拔毛癖 (Trichotillomania)
臨床特徵 (Clinical Features)
拔毛癖 (trichotillomania) 由 Hallopeau 於一八八九年首次描述。它是外傷性禿髮 (traumatic alopecia) 的一種變異型,由牽拉與拔扯頭髮所造成。本病主要影響年輕女性,但也可見於較年長的成人與兒童,包括幼兒。雖然有些病人承認自己拔頭髮,但根據我們的經驗,絕大多數病人都斷然否認此行為。因此,通常需要進行徹底的問診與詳細的精神科病史採集。
拔毛癖構成一種慢性精神疾病,其強度與表現多變,可導致病人生活上嚴重的情緒與社交限制。拔毛癖與強迫症 (obsessive-compulsive disorder) 有部分共通特徵。在最嚴重的病例中,它可能合併較深層的人格障礙,例如自我傷害 (self-harming)、食毛癖 (trichophagia) 與毛糞石 (trichobezoar,Rapunzel 症候群)。偶爾,拔毛的衝動不僅限於頭皮,也可能涉及其他身體部位,包括陰阜、眉毛、睫毛,甚至鼻孔。
拔毛癖的常見程度可能與強迫症相當,可能影響高達百分之三的美國人口。亞臨床型 (subclinical forms) 也相當常見,可能影響每十名美國人中的一人。
慢性拔毛有兩種模式。最嚴重且最毀容的一種,是病人在短時間內拔下大量頭髮,並由負面情緒狀態所觸發。最不嚴重的模式則是病人在靜態與社交活動(例如閱讀、看電視或講電話)期間拔毛。
拔毛癖的脫髮模式相當多變,從單一孤立區域受累(「修士 Tuck 徵 (friar Tuck sign)」),到多個幾何形區域、幾乎可影響整個頭皮(圖 22.75 與 22.76)。與圓禿 (alopecia areata) 相反,其脫髮通常是不完全的。在每一個受累區域內都有脫髮,但並非完全脫光,因為使用放大鏡可看見殘留的、細小的、斷裂的、無色素的毛髮。有時可見紅斑、膿疱形成或外傷性表皮剝脫 (traumatic excoriations) 的證據(圖 22.77)。也不罕見發現其他有毛部位受累(圖 22.78)。
由於此型禿髮的毛髮甚短,通常無法以拔髮法 (hair-pull) 或拔毛法 (hair-pluck) 技術取得毛髮。在禿髮區邊緣以這些技術評估的毛髮為正常。
毛髮生長窗技術 (hair-growth window technique) 對拔毛癖的診斷非常有用。它涉及在頭皮(後腦勺)剃除一塊 2.0 cm2 的區域,使病人無法從此部位拔毛。若可能,此區域應加以選擇,以使相鄰的毛髮可遮蓋住剃除區(圖 22.79)。若在一週結束時毛髮正常生長,即可確診拔毛癖。之所以僅在一週後評估毛髮生長,是因為在此階段正常毛髮仍非常短,病人無法搆到它們。毛髮每月約生長 1.0 cm,一週內毛髮長度平均應為
在罕見的廣泛性拔毛癖病人中,可見蟲蝕狀外觀 (moth-eaten appearance),以致可能需要以血清學檢查排除梅毒 (syphilis)。
2.5 mm。然而,頭皮上個別毛髮的生長速率可能不均一。
