Telogen effluvium
Telogen effluvium
Clinical features Telogen effluvium is one of the most frequent forms of diffuse hair loss in women. In general, the term is applicable to those cases in which there is
an early end to anagen stage with progression of many hairs to catagen and subsequently to telogen.1
Telogen effluvium was first described by Kligman in 1961 to refer to a phenomenon of increased loss of telogen hairs in different processes without making any reference to a particular disease.2 Telogen effluvium is characterized by diffuse hair shedding. There are two clinical presentations: an acute self-limiting presentation, lasting less than 6 months, generally precipitated by a recognizable event, and a chronic presentation of longer duration and unknown etiology.
Acute telogen effluvium may be precipitated by an extensive range of events and diseases, such as:
• physiological processes such as telogen effluvium in the newborn and postpartum, severe psychological stress, crash diets,
1083 Nonscarring alopecias
• pathological events including spinal cord injury, intense fever (malaria, yellow and typhoid fevers), severe systemic illnesses, major surgery, anesthesia, septicemia, HIV-1 infection, after orthognathic surgery, early androgenetic alopecia, hypothyroidism, hyperthyroidism, iron-deficiency anemia, eosinophilia-myalgia syndrome, Hodgkin lymphoma, contact dermatitis of the scalp, and eating disorders.3–16
A number of drugs have also been implicated. The most relevant include antihyperlipidemic agents, retinoids, anticoagulants, antithyroid medications, anticonvulsants, heavy metals, propranolol, nadolol, metoprolol, minoxidil, oral contraceptives, heparin, clofibrate, salicylates, gentamicin, nicotinic acid, nitrofurantoin, vitamin A, albendazole, IFN-α2b, imiquimod, and the dopamine agonist pramipexole.2,17–24 The list of drugs associated with telogen effluvium is continuously increasing and may be consulted in specialized references. Drug-induced hair loss is often reversible and may present in various forms such as telogen effluvium, anagen effluvium, or both.25,26
A seasonal increased hair loss (seasonal alopecia) has been observed in clinical practice.27
Most patients are adults, mainly women, but the process also occurs fairly commonly in children and adolescents.28 Associated trichodynia has been documented.29
On examination, patients show diffuse noninflammatory hair loss involving the entire scalp (Figs 22.91 and 22.92). The loss of hair begins approximately 3–4 months after the precipitating event and, although it can be significantly noticeable, baldness is never observed (Fig. 22.93). Telogen effluvium can overlap with androgenetic alopecia.
carry out laboratory tests to exclude or confirm a subclinical illness such as hypothyroidism, systemic lupus erythematosus (SLE), or syphilis.
Some studies have found decreased ferritin and serum iron levels in females with telogen effluvium, androgenetic alopecia, and alopecia areata. The clinical and therapeutical significance of these findings is still unclear, as other studies have not found any relationship between iron deficiency and hair loss. Currently, in the absence of a clinical setting suggestive of anemia (menstruating women, vegetarians, and women with a history of anemia), there is insufficient evidence to recommend universal screening for iron deficiency in patients with hair loss.30–32
The hair-pull test and trichogram show a net increase in the number of telogen hairs (see Figs 22.3 and 22.4). The number of telogen hairs varies from individual to individual and also according to the stage of evolution of the disease. In the initial stages the telogen hair count in trichogram is high, but by the end of the process almost normal counts may be found. The upper normal limit of telogen hairs is considered to be 15% of terminal hairs. Between 15% and 20% is suggestive of effluvium telogen, yet this count is the most frequently found in chronic effluvium telogen. More than 20% is a determinant of the disease. The hair-pull test is positive in all areas of the scalp (Fig. 22.94).
