圓禿 (Alopecia areata)
Alopecia areata
臨床特徵 (Clinical Features)
圓禿 (alopecia areata) 相當常見,影響高達 1% 的人口。有家族史的比例非常高,介於 10% 至 42% 的病例之間。本病較常見於 15 至 40 歲之間的個體,約 60% 的病例發生於 20 歲之前。本病在新生兒與幼童極為罕見。然而,例外情況下仍可能出現先天性病例。
顳部三角形禿髮 (temporal triangular alopecia) 曾被描述與下列情況相關:先天性皮膚發育不全 (aplasia cutis)、色素血管性斑痣性錯構瘤病 (phakomatosis pigmentovascularis)、唐氏症 (Down syndrome)、Klippel-Trénaunay syndrome、智能障礙與癲癇,以及一對母女病例、leopard syndrome,與合併腎臟及生殖器異常的先天性心臟病。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
本病的遺傳基礎尚不明確,但曾有人提出其為一種 paradominant 性狀。
侵犯程度差異極大,可從極輕微、難以察覺落髮的疾病,到極為嚴重、瀰漫性落髮波及整個頭皮甚至全身的病例 (Fig. 22.54)。任何長毛的表面皆可能受侵犯。典型病人表現為突然出現非瘢痕性禿髮 (nonscarring alopecia) 斑塊,呈現不同的型態:界線分明 (circumscribed)、顳枕部呈帶狀 (ophiasic)、額頂部呈帶狀的「sisaipho」型態 (ophiasis inversus) (Fig. 22.55),以及網狀 (reticular)。當斑塊擴展並融合、波及整個頭皮時,此外觀稱為全頭禿 (alopecia totalis) (Fig. 22.56)。若全身毛髮皆脫落,此情況則稱為全身禿 (alopecia universalis)。即使在 alopecia totalis 與 alopecia universalis 最嚴重的型態中,仍可觀察到孤立的小群未受侵犯的毛囊。Alopecia areata 偶可表現為類似急性休止期落髮 (acute telogen effluvium) 的型態,伴隨陽性拉髮試驗 (pull test) 與毛髮觸痛 (trichodynia) (alopecia areata incognita)。最終發展為 alopecia totalis 與 alopecia universalis 的病人比例不一,但約為 7%。Alopecia totalis 在兒童較常見。
顳部三角形禿髮的診斷通常依據臨床特徵。只有在診斷有疑問時才進行切片。可施行水平切片,並特別注意漏斗部 (infundibulum) 層級之最表淺切片。
表皮與真皮正常,但幾乎沒有終端毛 (terminal hairs),且毳毛 (vellus hairs) 數量增加。皮脂腺與外分泌腺 (eccrine glands) 正常。纖維狀殘跡 (fibrous stellae) 與發炎反應均缺如 (Fig. 22.53)。一般而言,其組織學外觀與正常皮膚切片非常相似。
鑑別診斷 (Differential Diagnosis)
鑑別診斷包括其他造成界線分明非瘢痕性禿髮的原因,特別是 alopecia areata、頭癬 (tinea capitis) 與拔毛癖 (trichotillomania)。在前者中,生長期 (anagen) 毛囊的毛球被淋巴球包圍與浸潤,且有終端與微小化 (miniaturized) 毛囊循環進入退化期 (catagen) 與休止期 (telogen)。在 tinea capitis 中,可見真菌微生物。
檢查受侵犯的頭皮通常顯示:除了毛髮缺失之外,皮膚外觀正常、毛囊開口保留,且無瘢痕證據 (Fig. 22.57)。然而,偶有病例可觀察到水腫與紅斑。