組織病理特徵 (Histopathology)
拔毛癖的組織學特徵相當獨特,配合臨床對照,可在大多數病例中作出診斷。在水平與垂直切片中,相當容易觀察到最重要的組織學成分,而這些成分僅影響終毛毛囊 (terminal follicles)。微小化的毳毛 (miniaturized vellus) 與毛囊因其短小的長度而免於被拔出。最重要的組織學變化為退行期毛囊 (catagen follicles)、色素管型 (pigmented casts),以及受外傷與變形的毛囊。
最佳的切片是在毛髮被拔除後的最初兩個月內取得。應檢查許多切片,因為只有少數切片可能顯示出特徵性變化。
受外傷與變形的毛囊代表顯示出各種不同改變的毛囊結構。最常見的變化包括內毛根鞘 (inner root sheath) 塌陷、毛囊間與毛囊內出血,以及毛軟化 (trichomalacia)。後者指的是變形的、小的、不完全角化的毛囊,其囊壁厚度不均(圖 22.84)。它們可能顯示不規則的色素沉著。儘管拔毛癖中毛囊有廣泛的解剖學與生理學改變,發炎反應卻極輕微。其他組織學發現包括色素性毛囊星狀體 (pigmented follicular stellae)(圖 22.85)。
在掃描放大倍率下,最顯著的特徵包括極高百分比的退行期或休止期毛囊 (catagen or telogen hair follicles)、若干正常毛囊,以及缺乏發炎(圖 22.80)。受累的毛囊容易辨識,因為它們含有深紅色角蛋白 (dark-red keratin),且外毛根鞘 (external root sheath) 顯示廣泛的細胞凋亡 (apoptosis)(見圖 22.26 與 22.29)。
色素管型對應於毛基質與毛皮質中的色素細胞,這些細胞因牽拉而脫位,並被移位至毛管、外毛根鞘、纖維性拖尾 (fibrous streamers) 與真皮乳頭 (dermal papilla)。
在拔毛癖中,色素管型可見於毛管的各個層面,主要位於漏斗部 (infundibulum) 與毛囊口 (ostium),並與過度角化 (hyperkeratosis) 相關(圖 22.81 與 22.82)。這些管型偶爾也可見於圓禿、化療誘發性禿髮 (chemotherapy-induced alopecia) 與壓力誘發性禿髮 (pressure induced alopecia)。在色素稀少的金髮或紅髮者中,它們可能難以偵測。另一種觀察到的形態學改變是毛幹內出現垂直走向的裂隙。此裂隙缺損充滿了蛋白質性物質與紅血球。其組織學影像令人聯想到夾在麵包中的漢堡(「漢堡徵 (hamburger sign)」)(圖 22.83)。有時,色素物質呈現出其他形狀,類似拉鍊,或類似鈕扣及其扣眼。
鑑別診斷 (Differential Diagnosis)
