluvium),
- immediate telogen release (外用 minoxidil 治療、seasonal alopecia),
- delayed telogen release (一種理論上的可能性)。
這些不同的機轉是由上述提及的不同刺激與過程所誘發。控制這些過程的潛在分子機轉尚不清楚。然而,有趣的是,已證實可誘導性的轉殖基因小鼠 (inducible transgenic mice),其表現出可逆的脫髮表現型,會高度表現轉錄因子 tTA (tetracycline transactivator) 與報導子 luciferase 基因。這導致 anagen 毛囊數量減少,而 telogen 毛囊數量增加。
雖然診斷可依臨床判斷做出,但當臨床表現不明確時,可能需要切片。理想上應從不同部位取兩塊切片並以水平切片 (horizontal sections) 處理,以驗證此過程的瀰漫性質,並精確計數處於 telogen、catagen 與 anagen 的毛囊數量,以及微小化毛囊 (miniaturized hair follicles) 的數量。Telogen effluvium 的組織學表現很細微,唯一的發現是深層中 telogen germinal units (休止期生發單位) (Fig. 22.95,並見 Figs 22.29–22.31)、telogen 毛囊 (Fig. 22.96) 與 follicular stellae (Fig. 22.97) 數量增加,毛囊數量正常,且無顯著發炎浸潤或毛囊微小化。這些 follicular stellae 與在 androgenic alopecia 中所見者完全相同。當疾病處於活動期時,這些變化較易觀察到,因為在緩解狀態時,處於 telogen 的毛囊數量可能正常。務必牢記此事實,因為通常正是在此時刻患者才注意到掉髮並就診於皮膚科醫師。許多看似「正常」或「超正常」(supernormal) (所有 terminal follicles 皆處於 anagen) 的頭皮切片,其實屬於臨床診斷為 telogen effluvium 的患者。Telogen terminal 毛囊的百分比一般大於 20%;然而此數字不應被視為嚴格定義,因為如先前所述,在慢性疾病患者中偶爾會發現較低的計數。
鑑別診斷 (Differential Diagnosis)
Telogen effluvium 的鑑別診斷主要與瀰漫性非瘢痕性脫髮 (diffuse nonscarring alopecias) 有關,包括 androgenetic alopecia、alopecia areata incognito,以及 loose anagen hair syndrome。
在 androgenetic alopecia 中,主要的組織學特徵為帶狀分布 (zonal pattern) 的脫髮並伴隨毛髮微小化。此外,輕柔的拉髮試驗為正常。Hair pluck (拔髮) 可能令人困惑,因為 telogen 毛髮計數較高。然而,重要的是要記得,在 androgenetic alopecia 的早期,毛囊較常進入 telogen。儘管如此,在 telogen effluvium 中,terminal 毛囊與 vellus 毛髮之間的比例仍維持在大於 7 : 1 的正常範圍內,且無發炎。當與 androgenetic alopecia 有重疊時,從兩個不同部位切片以對照各項發現 (androgenetic alopecia 的局灶性變化相對於 telogen effluvium 的瀰漫性變化) 並建立精確診斷,會非常有用。然而,同樣重要的是要記得,這兩種病況可能並存,且 chronic telogen effluvium 可能揭露隱匿的 androgenetic alopecia (Fig. 22.98)。