毛髮顏色可能看似正常,或顯示輕微變淡與失去光澤。在禿髮斑塊的周邊,典型可見驚嘆號毛 (exclamation mark hairs),這些毛髮短小,且愈接近頭皮愈逐漸變細。它們是非常具特徵性的表徵,但也可見於 trichotillomania。有時生長期毛囊受損極為嚴重,以致毛髮一冒出頭皮即斷裂。皮膚鏡 (dermoscopy) 發現包括黃點 (yellow dots),見於 95% 的病例。此過程通常侵犯有色素的毛髮。無色素毛髮似乎較具抗性,至少是暫時性的。這種選擇性黑毛脫落而灰白毛被保留的現象,可能造成快速白髮化的印象 (Marie Antoinette syndrome)。當毛髮重新生長時,往往呈白色或淺棕色,並緩慢恢復其正常顏色。例外情況下,會出現持續性的白毛。
Alopecia areata 若放過了眉部的先天性痣 (congenital nevus) 與火焰痣 (nevus flammeus),此現象稱為 Renbök 現象(反向 Koebner 現象,inverse Koebner phenomenon),並被解釋為一種局部型的遺傳性抗性。
Alopecia areata 病人可能出現指甲變化,包括點狀凹陷 (pitting)、斑點狀甲半月 (spotted lunula) 與紅色甲半月 (red lunula)。變化可見於一個、數個或全部指甲 (Fig. 22.58)。粗糙甲 (trachyonychia,又稱二十甲失養症 twenty-nail dystrophy) 發生於高達 3% 的病人。此失養症可能在禿髮發作之前、同時或之後出現。
Alopecia areata 曾與許多其他疾病相關。其中部分具有自體免疫病因,例如 Hashimoto thyroiditis、第 I 型(胰島素依賴型)糖尿病、Addison disease、白斑 (vitiligo)、遺傳性血小板減少症(假性 von Willebrand disease)、重症肌無力 (myasthenia gravis)、interleukin (IL)-1 受體拮抗劑基因之多型性、紅斑性狼瘡 (lupus erythematosus)、自體免疫多內分泌病變-念珠菌病-外胚層發育不良症候群(自體免疫多腺體症候群-1,autoimmune polyglandular syndrome-1)、常見變異型免疫缺乏症 (common variable immunodeficiency)、復發性多軟骨炎 (relapsing polychondritis)、服用 ciclosporine 的腎臟-胰臟移植受贈者,以及異體骨髓移植後。其他相關情況包括扁平苔癬 (lichen planus)、異位性體質 (atopy)、人類免疫缺乏病毒 (HIV) 感染、二十甲失養症、Down syndrome、巨細胞病毒 (cytomegalovirus) 與 Epstein-Barr virus 感染、兒童乳糜瀉 (celiac disease)、化學治療、interferon-alpha (IFN-α)、ribavirin、ciclosporine A、rifampicin、邊緣型類結核樣痲瘋 (borderline tuberculoid leprosy),以及眼部改變(圓錐角膜 keratoconus、無症狀點狀晶體混濁)。本病亦曾於 Clozapine 引起的高嗜酸性球血症、第 1 型猝睡症 (narcolepsy type 1) 中被觀察到,並可於疫苗接種後復發。數種生物製劑,如 etanercept、infliximab 與 adalimumab,與本病的出現或惡化有關。本病亦曾於一名 pili annulati 病人中發生。嚴重 alopecia areata 的病人似乎有較高的頸後火焰痣 (nuchal nevus flammeus) 發生率。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
實驗研究顯示,alopecia areata 基本上是一種器官特異性自體免疫疾病,被認為源自毛囊免疫豁免 (hair follicle immune privilege) 的崩潰,由細胞免疫驅動,而自體抗體產生則代表一種次發性現象。曾有文獻描述對多種抗原的自體抗體,包括平滑肌細胞、胃壁細胞 (gastric parietal cells)、甲狀腺細胞,以及生長期毛囊的成分。
目前尚不清楚本病的誘發是源自外源性或內源性抗原的暴露,亦不清楚其是否代表免疫反應對正常或異常表位 (epitopes) 的後果。然而,研究顯示其致病機轉至少涉及四個事件:
- 生長期毛囊未能維持其豁免免疫(內毛根鞘 inner root sheath 與毛基質 hair matrix 不表現、或僅極低度表現主要組織相容性複合體第 Ia 類抗原,並維持活躍的 NK 細胞抑制),導致表位暴露而啟動免疫反應,