外傷性禿髮(特別是拔毛癖)最重要的臨床與組織學鑑別診斷是 alopecia areata。在後者中,偶爾也可發現色素管型與 trichomalacia。然而,在 alopecia areata 中後一成分極輕微,且有休止期毛囊 (telogen follicles)、小的生長期毛囊 (small anagen follicles)、微小化毛髮 (miniaturized hairs),以及毛球周圍發炎細胞浸潤 (peribulbar inflammatory cell infiltrate)。梅毒性禿髮 (syphilitic alopecia) 在臨床上也可能類似拔毛癖,但後者(拔毛癖)的色素管型、trichomalacia 與缺乏發炎細胞浸潤通常能讓兩者輕易區分。然而在困難的病例中,有時仍需血清學檢查。
另外有兩種狀況在鑑別診斷中必須牢記:剪毛癖 (trichotemnomania),這是一種以剪刀或剃刀剪斷頭髮的強迫性習慣;以及摩毛癖 (trichoteiromania),這是由於持續摩擦頭皮導致毛幹斷裂所造成。與後者相關的是因衣物(例如襪子、褲子)或床鋪持續壓迫所導致的摩擦性脫髮 (frictional hair loss)。後面這些病症並無診斷性組織病理學特徵,且呈現正常的組織學表現。
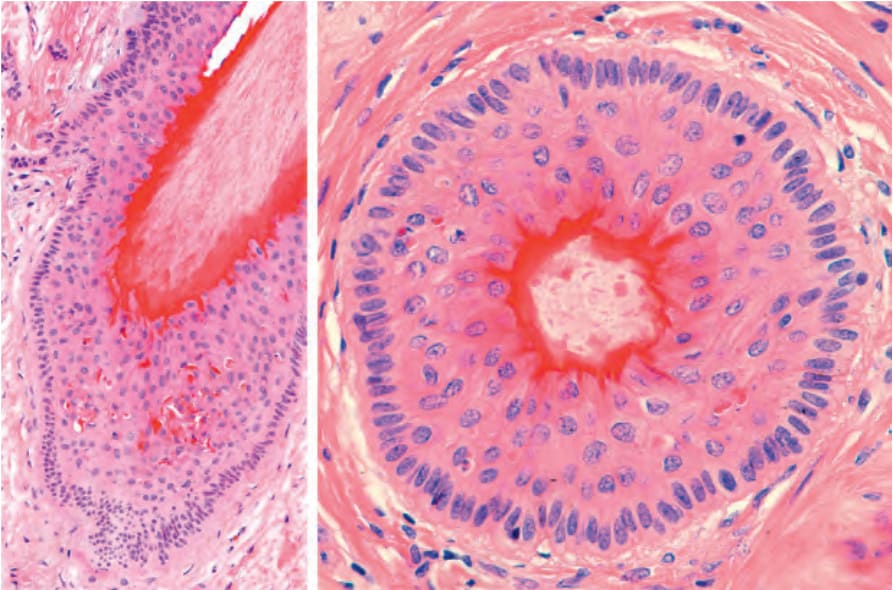
圖 22-26:退行期 (catagen) 的終毛毛囊,垂直與水平切片:注意毛囊的退縮,以及圍繞棒狀毛幹 (club-shaped hair shaft) 的深紅色毛鞘角化 (trichilemmal keratinization)。外毛根鞘顯示顯著的細胞凋亡 (apoptosis)。在毛囊最深處,可見次級毛芽形成 (secondary germ formation) 的跡象。
Fig. 22.26 Terminal hair follicle in catagen, vertical and horizontal sections: note the involution of the follicle and the deep red trichilemmal keratinization around the club-shaped hair shaft. The outer root sheath shows marked apoptosis. At the deepest part of the follicle, there is a hint of secondary germ formation.
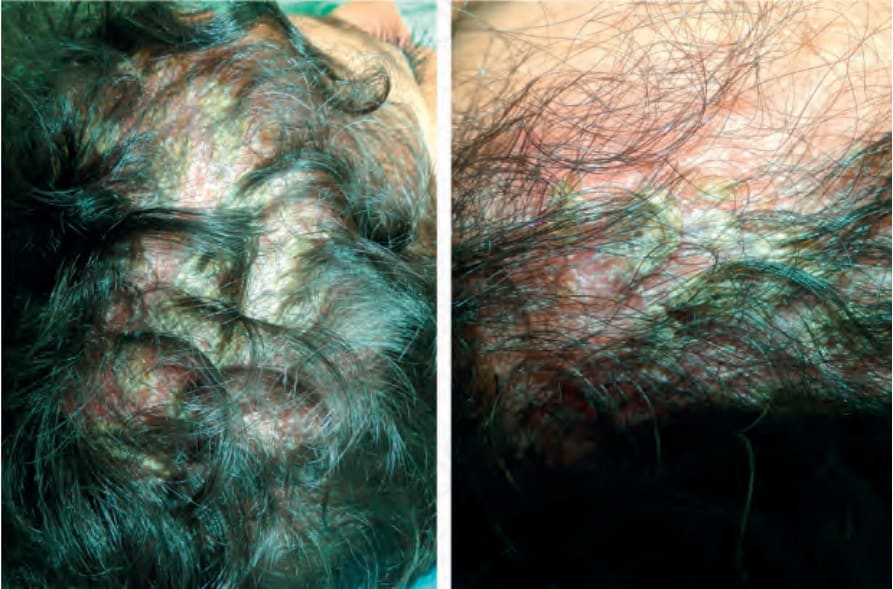
圖 22-72:乾癬 (Psoriasis)。注意一層厚鱗屑覆蓋於禿髮區域,類似頭癬 (tinea capitis)。Courtesy of C. Velázquez, MD, CES, Medellín, Colombia。
Fig. 22.72 Psoriasis. Note a thick scale covering an area of alopecia simulating tinea capitis. Courtesy of C. Velázquez, MD, CES, Medellín, Colombia.