Alopecia areata incognito 顯示許多 yellow dots (黃點,即擴張的 infundibular 開口)、大量處於 telogen 的毛囊,以及微小化毛髮數量增加。有時可觀察到毛球 (hair bulbs) 的淋巴球浸潤。相對地,telogen effluvium 缺乏發炎與擴張 infundibular 開口的組織學證據。
Loose anagen hair syndrome 偶爾可影響無家族史的成人,可能與 telogen effluvium 混淆。其鑑別診斷容易,hair-pull test 顯示大多數毛髮處於 anagen,且拔出的毛髮缺乏外、內 root sheaths (根鞘)。Short anagen syndrome 也出現於留短髮的金髮女孩;其差異在於拉髮試驗所取得的毛髮為 telogen。此外,short anagen 的患者不會隨年齡增長而改善。
另一種可能以過量 telogen 毛囊 (計數接近 50% 或更高) 表現的病況是 trichotillomania (拔毛癖)。然而,在後者中,stellae 與 telogen germinal units 會呈現 melanin debris (黑色素碎屑),此外還有其他發現,如色素管型 (pigmented casts) 與 trichomalacia (Fig. 22.99)。
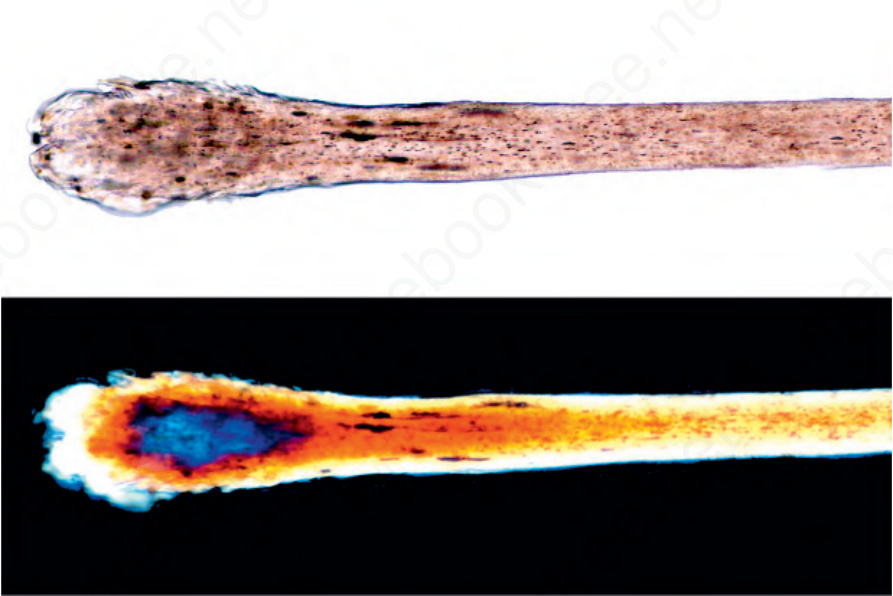
圖 22-3:偏振光顯微鏡 (polarized light microscopy)。以正常光 (上) 與偏振光 (下) 觀察到處於 telogen 之 hair shaft 與毛球的正常結構。
Fig. 22.3 Polarized light microscopy. Normal architecture of the hair shaft and the bulb in telogen is observed with normal light (above) and polarized light (below).
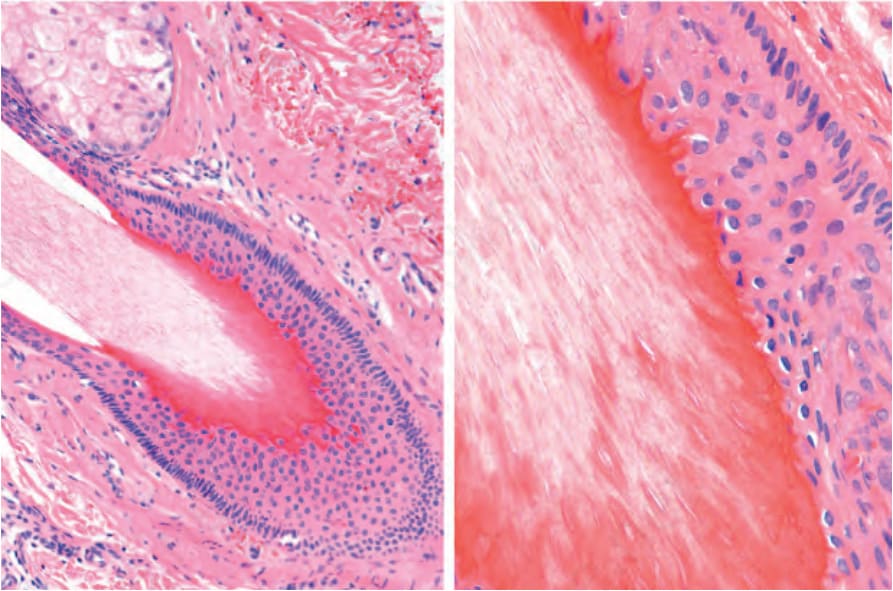
圖 22-29:晚期 catagen 的 terminal 毛囊:外根鞘 (outer root sheath) 已喪失,角化為 trichilemmal type。
Fig. 22.29 Terminal hair follicles in late catagen: the outer root sheath has been lost and the keratinization is of trichilemmal type.

圖 22-91:Telogen effluvium:注意瀰漫性脫髮且無發炎。
Fig. 22.91 Telogen effluvium: note diffuse hair loss without inflammation.

圖 22-92:Telogen effluvium 的皮膚鏡 (dermoscopy):毛囊密度低於正常,無發炎或毛囊開口 (follicular ostia) 喪失。Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
Fig. 22.92 Dermoscopy of telogen effluvium: the follicular density is lower than usual, without inflammation or loss of follicular ostia. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.