- 抗原呈現、淋巴球對抗原呈現細胞的活化與反應,
- 活化的發炎細胞遷移並浸潤毛囊,
- 發炎細胞浸潤對毛囊造成損傷。
有人提出神經營養因子 (neurotrophins) 在本病的致病機轉中扮演角色。由於神經營養因子及其受體在 alopecia areata 的免疫細胞亞群中呈差異性表現,這些蛋白在致病機轉中的角色似乎相當可能。
Alopecia areata 在遺傳相關個體中頻率增加,顯示本病與遺傳相關。在一般族群中,本病並不呈現孟德爾式 (mendelian) 表現型態,因為其產生的表現型展現不同程度的落髮。曾有人提出 alopecia areata 的表現涉及多個基因的複雜交互作用,其中主要基因控制對本病的易感性,而其他次要基因則修飾表現型。
Alopecia areata 的預後不一,且對個別病人而言相當難以預測。然而,已觀察到在曾經歷毛髮再生、且發作之間有長期緩解的病人中,預後傾向良好。可預期 34–50% 的病人在 1 年內出現自發性緩解,儘管幾乎所有病人都會經歷一次以上的疾病發作。相反地,曾有持續性落髮、或短暫或不完全緩解的病人則預後不佳。初診時 alopecia areata 的嚴重度以及對治療的反應是重要的預後因子。下列病人的展望特別不佳:青春期前發病者、有本病家族史者(見於 25% 的病例)、以及罹患 alopecia totalis 與 alopecia universalis 者。異位性體質的病人似乎罹患較嚴重型態的 alopecia areata。
許多具自體免疫基礎的疾病曾與特定的人類白血球抗原 (HLA) 相關。Alopecia areata 已被研究與 HLA 第 I 類及第 II 類的關聯。最相關的關聯見於 HLA 第 II 類抗原(HLA-DR、-DQ、-DP)。此遺傳關聯的分子基礎,得到下列事實的支持:HLA 結合並將源自自體及外來蛋白抗原的胜肽呈現給免疫系統以供辨識與活化。在某項研究所評估的全部病例中,超過 80% 對抗原 DQB103 (DQ3) 呈陽性,顯示此抗原為易感性的標記。此外,在罹患 alopecia totalis 與 universalis 的病人中,抗原 DRB10401 與 DBQ1*0301(DR4 與 DQ7)的頻率顯著增加。HLA-DR5 與早發及嚴重型 alopecia areata 相關。其他相關的 HLA 基因為 NOTCH4 與 MICA。與本病相關的非 HLA 基因為 PTPN22 與 AIRE。
在最近一項由美國 alopecia areata 全國登錄資料庫之遺傳資料庫所支持的基因體研究中,鑑定出 139 個與 alopecia areata 顯著相關且具多型性的核苷酸。共有八個不同的相關區域。其中一個區域對應於早已熟知的 HLA 複合體。亦發現七個基因體基因座 (loci)。其中五個表現於免疫系統,兩個表現於毛囊。有趣的是,這些基因與第 I 型糖尿病、多發性硬化症、類風濕性關節炎及乳糜瀉等疾病較相關,而非與當初認為相關的乾癬 (psoriasis) 與白斑疾病相關。這些疾病呈現一種統一的機轉,稱為 ULBP3,即標的器官中危險訊號 (danger signal) 調控的增強。在正常情況下,ULBP3 不見於毛囊,但在 alopecia areata 受侵犯的毛囊中則相當顯著。這些蛋白會吸引帶有 NKG2D 受體標記的殺手細胞。

圖 22-54:(A, B) 圓禿 (alopecia areata):典型的環狀非發炎性禿髮區域。Courtesy of L.M. Gómez, MD, UPB, Colombia.
Fig. 22.54 (A, B) Alopecia areata: typical annular noninflammatory areas of alopecia. Courtesy of L.M. Gómez, MD, UPB, Colombia.

圖 22-55:圓禿 (alopecia areata):(A) 此枕部寬帶狀的禿髮稱為 ophiasis。(B) 額頂部類似的型態稱為 ophiasis inversus 或「sisaipho」型態。Courtesy of the Institute of Dermatology, London, UK.