Owing to the great number of diseases that may present as telogen effluvium, a thorough clinical history is necessary. Diagnostic tests to identify the etiology and cause of the disease are also required. It is often prudent to
Some patients, particularly middle-aged postmenopausal women, may present with a chronic form of telogen effluvium that lasts more than 6 months, is of unknown etiology, has a fluctuating course, and is characterized by a diffuse pattern of hair thinning and hair loss, often associated with bitemporal recession (chronic telogen effluvium). The biopsy generally shows borderline findings between a biopsy with no alterations and a telogen effluvium of low intensity. Baldness does not develop because lost hairs are quickly replaced.33–36 The disease appears to be self-limiting, but some patients continue to experience chronic diffuse telogen hair shedding without tendency toward spontaneous improvement or development of female pattern hair loss.37 An exceptional case has been documented in a man.38
1084 Diseases of the hair
A
B
Pathogenesis and histologic features
Telogen effluvium is caused by a disturbance of the hair cycle which results in telogen shedding. It has been proposed that telogen effluvium develops as a result of five different functional changes in the hair follicle:39,40
• immediate anagen release (episode of fever, stress or medication),
• delayed anagen release (postpartum),
• short anagen syndrome (chronic telogen effluvium),
• immediate telogen release (topical minoxidil therapy, seasonal alopecia),
• delayed telogen release (a theoretical possibility). These different mechanisms are precipitated by the different stimuli and processes mentioned above. The underlying molecular mechanisms controlling these processes are unknown. Interestingly, however, it has been shown that inducible transgenic mice, which display a reversible hair loss phenotype, express high levels of the transcription factor tTA (tetracycline transactivator) and reporter luciferase gene.41 This results in a decreased
number of anagen hair follicles and an increase in the number of telogen hair follicles.
Although the diagnosis can be made on clinical grounds, when the clinical presentation is unclear, a biopsy may be necessary. Ideally, two biopsies should be taken from different sites and processed with horizontal sections to verify the diffuse nature of the process and to produce an exact count of the number of hair follicles in telogen, catagen, and anagen and the number of miniaturized hair follicles. The histologic findings in telogen effluvium are subtle, the only finding being an increase in the number of telogen germinal units (Fig. 22.95, and see Figs 22.29–22.31), telogen hair follicles (Fig. 22.96), and follicular stellae (Fig. 22.97) in the deep layers, with a normal number of hair follicles and absence of a significant inflammatory infiltrate or follicular miniaturization. The follicular stellae are identical to those observed in androgenic alopecia.42,43 These changes are better observed when the illness is active, as in the resolution state the number of follicles
1085 Nonscarring alopecias
in telogen may be normal. It is very important to bear in mind this fact, as normally this is the moment in which the patient notices the shedding and consults the dermatologist. Many scalp biopsies that appear ‘normal’ or ‘supernormal’ (all terminal follicles in anagen) belong to patients with the clinical diagnosis of telogen effluvium.44,45 The percentage of telogen terminal hair follicles is generally greater than 20%; however, this figure should not be taken as a rigid definition since lower counts are occasionally found in patients with chronic disease as discussed before.
Differential diagnosis The differential diagnosis of telogen effluvium is mainly with diffuse nonscarring alopecias, including androgenetic alopecia, alopecia areata incognito, and loose anagen hair syndrome.40
In androgenetic alopecia, the main histologic feature consists of a zonal pattern of hair loss with miniaturization of hairs. In addition, the gentle hair pull is normal. Hair pluck can be puzzling due to a higher count of hairs in telogen. It is important to remember, however, that in the early stages of androgenetic alopecia, hair follicles more frequently enter telogen. Nevertheless, in telogen effluvium the ratio between terminal hair follicles and vellus hairs remains within the normal range of greater than 7 : 1 and there is no inflammation.46 In cases when there is overlap with androgenetic alopecia, it is very useful to biopsy two different sites to correlate the findings (focal changes in androgenetic alopecia versus diffuse changes in telogen effluvium) and establish a precise diagnosis. However, it is also important to remember that the two conditions may coexist and that chronic telogen effluvium may uncover occult androgenetic alopecia (Fig. 22.98).45,47–49
Alopecia areata incognito displays many yellow dots (dilated infundibular openings), numerous hair follicles in telogen, and increased number of miniaturized hairs. Lymphoid infiltration of the hair bulbs is sometimes observed. In contrast, telogen effluvium lacks histologic evidence of inflammation and dilated infundibular openings. 50
Loose anagen hair syndrome which may occasionally affect adults without a family history can be confused with telogen effluvium. The differential diagnosis is easy, with the hair-pull test showing the majority of the hairs in anagen and the extracted hairs lacking external and internal root sheaths. Short anagen syndrome presents also in blonde girls with short hair; the difference is that the hair that is obtained in the pull test is telogen.51 Additionally, the patients with short anagen do not improve with age.52
Another condition that may present with an excess of telogen hair follicles, (with number counts near 50% or more) is trichotillomania. Nevertheless, in this latter disorder, the stellae and telogen germinal units present melanin debris, in addition to the other findings such as pigmented casts and trichomalacia (Fig. 22.99).