圖 22-93:Telogen effluvium;每日掉髮計數:患者在 10 天期間收集了她所掉落的毛髮。儘管掉髮量大,仍無局部的脫髮區域。Courtesy of J. Cadavid, MD, Clínica Medellín, Medellín, Colombia.
Fig. 22.93 Telogen effluvium; daily hair shedding count: during 10 days the patient has collected the hair she has shed. Despite the amount of hair loss there are no localized areas of hair loss. Courtesy of J. Cadavid, MD, Clínica Medellín, Medellín, Colombia.

圖 22-94:Hair-pull test (拉髮試驗):(A) 以手指夾住 20 至 30 根毛髮並輕柔拉扯。應該只取得處於 telogen 的毛髮;通常為總毛髮的 10%,或拉扯 30 根中的 2 或 3 根。處於 anagen 者仍黏附於頭皮。當每次拉扯取得較多的 hair shafts 時,提示毛髮疾病 (telogen effluvium)。(B) 處於 telogen 的毛髮通常因其杵狀 (club shape) 外形而可辨認。
Fig. 22.94 Hair-pull test: (A) Take 20 to 30 hairs between the fingers and gently pull. The only hairs one should obtain are those in telogen; usually 10% of the total hairs, or 2 or 3 of the 30 pulled. Those that are in anagen remain adhered to the scalp. When more hair shafts are obtained from each pull, this suggests hair disease (telogen effluvium). (B) The hairs in telogen are usually recognizable because of their club shape.
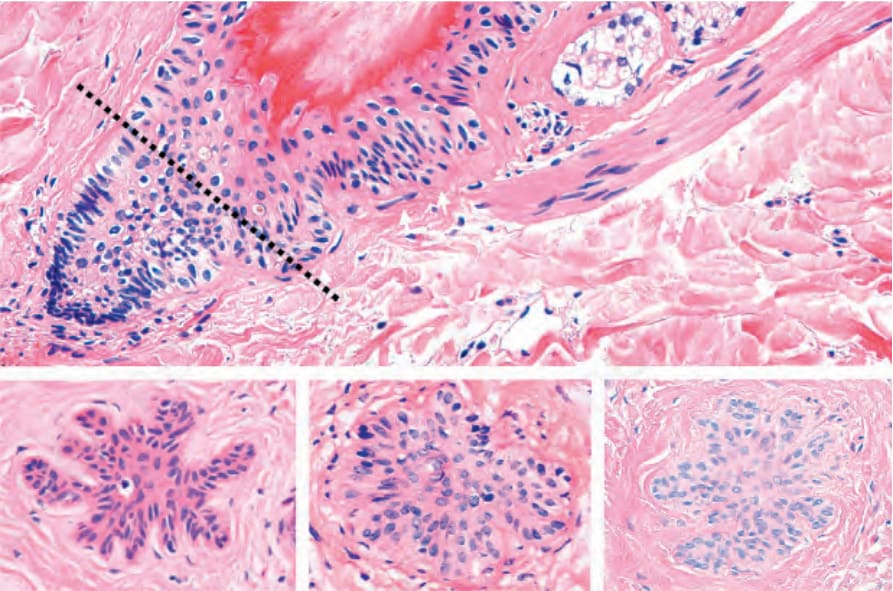
圖 22-95:Telogen germinal units (休止期生發單位,secondary germ):上圖為一毛囊處於 telogen 的垂直切片,其下段在 arrector pili muscle (豎毛肌) 的層面回縮。緊鄰此結構者為 telogen germinal unit。下圖,注意 3 個 telogen germinal units 的橫切面。
Fig. 22.95 Telogen germinal units (secondary germ): the top panel is a vertical section of a hair follicle in telogen with retraction of the lower segment at the level of the arrector pili muscle. Next to this structure is the telogen germinal unit. Bottom panel, note transverse sections of 3 telogen germinal units.