Fig. 22.55 Alopecia areata: (A) this broad band of alopecia in the occipital region is known as ophiasis. (B) A similar pattern in the frontoparietal region it is known as ophiasis inversus, or a ‘sisaipho’ pattern. Courtesy of the Institute of Dermatology, London, UK.
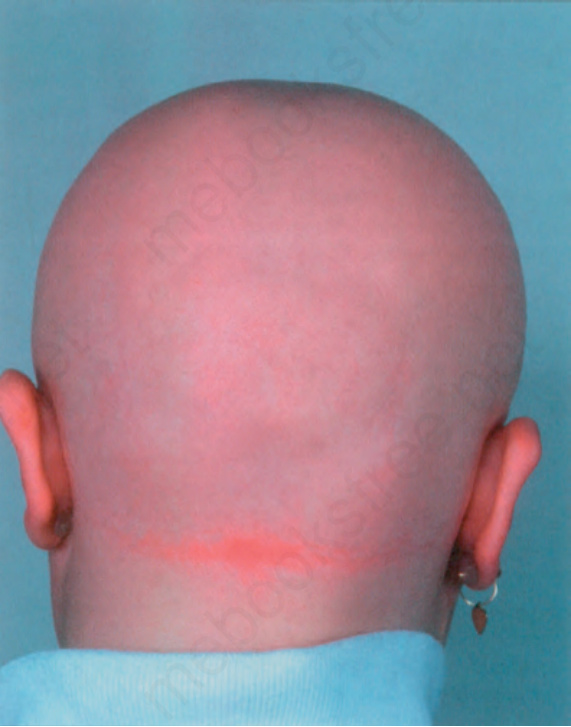
圖 22-56:全頭禿 (alopecia areata totalis):此病人頭皮毛髮完全脫落。Courtesy of the Institute of Dermatology, London, UK.
Fig. 22.56 Alopecia areata totalis: in this patient, there is complete loss of scalp hair. Courtesy of the Institute of Dermatology, London, UK.
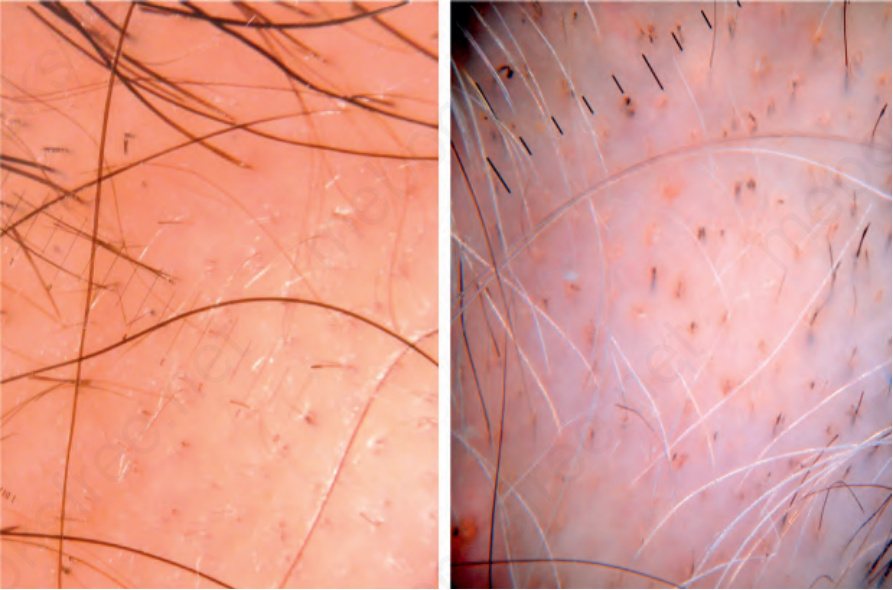
圖 22-57:圓禿皮膚鏡 (alopecia areata dermoscopy):注意毛囊密度正常且毛囊開口未消失。可見一些微小化毛囊 (miniaturized hair follicles) 與一根驚嘆號毛 (exclamation mark hair)。右側影像中可觀察到黃點 (yellow dots)。儘管有色素毛髮脫落,灰白毛仍持續存在。亦可見一些驚嘆號毛。Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
Fig. 22.57 Alopecia areata dermoscopy: note that the follicular density is normal and the opening of the follicles have not been lost. There are some miniaturized hair follicles and an exclamation mark hair. On the right panel, yellow dots are observed. The gray hairs have persisted despite the loss of the pigmented hair. There are also some exclamation mark hairs. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.

