Trichotillomania
Trichotillomania
Clinical features Trichotillomania was described in 1889 by Hallopeau.1 It is a variant of traumatic alopecia caused by traction and pulling of hair.2 It mainly affects
1078 Diseases of the hair
young women but can also be found in older adults and children, including toddlers.3–5 Although some patients admit to pulling their hair, in our experience the great majority emphatically deny this. For this reason, a thorough interview and detailed psychiatric history are usually required.
Trichotillomania constitutes a chronic mental illness, of variable intensity and presentation, which can lead to severe emotional and social limitations to the patient’s life. Trichotillomania shares some characteristics with obsessive-compulsive disorder.6 In the most severe cases, it can be associated with deeper personality disorders such as self-harming, trichophagia, and trichobezoar (Rapunzel syndrome).7,8 Occasionally, the compulsion to pull hair is not limited to the scalp but can involve other body sites including the pubis, the eyebrows, the eyelashes, and even the nostrils.9–11
Trichotillomania may be as common as obsessive-compulsive disorder and affect as many as 3% of the US population. Subclinical forms are also quite common, possibly affecting 1 in 10 Americans.12–14
There are two patterns of chronic hair pulling. The most severe and disfiguring is that in which patients pull off large amounts of hair during a brief period, and this is triggered by negative affective states. The least severe pattern is that of patients who engage in hair pulling during sedentary and social activities, such as reading, watching television, or talking on the telephone.15
The pattern of hair loss in trichotillomania is very variable, ranging from involvement of an isolated area (the ‘friar Tuck sign’) through to multiple geometric zones that may affect practically the entire scalp (Figs 22.75 and 22.76). In contrast to alopecia areata, the hair loss is typically incomplete. In every individual affected area there is hair loss, but this is not total, as the use of a magnifying glass shows residual small, broken, nonpigmented hairs. Sometimes there is evidence of erythema, pustule formation, or traumatic excoriations (Fig. 22.77). It is not infrequent to find other hair-bearing areas affected (Fig. 22.78).
Owing to the shortness of the hairs in this form of alopecia, it is usually not possible to obtain hairs by the hair-pull or hair-pluck techniques. Hairs evaluated by these techniques at the edges of the areas of alopecia are normal.
The hair-growth window technique is very useful in the diagnosis of trichotillomania. It involves shaving an area of 2.0 cm2 on the scalp such that the patient cannot pull hairs from this site (back of the head). If possible, this area should be chosen so that adjacent hairs may hide the shaved area (Fig. 22.79). A diagnosis of trichotillomania is confirmed if, by the end of a week, hairs are developing normally. Hair growth is evaluated after a period of 1 week only because at this stage normal hairs are still very short and the patient cannot reach them. The hair grows by about 1.0 cm per month, and in 1 week the length of the hair should average
1079 Nonscarring alopecias
At scanning magnification, the most salient features consist of very high percentage of catagen or telogen hair follicles, a number of normal hair follicles, and absence of inflammation (Fig. 22.80). The affected hair follicles are easily recognized because they contain dark-red keratin and the external root sheath displays extensive apoptosis (see Figs 22.26 and 22.29).
Pigment casts correspond to pigmented cells in the hair matrix and cortex, which due to traction are dislodged and become displaced to the hair canal, outer root sheath, fibrous streamers, and the dermal papilla.
In trichotillomania, pigment casts are seen at every level of the hair canal, mainly in the infundibulum and in the ostium, and are associated with hyperkeratosis (Figs 22.81 and 22.82). These casts are occasionally observed in alopecia areata, chemotherapy-induced alopecia, and pressure induced alopecia.20 They may be difficult to detect in poorly pigmented blond or red-haired individuals.21 Another morphological alteration observed has been the presence of a vertically oriented split within the hair shafts. This split defect is full of proteinaceous material and erythrocytes. The histologic image is reminiscent of a hamburger within a bun (the ‘hamburger sign’) (Fig. 22.83).22 Sometimes, the pigmented material takes other shapes similar to a zipper or a button and its buttonhole.20
2.5 mm. However, the individual hair growth rate may be heterogeneous on the scalp.16,17
In rare patients with extensive trichotillomania, a moth-eaten appearance is seen such that it may be necessary to exclude syphilis by serology.18
Histologic features The histologic features of trichotillomania are quite distinct and, with clinical correlation, enable the diagnosis to be made in the majority of cases.19 In horizontal and vertical sections it is fairly easy to observe the most important histologic components, which only affect terminal follicles. The miniaturized vellus and follicles are protected from being pulled out because of their short length. The most important histologic alterations are catagen follicles, pigmented casts, and traumatized and distorted hair follicles.