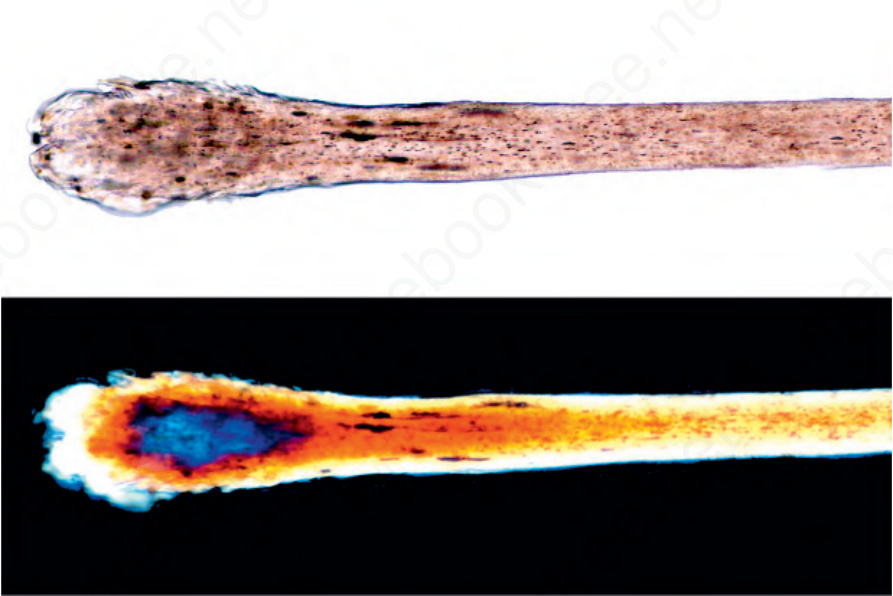
Fig. 22.3 Polarized light microscopy. Normal architecture of the hair shaft and the bulb in telogen is observed with normal light (above) and polarized light (below).
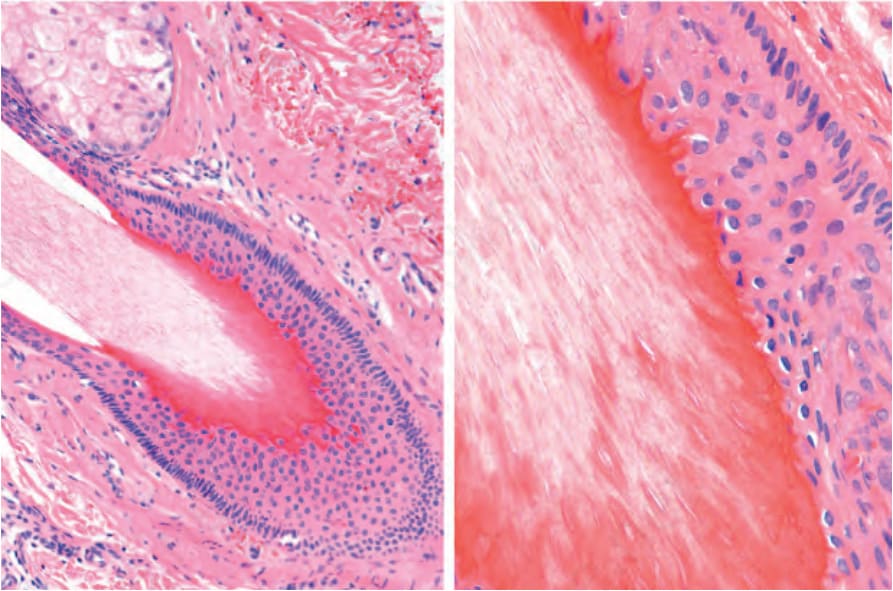
Fig. 22.29 Terminal hair follicles in late catagen: the outer root sheath has been lost and the keratinization is of trichilemmal type.