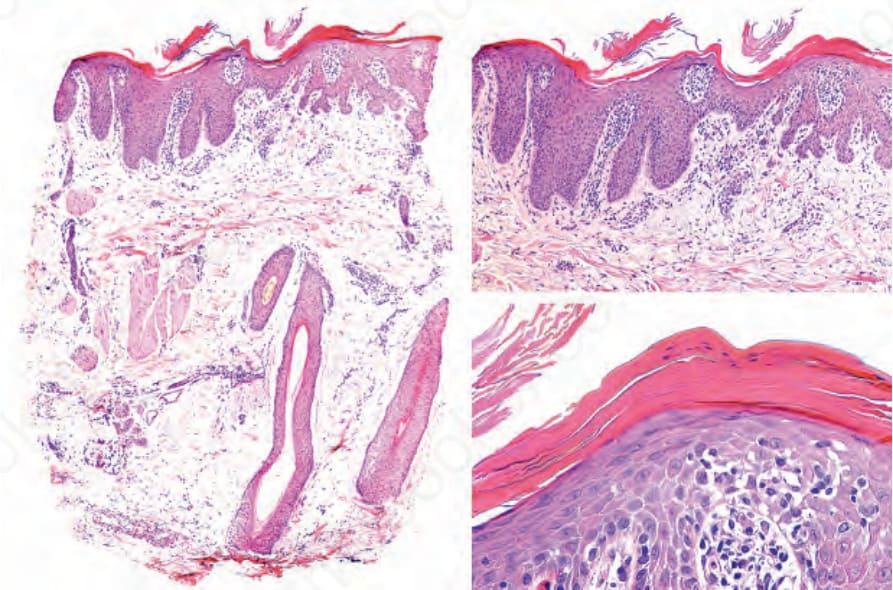
圖 22-73:乾癬 (Psoriasis)。左側可明顯見到皮脂腺與毛囊單位的喪失。右圖為表皮的乾癬性變化,包括表皮突 (rete ridges) 延長、過度角化 (hyperkeratosis)、角化不全 (parakeratosis)、顆粒層減少 (hypogranulosis) 與角質層內中性球 (corneal neutrophils)。
Fig. 22.73 Psoriasis. On the left the loss of sebaceous glands and follicular units is evident. On the right panel epidermal psoriatic changes including elongation of the rete ridges, hyperkeratosis, parakeratosis, hypogranulosis and corneal neutrophils.
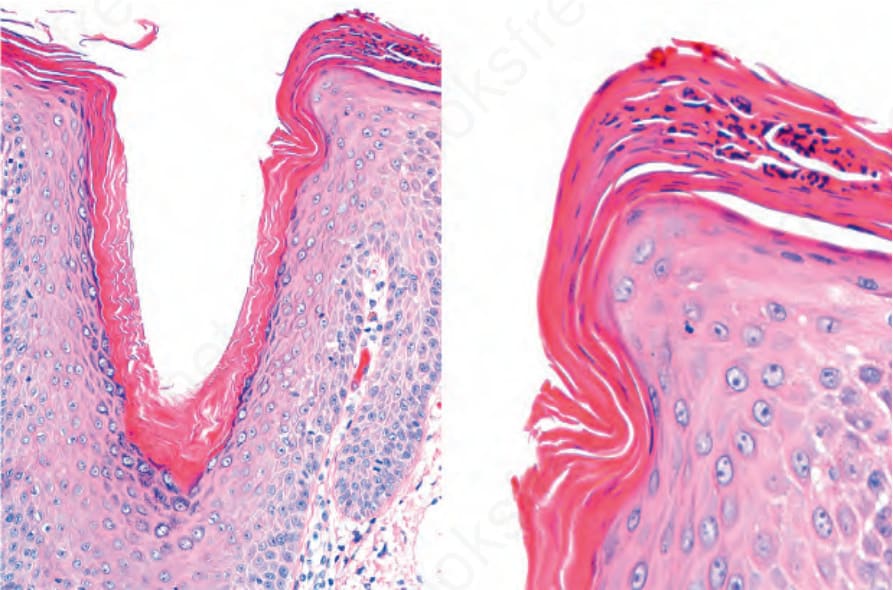
圖 22-74:頭皮乾癬 (Psoriasis of the scalp),其變化類似脂漏性皮膚炎 (seborrheic dermatitis)。有過度角化 (hyperkeratosis) 與角化不全 (parakeratosis) 並伴有中性球聚集,在毛囊口 (follicular ostium) 邊緣更為明顯。
Fig. 22.74 Psoriasis of the scalp with changes simulating of seborrheic dermatitis. There is hyperkeratosis and parakeratosis with collections of neutrophils, more pronounced at the lip of the follicular ostium.