圖 22-58:圓禿 (alopecia areata):此病人指甲嚴重受侵犯(粗糙甲 trachyonychia)。Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.
Fig. 22.58 Alopecia areata: in this patient, there is severe involvement of the nails (trachyonychia). Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.
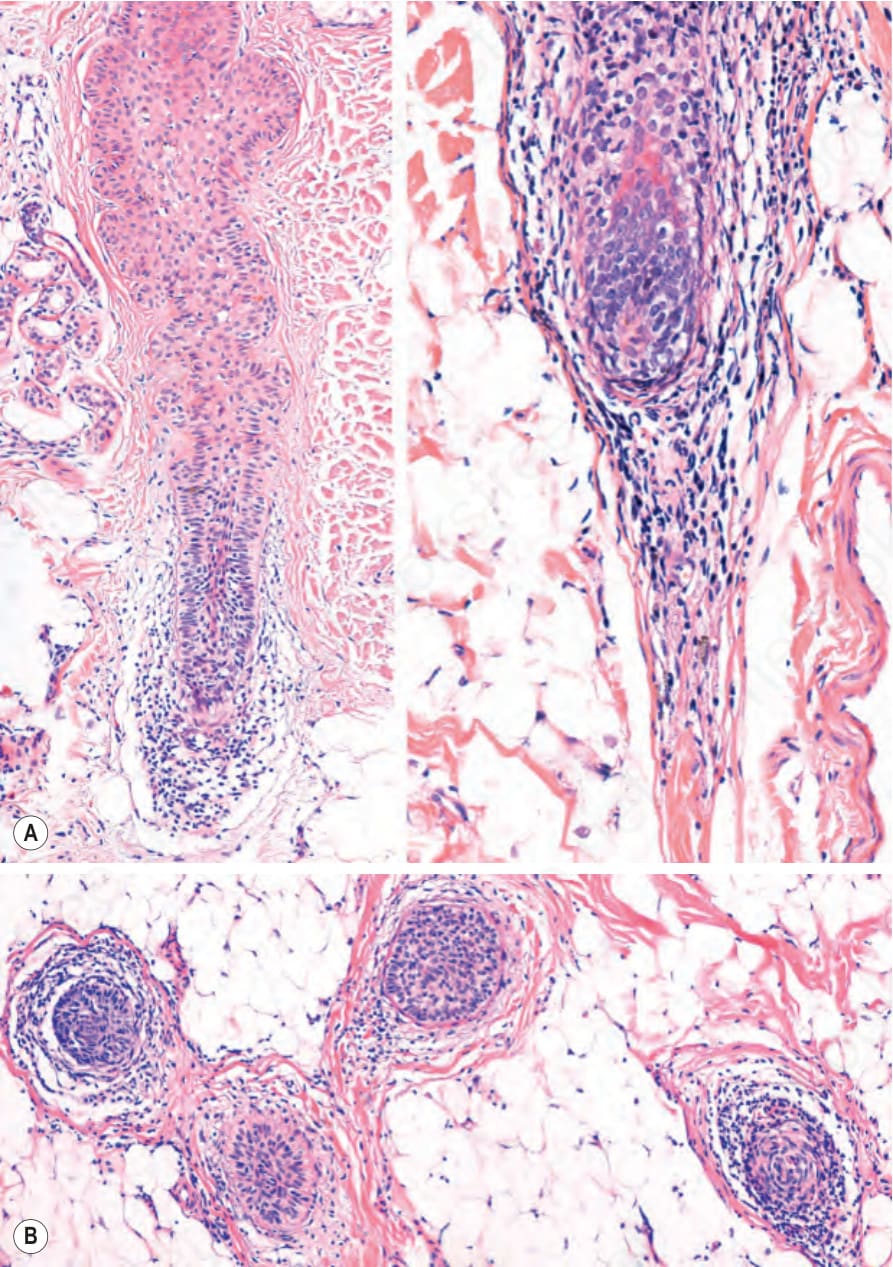
圖 22-62:圓禿 (alopecia areata):退化中的毛囊。(A) 垂直切片。右側毛囊中有毛球淋巴球浸潤,亦波及毛囊殘跡 (follicular stella)。(B) 水平切片。皮下組織中的毛囊伴有強度不一的淋巴球浸潤。
Fig. 22.62 Alopecia areata: hair follicle in involution. (A) Vertical section. In the follicle on the right there is a hair bulb lymphocytic infiltrate which also involves the follicular stella. (B) Horizontal section. Hair follicles in the subcutaneous tissue with a lymphocyte infiltrate of variable intensity.