The best biopsies are obtained in the first 2 months after the hairs have been pulled. Many sections should be examined because only a few sections may show the characteristic changes.20
Traumatized and distorted hair follicles represent follicular structures that display different alterations. The most frequent changes consist of collapse of the inner root sheath, inter- and intrafollicular hemorrhage, and trichomalacia. The latter refers to distorted, small, and incompletely keratinized hair follicles with walls of uneven thickness (Fig. 22.84). They may show irregular pigmentation.23 Despite the extensive anatomical and physiological alteration of the hair follicles in trichotillomania, inflammation is minimal.24 Additional histologic findings include pigmented follicular stellae (Fig. 22.85).
1080 Diseases of the hair
Differential diagnosis The most important clinical and histologic differential diagnosis of traumatic alopecia, particularly trichotillomania, is alopecia areata. In the latter, one can also occasionally find pigmented casts and trichomalacia. However, in alopecia areata the latter component is minimal and there are telogen follicles, small anagen follicles, miniaturized hairs, and a peribulbar inflammatory cell infiltrate.25 Syphilitic alopecia may also resemble trichotillomania clinically, but the pigmented casts, trichomalacia, and absence of an inflammatory cell infiltrate in the latter condition usually afford their easy distinction. In difficult cases, however, serology is sometimes necessary.
Two other conditions that must be kept in mind in the differential diagnosis are trichotemnomania, an obsessive-compulsive habit to cut the hair with scissors or with a razor, and trichoteiromania, which results from perpetual rubbing of the scalp with fracturing of the hair shafts. Related to the latter is the appearance of frictional hair loss due to continuous pressure from items of clothing such as socks and trousers or the bed. The latter entities have no diagnostic histopathological features and show normal histology.26–28
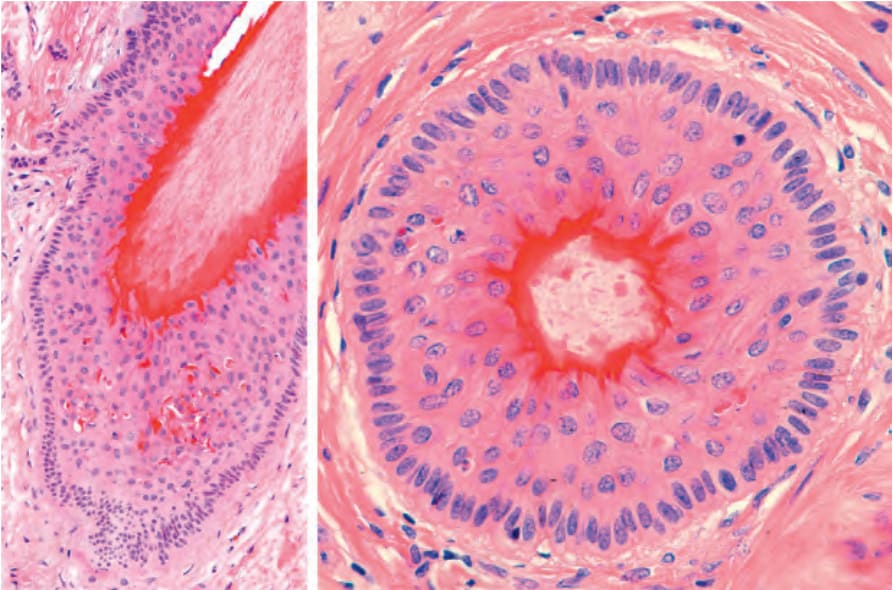
Fig. 22.26 Terminal hair follicle in catagen, vertical and horizontal sections: note the involution of the follicle and the deep red trichilemmal keratinization around the club-shaped hair shaft. The outer root sheath shows marked apoptosis. At the deepest part of the follicle, there is a hint of secondary germ formation.