圖 22-75:拔毛癖 (Trichotillomania):輕度受累,呈現非常斑駁的脫髮。Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia。
Fig. 22.75 Trichotillomania: mild involvement with very patchy hair loss. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
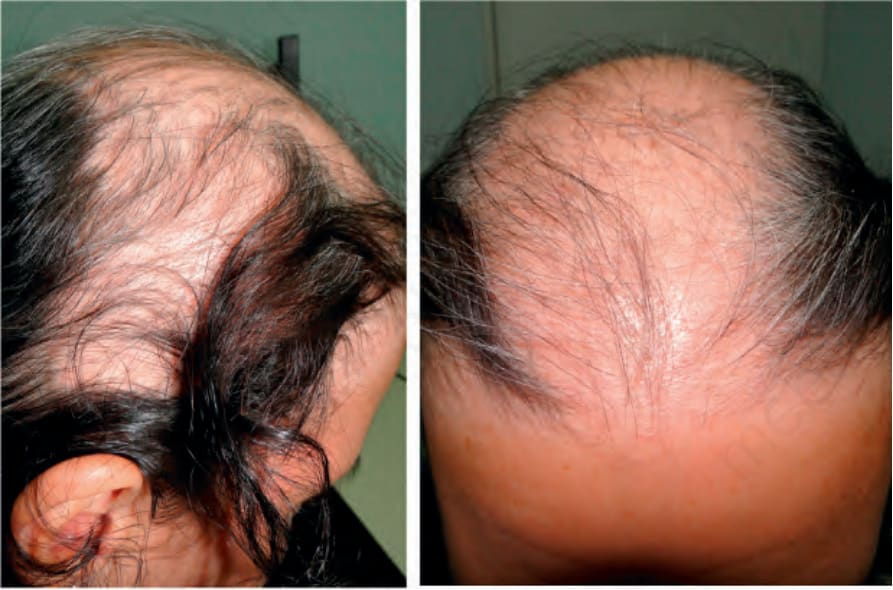
圖 22-76:拔毛癖 (Trichotillomania):嚴重受累的年輕病人,脫髮更為明顯且廣泛,呈現怪異的模式。Courtesy of C. Velázquez, MD, CES, Medellín, Colombia。
Fig. 22.76 Trichotillomania: severely affected young patient, with much more obvious and extensive hair loss with a bizarre pattern. Courtesy of C. Velázquez, MD, CES, Medellín, Colombia.

圖 22-77:拔毛癖 (Trichotillomania):注意左側的表皮剝脫 (excoriations)。Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia。
Fig. 22.77 Trichotillomania: note excoriations on the left side. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
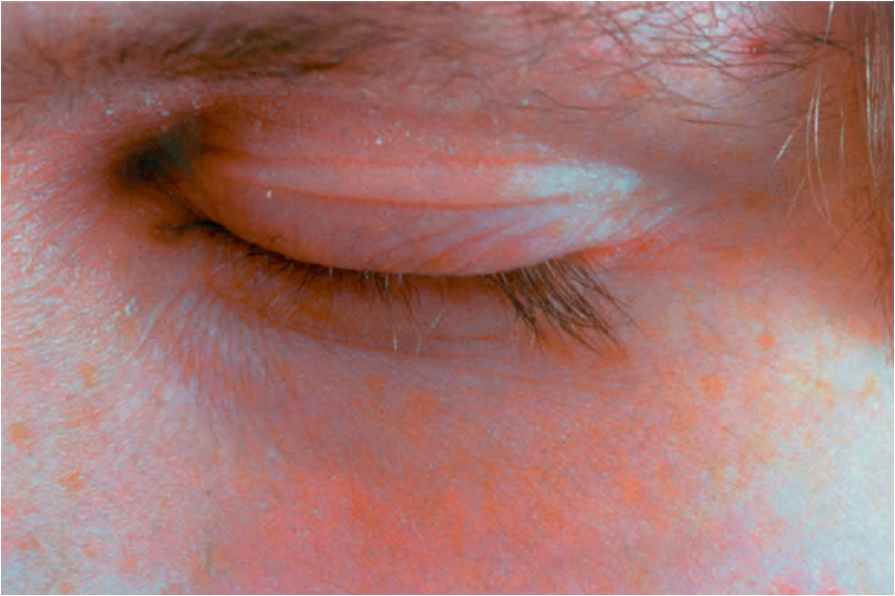
圖 22-78:拔毛癖 (Trichotillomania):許多睫毛已被拔除。Courtesy of the Institute of Dermatology, London, UK。
Fig. 22.78 Trichotillomania: many of the eyelashes have been pulled out. Courtesy of the Institute of Dermatology, London, UK.