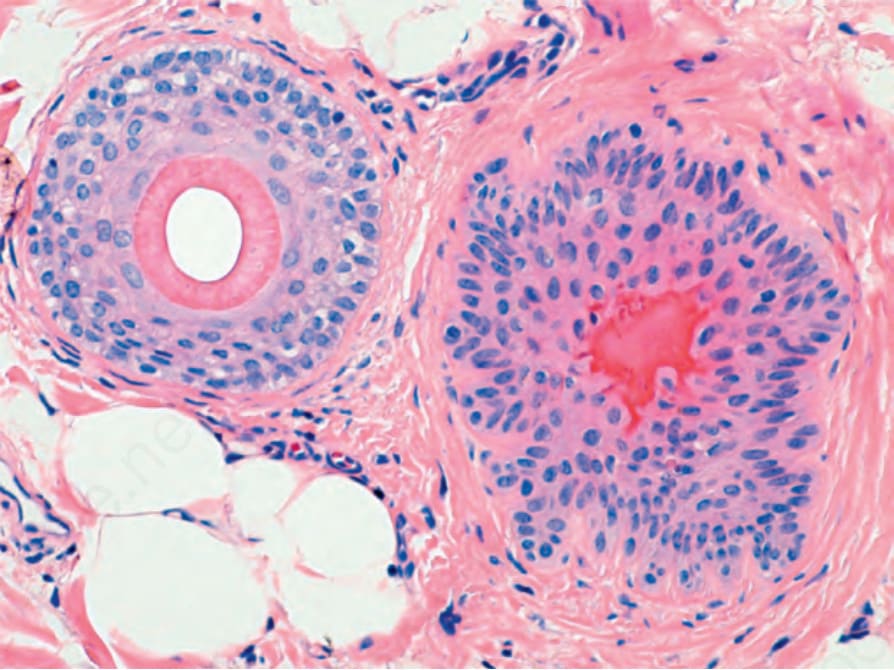
圖 22-96:Telogen 毛囊:左側為一處於 anagen 的 terminal 毛囊,右側為一處於 telogen 的毛囊,其中央顯示明顯的 trichilemmal 鮮紅色角質 (bright red keratin)。
Fig. 22.96 Telogen follicle: on the left there is a terminal follicle in anagen and on the right a hair follicle in telogen with its center displaying prominent trichilemmal bright red keratin.
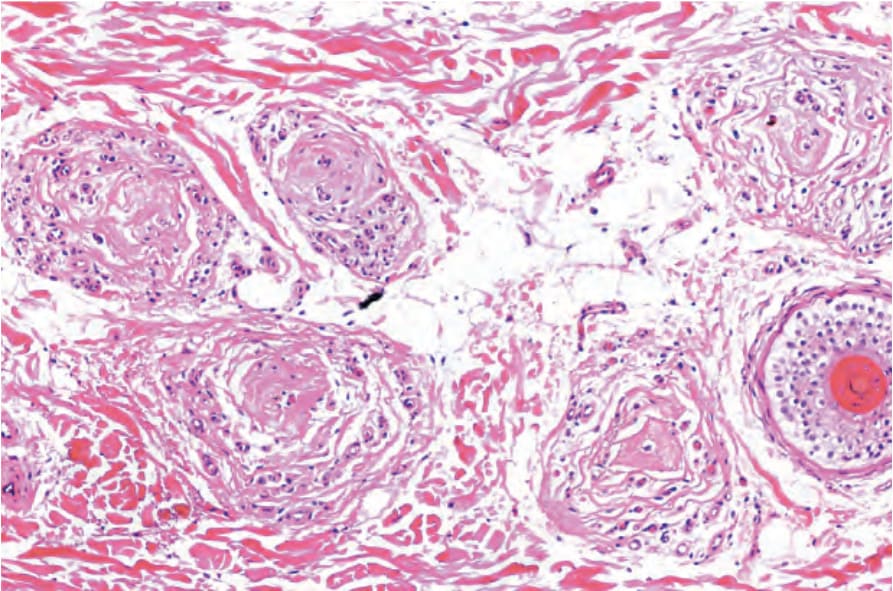
圖 22-97:Follicular stellae:五個 stellae 對應於已退化 (involuted) 的 telogen 毛囊。右側為一微小化毛囊。
Fig. 22.97 Follicular stellae: five stellae corresponding to telogen follicles that have involuted. To the right a miniaturized hair follicle.