Fig. 22.91 Telogen effluvium: note diffuse hair loss without inflammation.

Fig. 22.92 Dermoscopy of telogen effluvium: the follicular density is lower than usual, without inflammation or loss of follicular ostia. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.

Fig. 22.93 Telogen effluvium; daily hair shedding count: during 10 days the patient has collected the hair she has shed. Despite the amount of hair loss there are no localized areas of hair loss. Courtesy of J. Cadavid, MD, Clínica Medellín, Medellín, Colombia.

Fig. 22.94 Hair-pull test: (A) Take 20 to 30 hairs between the fingers and gently pull. The only hairs one should obtain are those in telogen; usually 10% of the total hairs, or 2 or 3 of the 30 pulled. Those that are in anagen remain adhered to the scalp. When more hair shafts are obtained from each pull, this suggests hair disease (telogen effluvium). (B) The hairs in telogen are usually recognizable because of their club shape.
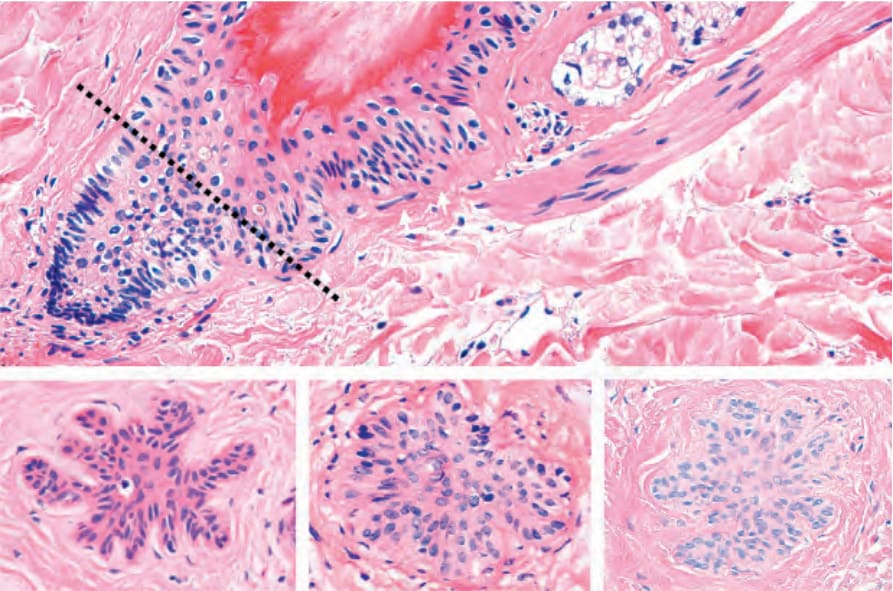
Fig. 22.95 Telogen germinal units (secondary germ): the top panel is a vertical section of a hair follicle in telogen with retraction of the lower segment at the level of the arrector pili muscle. Next to this structure is the telogen germinal unit. Bottom panel, note transverse sections of 3 telogen germinal units.