圖 22-79:毛髮窗 (Hair window):剃除一塊 1.5 × 1.5 cm 的小範圍頭皮,然後於一週後評估,觀察是否有毛髮生長。Courtesy of M.S. Aluma, MD, Medellín, Colombia。
Fig. 22.79 Hair window: a small area of 1.5 × 1.5 cm of the scalp is shaved and then evaluated after a week to observe if there has been hair growth. Courtesy of M.S. Aluma, MD, Medellín, Colombia.
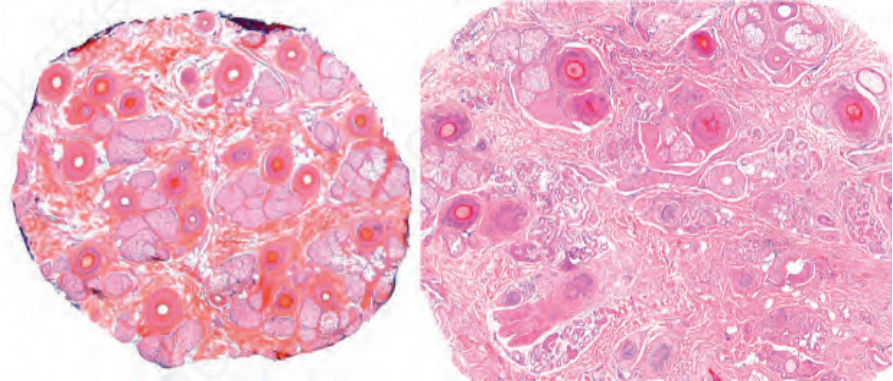
圖 22-80:拔毛癖 (Trichotillomania):除了殘留的生長期 (anagen) 與休止期 (telogen) 毛囊外,還有顯著的退行期 (catagen) 毛囊,其中央呈明亮的嗜伊紅性 (eosinophilic)。未見明顯發炎。
Fig. 22.80 Trichotillomania: in addition to residual anagen and telogen follicles, there are conspicuous catagen follicles with a bright eosinophilic center. No significant inflammation is seen.
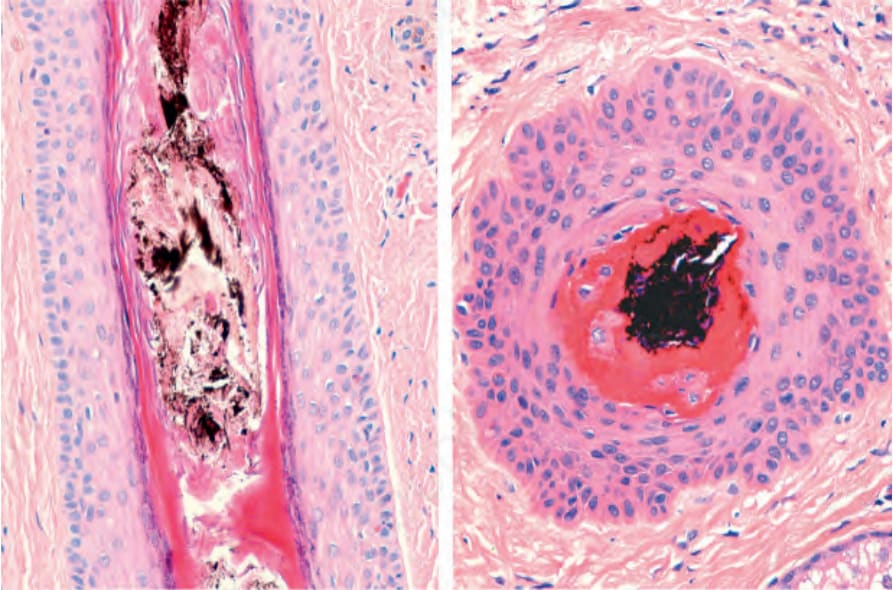
圖 22-81:拔毛癖 (Trichotillomania):注意漏斗部擴張 (infundibular dilation) 並伴有色素管型 (pigment cast)。
Fig. 22.81 Trichotillomania: note infundibular dilation with a pigment cast.