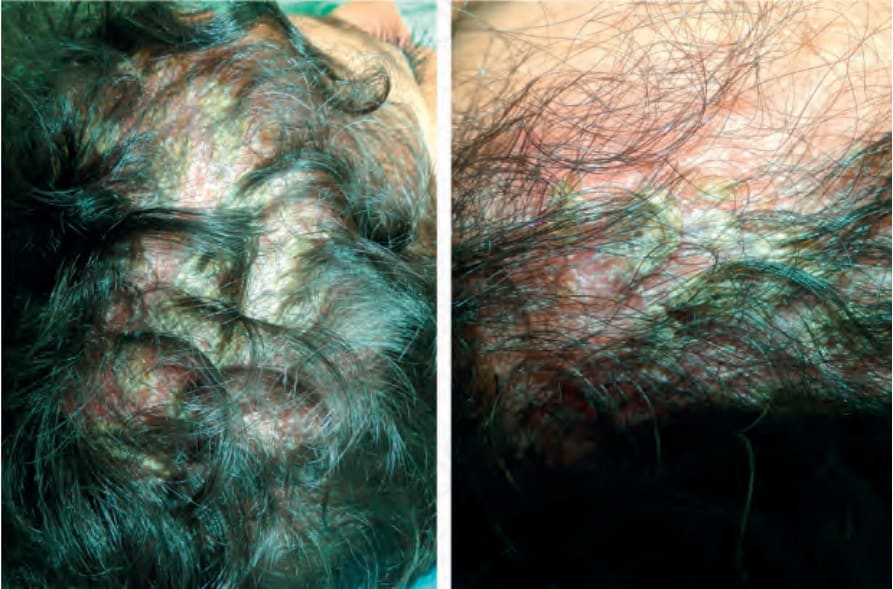
Fig. 22.72 Psoriasis. Note a thick scale covering an area of alopecia simulating tinea capitis. Courtesy of C. Velázquez, MD, CES, Medellín, Colombia.
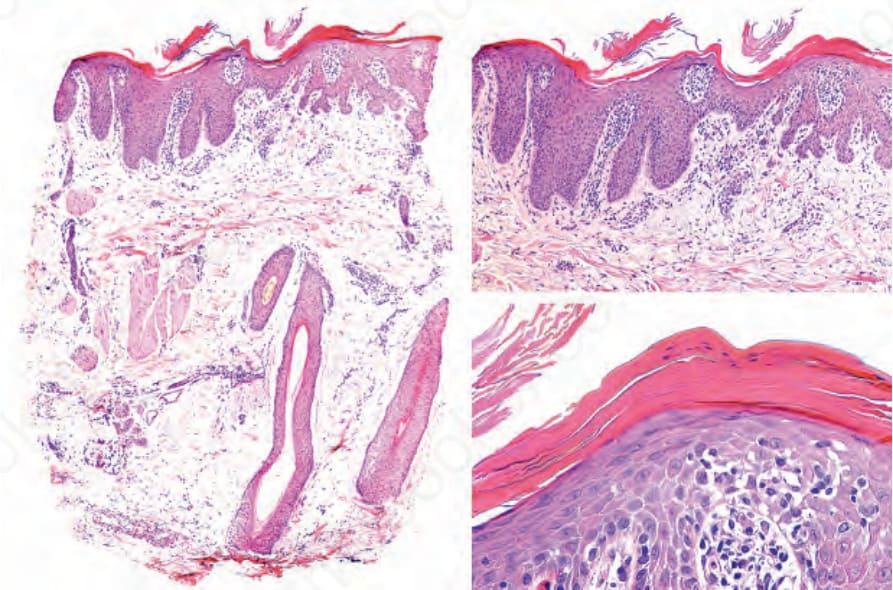
Fig. 22.73 Psoriasis. On the left the loss of sebaceous glands and follicular units is evident. On the right panel epidermal psoriatic changes including elongation of the rete ridges, hyperkeratosis, parakeratosis, hypogranulosis and corneal neutrophils.