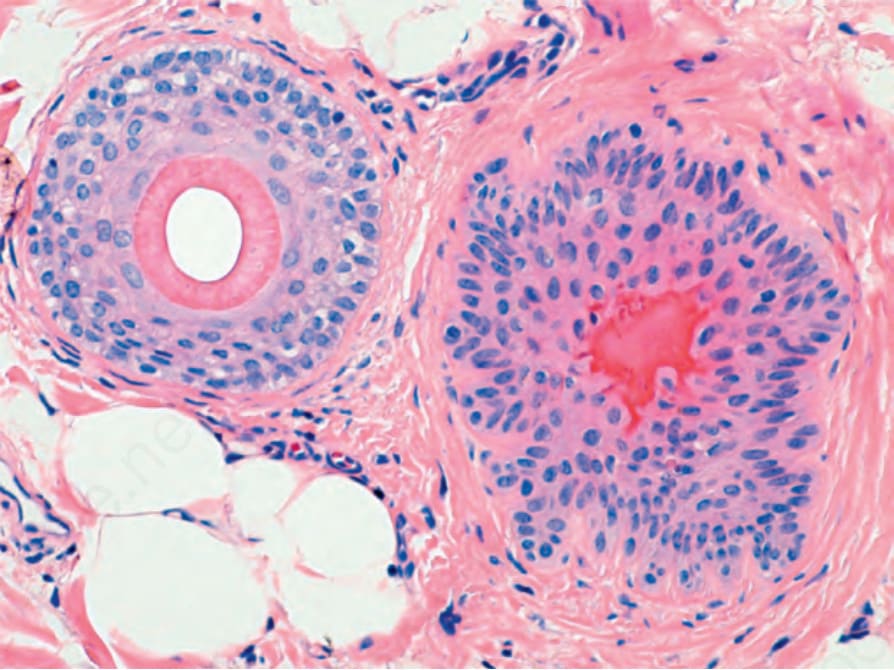
Fig. 22.96 Telogen follicle: on the left there is a terminal follicle in anagen and on the right a hair follicle in telogen with its center displaying prominent trichilemmal bright red keratin.
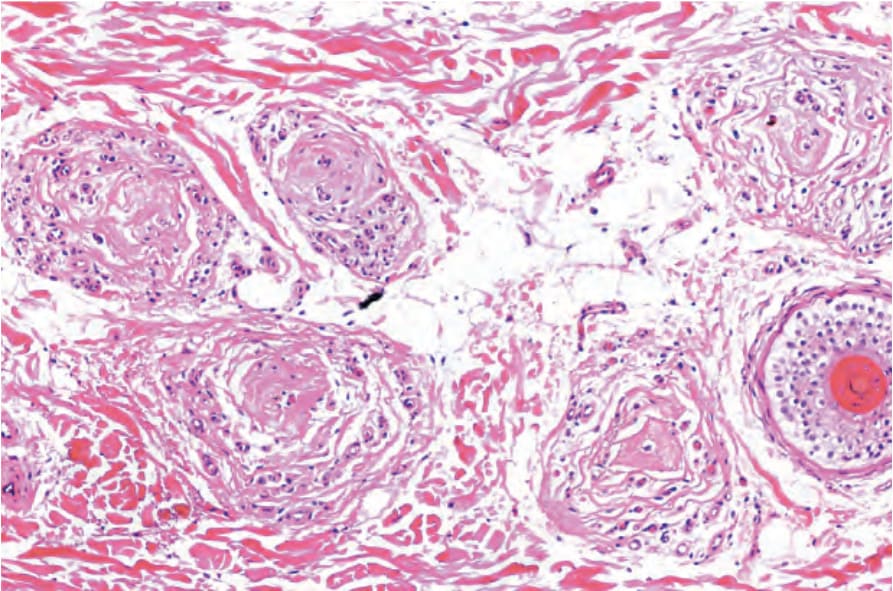
Fig. 22.97 Follicular stellae: five stellae corresponding to telogen follicles that have involuted. To the right a miniaturized hair follicle.