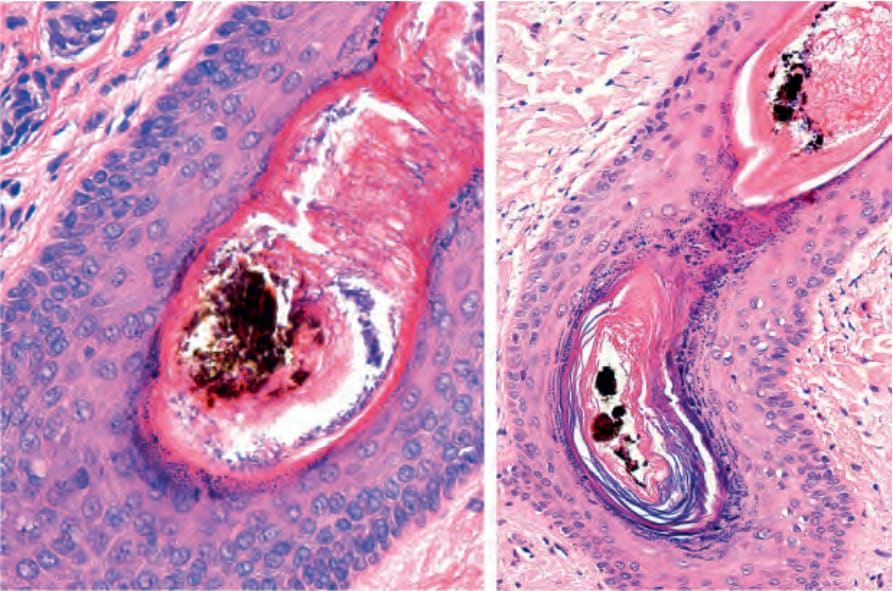
圖 22-82:拔毛癖 (Trichotillomania):有漏斗部擴張 (infundibular dilatation)、內毛根鞘 (inner root sheath) 厚度不規則、顯著的過度角化 (hyperkeratosis),以及一個色素管型 (pigmented cast)。
Fig. 22.82 Trichotillomania: there is infundibular dilatation, irregularity in the thickness of the inner root sheath, marked hyperkeratosis, and a pigmented cast.
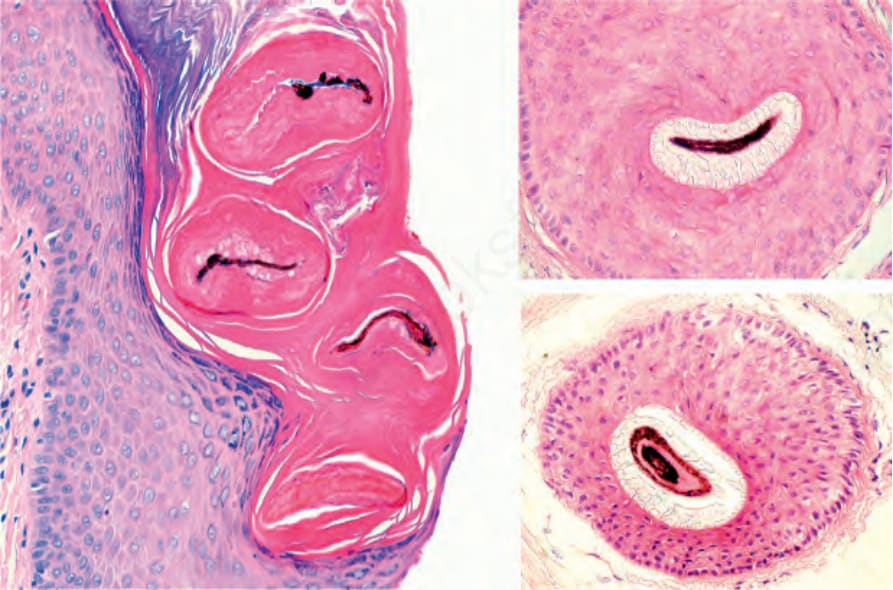
圖 22-83:拔毛癖 (Trichotillomania):漢堡徵 (hamburger sign)。左圖,注意毛幹內的色素聚集 (pigment aggregates)。右側為對照,注意在部分塌陷的毛囊管道中的色素聚集。
Fig. 22.83 Trichotillomania: hamburger sign. Left panel, note pigment aggregates within the hair shaft. On the right side, for comparison, note the pigment aggregates in a partially collapsed follicular channel.