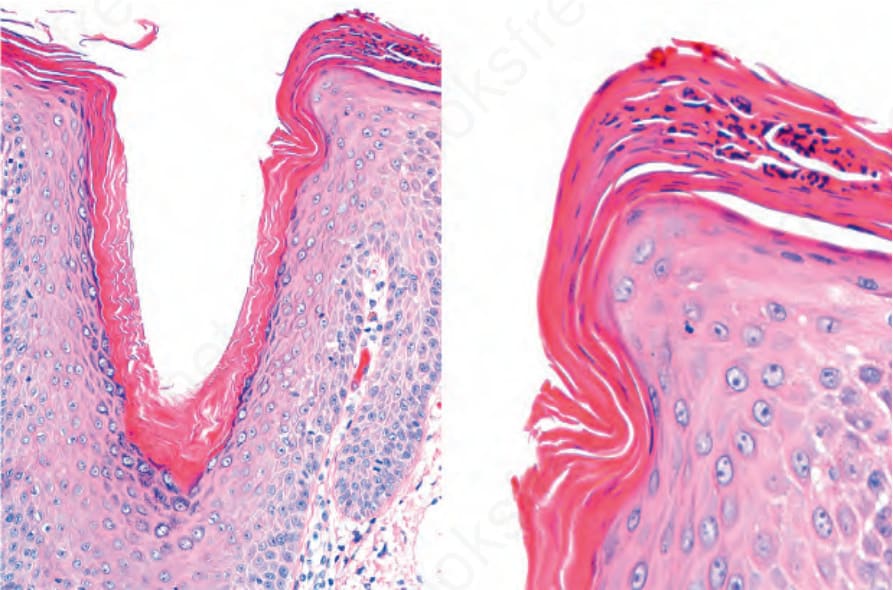
Fig. 22.74 Psoriasis of the scalp with changes simulating of seborrheic dermatitis. There is hyperkeratosis and parakeratosis with collections of neutrophils, more pronounced at the lip of the follicular ostium.

Fig. 22.75 Trichotillomania: mild involvement with very patchy hair loss. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
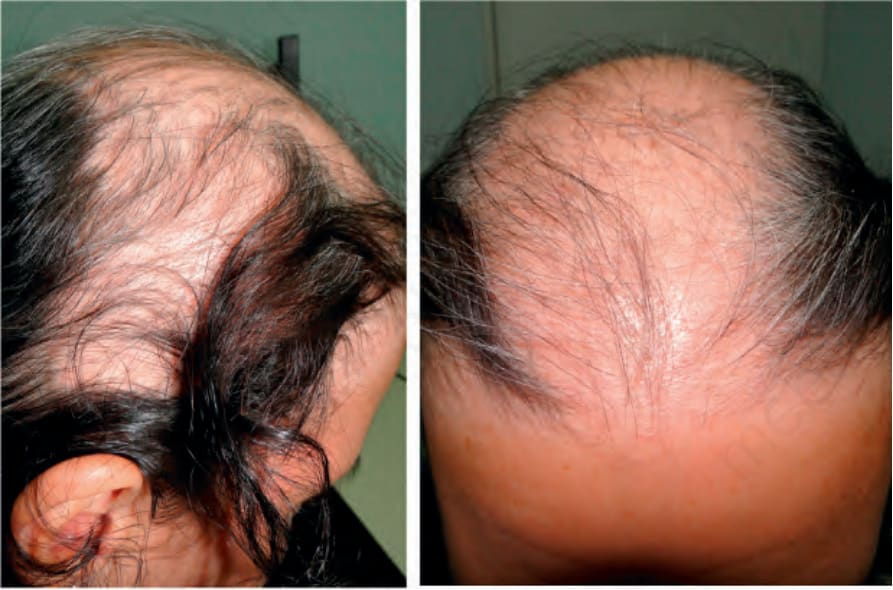
Fig. 22.76 Trichotillomania: severely affected young patient, with much more obvious and extensive hair loss with a bizarre pattern. Courtesy of C. Velázquez, MD, CES, Medellín, Colombia.