圖 22-53:(圖說烘焙於圖內)
Fig. 22-53 (caption embedded in image / 圖說烘焙於圖內)
It is important to remember that the histopathological features depend on the stage of the disease.
切片的最佳取材部位是活動性病灶的周邊。當需要選擇最活躍的區域時,拔取試驗(拉髮試驗 hair-pull tests)與皮膚鏡很有用,因為可觀察到驚嘆號毛、黃點或黑點。
所有在垂直切片中描述的 alopecia areata 變化,在水平切片中觀察得更清楚 (Fig. 22.59)。對於毛球淋巴球浸潤尤其如此。然而,發炎浸潤並非總是可見。觀察到此項及其他組織學變化的頻率,取決於進行切片時疾病的階段。
壓力對致病機轉的影響尚不明確且具爭議,儘管曾有人提出壓力可觸發本病。已觀察到 substance P 與神經生長因子 (nerve growth factor) 可能透過角質細胞凋亡 (keratinocyte apoptosis)、抑制毛囊增殖以及誘導退化期,作為壓力誘導之毛髮生長抑制效應的關鍵媒介。
早期階段 (Early stages)
在疾病的早期階段,毛球周圍 (peribulbar) 發炎浸潤強烈 (Fig. 22.60)。然而,浸潤逐漸減少。
實驗室檢查通常並非診斷所必需,但在偵測相關情況、特別是自體免疫疾病時可能有價值。拉髮與拔髮試驗 (hair-pull and hair-pluck tests) 顯示休止期與失養生長期 (dystrophic anagen) 毛髮數量增加。殘餘的生長期毛髮呈失養狀態,因為持續的發炎過程導致過早轉變為退化期與休止期。此縮短的生長週期導致許多終端毛囊具有角化不良的短毛幹,容易斷裂(驚嘆號毛)。
組織學上,alopecia areata 以四項基本特徵為特點:
- 初始階段毛囊單位 (follicular units) 與毛囊數量正常,但在頑固性及最慢性階段毛囊喪失,
- 退化期與休止期毛囊數量增加,
- 嚴重度不一的淋巴球浸潤,侵犯生長期毛囊的毛球以及退化期與休止期的毛囊殘跡 (follicular stellae),
- 在較慢性及頑固性型態中,毛囊傾向微小化。
is an increase in the number of catagen and telogen hair follicles. 休止期計數可能超過休止期落髮 (telogen effluvium) 所見 (Fig. 22.61)。毛囊在毛球周圍區域顯示程度不一的發炎性淋巴球浸潤 (Figs 22.60 and 22.62)。即使在較活動性的病灶中,此浸潤偶爾也可能非常輕微。後一特徵在本病的非典型、incognita 與 ophiasic 型態中特別明顯 (Fig. 22.63)。殘跡與毛球內出現嗜酸性球 (eosinophils) 曾被描述為早期且典型的特徵。最早的毛囊變化包括中央位置的基質上部上毛球區 (supramatrical upper bulbar region) 結構完整性喪失,以及毛球萎縮。毛基質被淋巴球浸潤,並有色素失禁 (pigment incontinence)、基質細胞壞死 (matrix cell necrosis) 與空泡性損傷。發炎浸潤在終端毛囊中特別顯著,其毛球位於皮下組織 (Fig. 22.64)。色素失禁可能非常明顯,並導致在變形的毛球與毛囊束帶 (follicular streamer) 中形成黑色素團塊(色素鑄型 pigment casts) (Fig. 22.65)。此浸潤由 CD4+ 與 CD8+ T 淋巴球混合組成 (Fig. 22.66)。