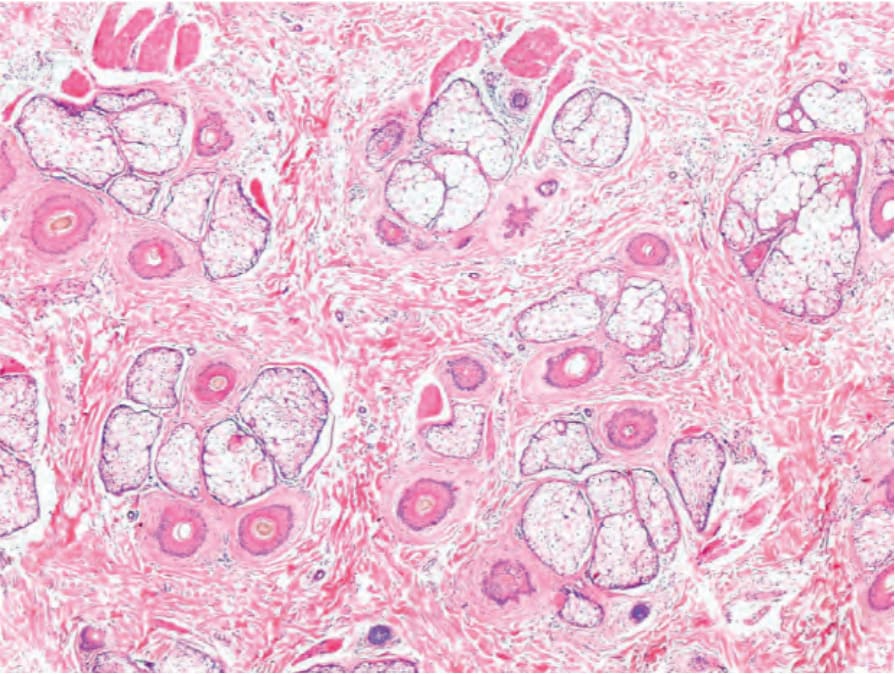
Fig. 22.98 Telogen effluvium and androgenetic alopecia: normal numbers of follicular units and hair follicles are present with increased numbers of telogen and miniaturized hair follicles.
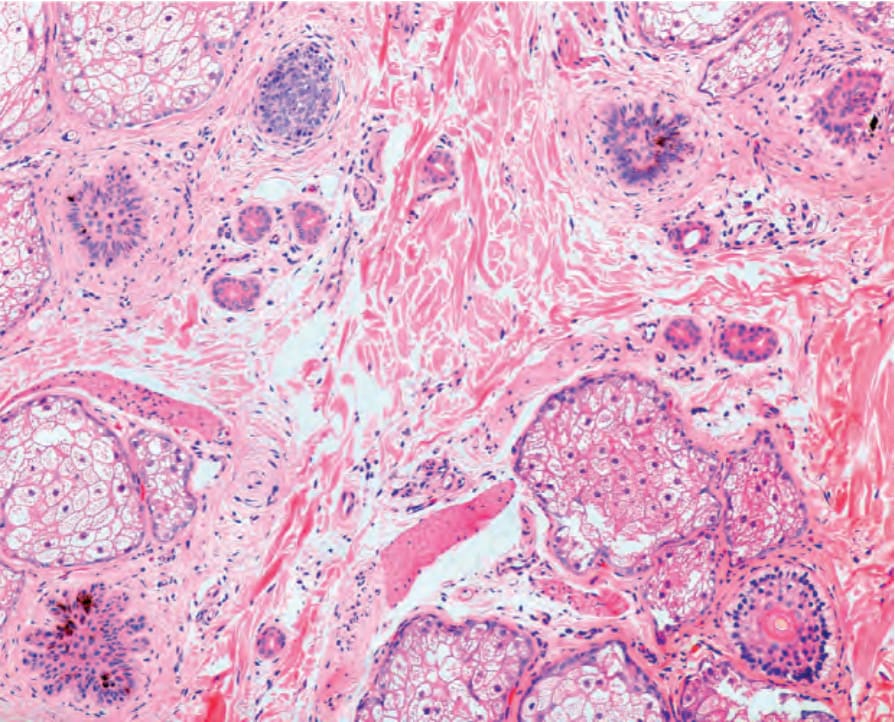
Fig. 22.99 Trichotillomania, pigmented telogen germinal units: in this biopsy there are five follicular structures, and four are telogen germinal units with melanin pigment related to the traumatic extraction of the hairs. Courtesy of A. Ruiz, MD, CES, Medellín, Colombia.