Fig. 22.77 Trichotillomania: note excoriations on the left side. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
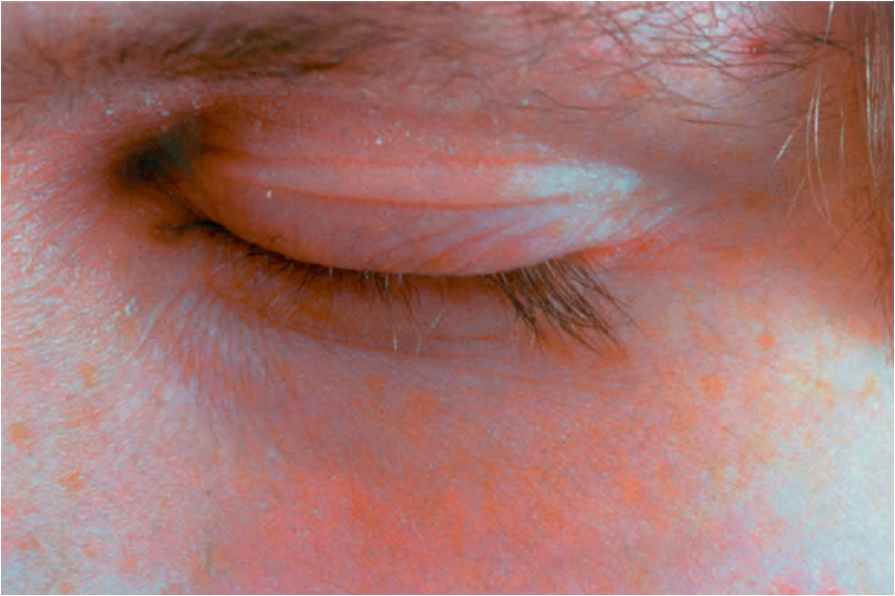
Fig. 22.78 Trichotillomania: many of the eyelashes have been pulled out. Courtesy of the Institute of Dermatology, London, UK.

Fig. 22.79 Hair window: a small area of 1.5 × 1.5 cm of the scalp is shaved and then evaluated after a week to observe if there has been hair growth. Courtesy of M.S. Aluma, MD, Medellín, Colombia.
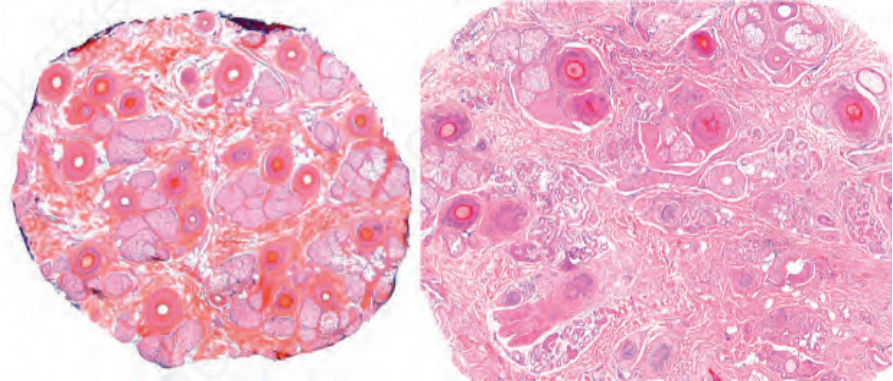
Fig. 22.80 Trichotillomania: in addition to residual anagen and telogen follicles, there are conspicuous catagen follicles with a bright eosinophilic center. No significant inflammation is seen.
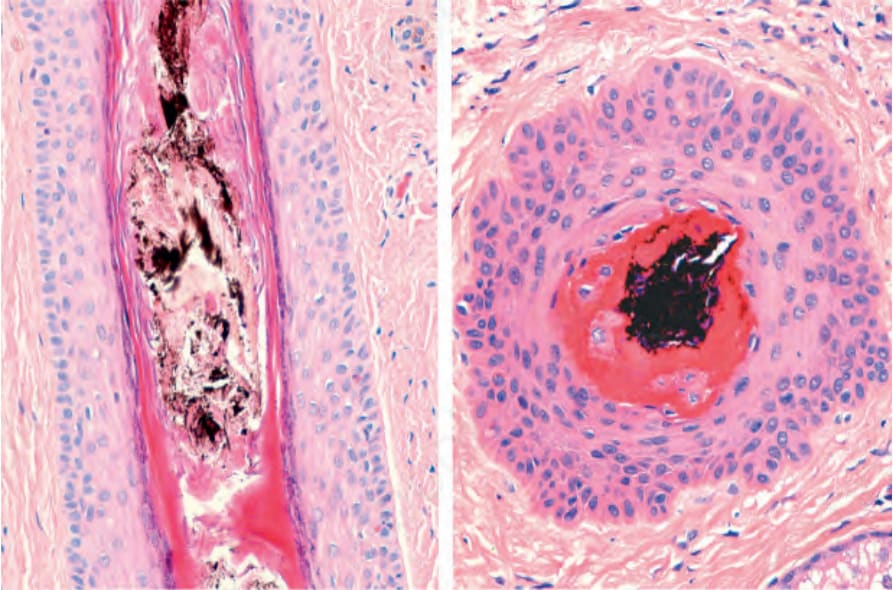
Fig. 22.81 Trichotillomania: note infundibular dilation with a pigment cast.