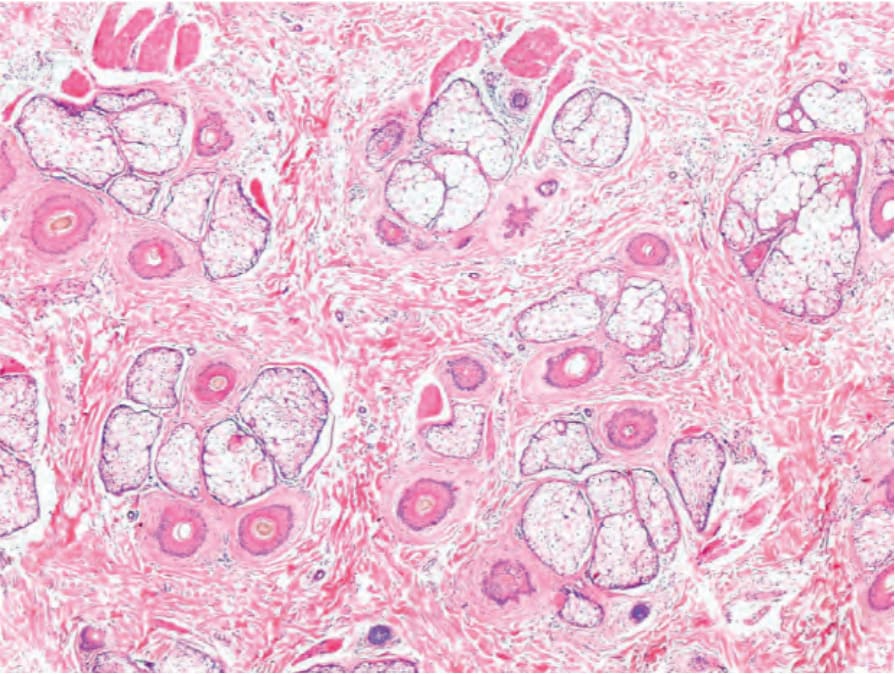
圖 22-98:Telogen effluvium 與 androgenetic alopecia:可見正常數量的毛囊單位 (follicular units) 與毛囊,並伴隨 telogen 與微小化毛囊數量增加。
Fig. 22.98 Telogen effluvium and androgenetic alopecia: normal numbers of follicular units and hair follicles are present with increased numbers of telogen and miniaturized hair follicles.
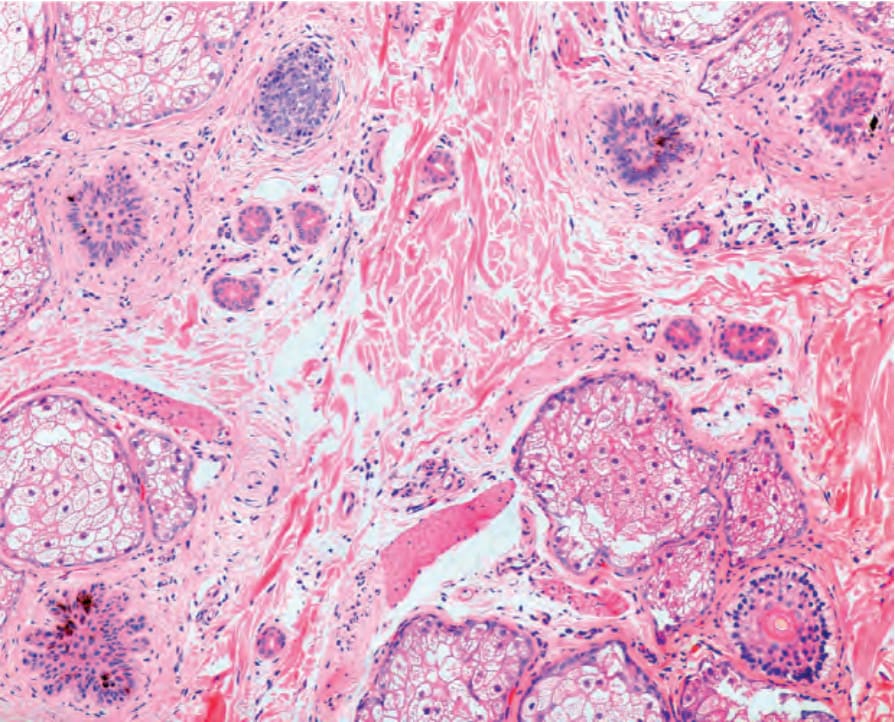
圖 22-99:Trichotillomania,色素性 telogen germinal units:此切片中有五個毛囊結構,其中四個為 telogen germinal units,帶有與毛髮創傷性拔除相關的 melanin 色素。Courtesy of A. Ruiz, MD, CES, Medellín, Colombia.
Fig. 22.99 Trichotillomania, pigmented telogen germinal units: in this biopsy there are five follicular structures, and four are telogen germinal units with melanin pigment related to the traumatic extraction of the hairs. Courtesy of A. Ruiz, MD, CES, Medellín, Colombia.