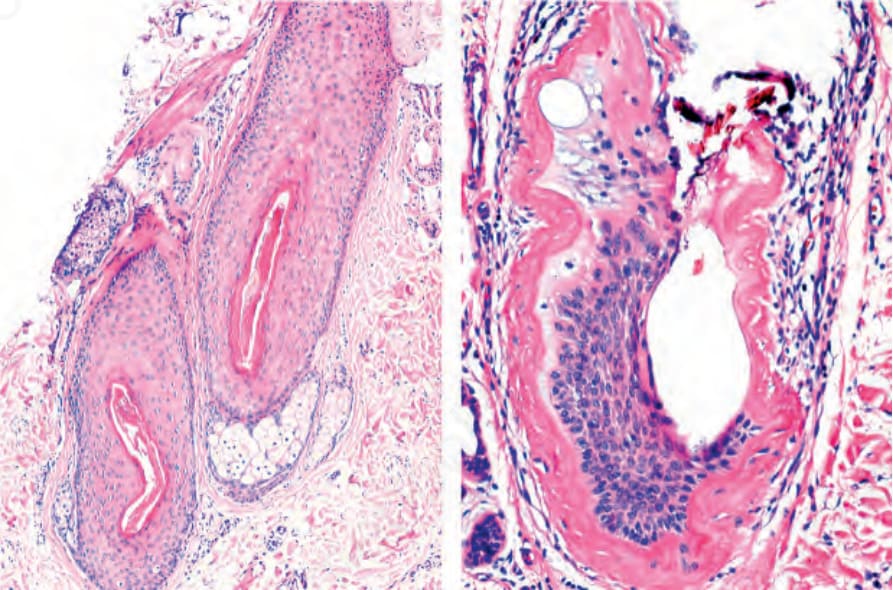
圖 22-84:毛軟化 (Trichomalacia):左圖,注意一個毛囊顯示其囊壁厚度不規則。右圖,此毛囊幾乎已喪失其全部結構完整性。Courtesy of the L.E. Muñoz, Cali, Colombia。
Fig. 22.84 Trichomalacia: left panel, note a hair follicle showing irregularities in the thickness of its wall. Right panel, this hair follicle has almost lost all its structural integrity. Courtesy of the L.E. Muñoz, Cali, Colombia.
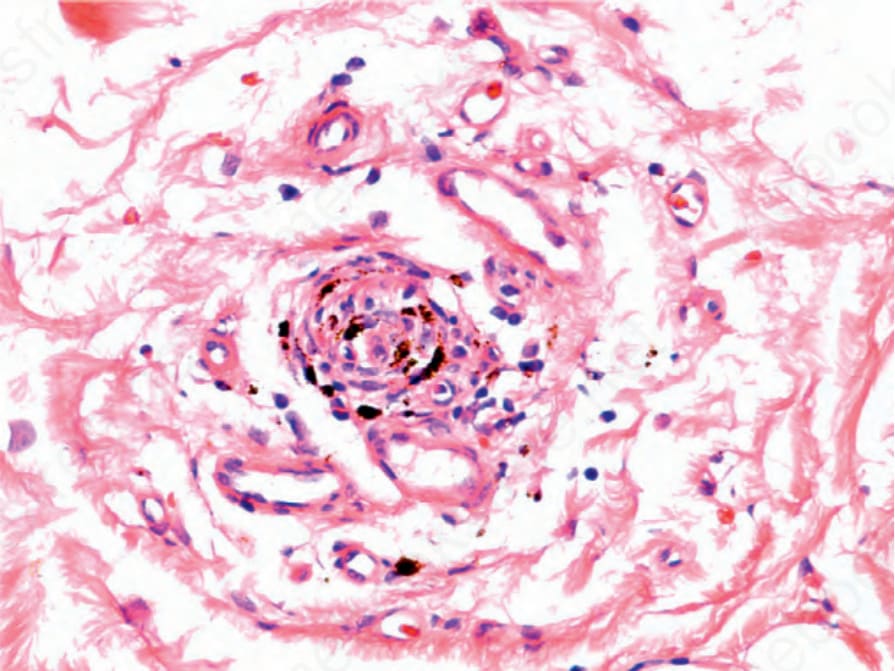
圖 22-85:拔毛癖 (Trichotillomania):色素性毛囊星狀體 (pigmented follicular stellae)。與圖 22.64 及 22.65 比較。
Fig. 22.85 Trichotillomania: pigmented follicular stellae. Compare with Figs 22.64 and 22.65.