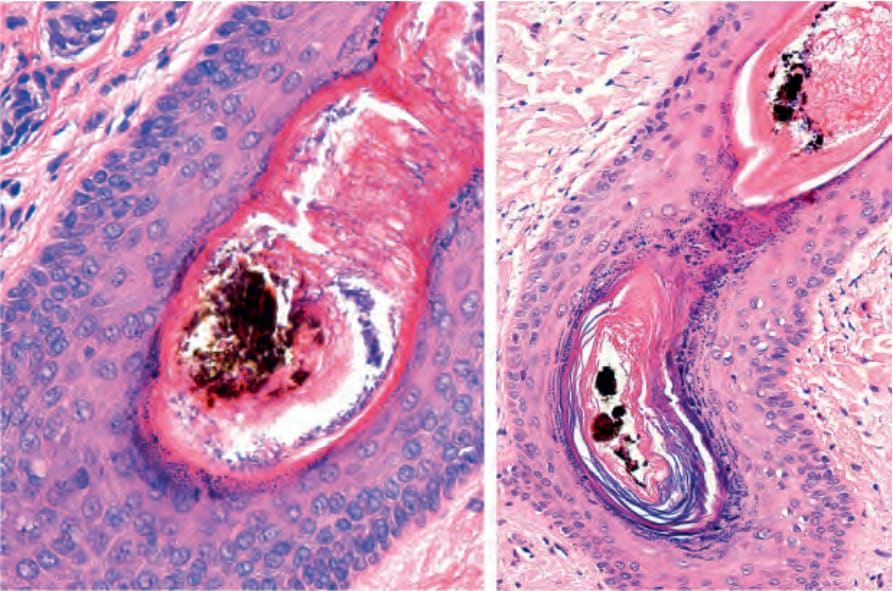
Fig. 22.82 Trichotillomania: there is infundibular dilatation, irregularity in the thickness of the inner root sheath, marked hyperkeratosis, and a pigmented cast.
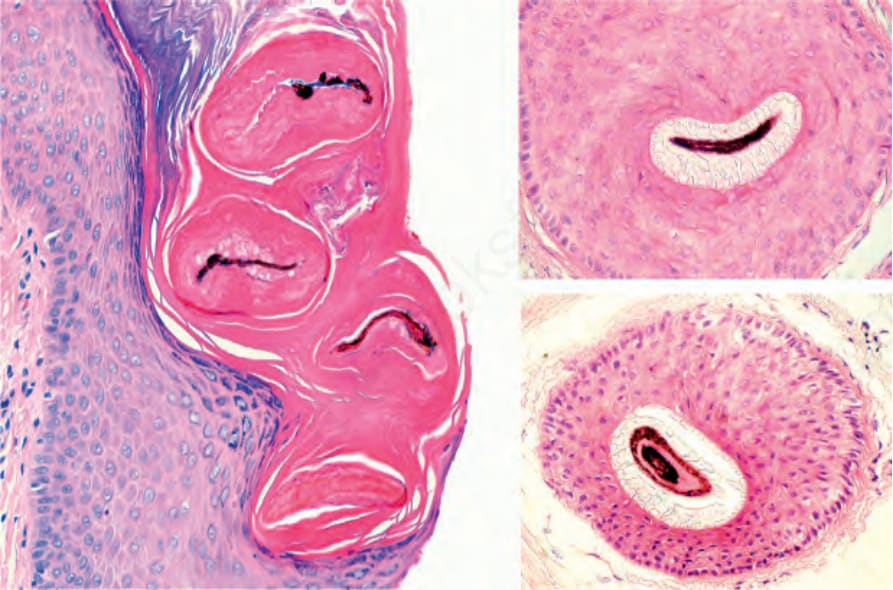
Fig. 22.83 Trichotillomania: hamburger sign. Left panel, note pigment aggregates within the hair shaft. On the right side, for comparison, note the pigment aggregates in a partially collapsed follicular channel.
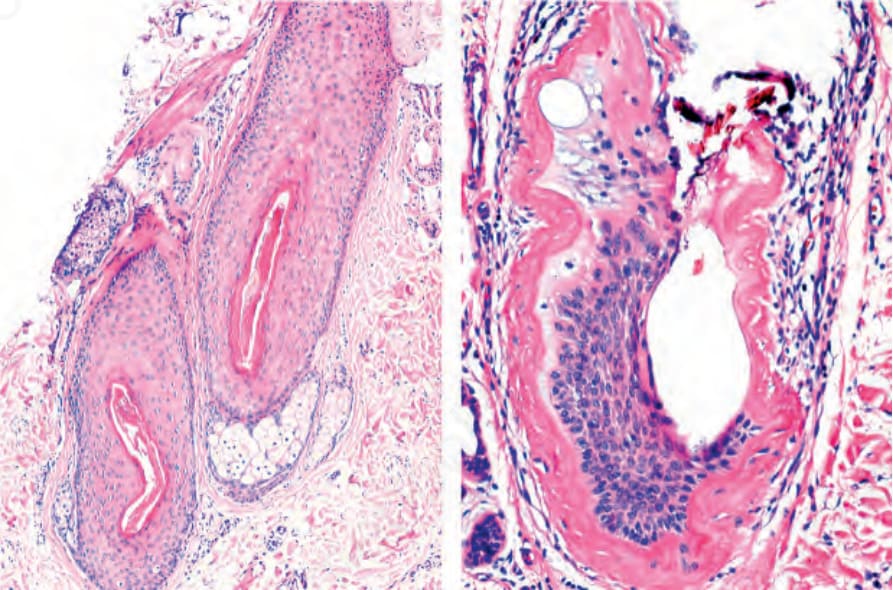
Fig. 22.84 Trichomalacia: left panel, note a hair follicle showing irregularities in the thickness of its wall. Right panel, this hair follicle has almost lost all its structural integrity. Courtesy of the L.E. Muñoz, Cali, Colombia.
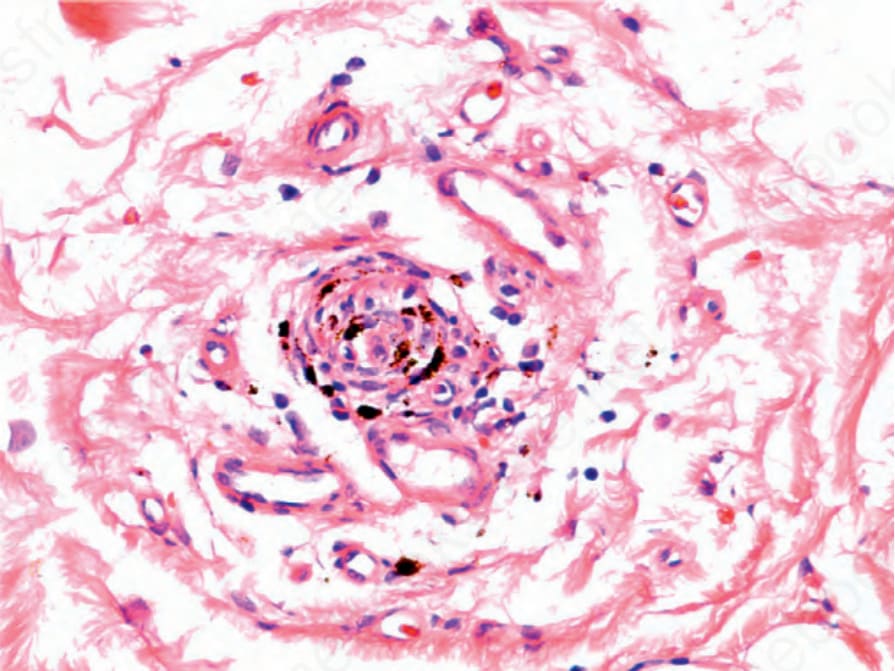
Fig. 22.85 Trichotillomania: pigmented follicular stellae. Compare with Figs 22.64 and 22.65.