在毛囊上部、表皮內,可觀察到充滿角質的擴張漏斗部 (dilated infundibulae),對應臨床所見的黃點 (Fig. 22.67 and see Fig. 22.57)。在水平切片中,這些可能呈現瑞士起司 (swiss cheese) 型態。
免疫螢光 (immunofluorescence) 研究顯示,沿毛囊下部的基底膜有 C3、IgG 與 IgM 的沉積。一旦毛囊進入退化期並進展至休止期,發炎細胞浸潤即減少。
毛囊淋巴球浸潤伴隨著進展至退化期與休止期。在此之後,毛囊迅速回到生長期,週期重新開始。由於此持續性週期以及伴隨的發炎過程,毛囊經歷兩項重要的形態學變化:
- 毛髮軟化 (trichomalacia),特徵為短而角化不完全的(鉛筆尖 pencil-point)毛髮,易受創傷影響,
- 部分生長期毛囊的微小化。
晚期階段 (Late stage)
在疾病的晚期階段,發炎減少,並出現眾多微小化毛囊與休止期毛囊。微小化毛囊的數量隨慢性化而增加,這些毛囊可能類似晚期生長期 (late anagen stage) 的毛囊。此類毛髮見於真皮中部或上部,曾被描述為 nanogen。它們代表毳毛與終端生長期毛囊之間的中間階段。在水平切片中,一般不產生毛幹,儘管偶爾會產生極細且角化不完全的型態,此與頭皮所觀察到的空漏斗部 (empty infundibula) 相關。在垂直切片中,毛幹的近端 (proximal end) 呈現參差不齊的外觀,而非正常的杵狀 (club shape)。這些毛囊有時可同時展現生長期、退化期與休止期的組織學特徵,並以有絲分裂活性 (mitotic activity) 與凋亡 (apoptosis) 的形式呈現生長與退化的證據 (Fig. 22.68)。
nail fold, nail matrix, nail bed, and hyponychium. 罕見情況下,其組織學與扁平苔癬 (lichen planus) 無法區別。
鑑別診斷 (Differential Diagnosis)
Alopecia areata 的鑑別診斷依落髮的臨床型態為侷限性或瀰漫性而有所不同。
在長期 alopecia areata 中,大多數毛囊處於退化期與休止期。由於發炎浸潤不侵犯處於這些生長階段的毛囊,皮下組織中可能無發炎 (Fig. 22.69)。
不活動性 alopecia areata 可類似雄性禿 (androgenetic alopecia),伴有許多微小化毛囊 (Fig. 22.70)。
深層真皮與皮下組織中存在眾多殘跡 (stellae),這些可能伴隨發炎細胞浸潤與黑色素 (Fig. 22.71)。在某些病例中,可能有毛囊被發炎細胞浸潤破壞,且此與組織球 (histiocytes) 及巨細胞 (giant cells) 相關 (see Fig. 22.64)。
在表現粗糙甲 (trachyonychia) 的病人中,指甲切片通常顯示淋巴球浸潤,伴有外滲 (exocytosis) 與海綿水腫 (spongiosis),侵犯近端甲褶 (proximal nail fold)、甲基質 (nail matrix)、甲床 (nail bed) 與下甲皮 (hyponychium)。
在表現為侷限性落髮區域的病例中,鑑別診斷包括 trichotillomania、triangular temporal alopecia、梅毒 (syphilis)、盤狀紅斑性狼瘡 (discoid lupus erythematosus)、毛髮扁平苔癬 (lichen planopilaris)、額部纖維化禿髮 (frontal fibrosing alopecia)、假性斑禿 (pseudopélade)、tinea capitis,以及乾癬性禿髮 (psoriatic alopecia)。
Trichotillomania 可能與 alopecia areata 極為相似,但前者在顯微鏡檢查中顯示較多色素鑄型 (pigmented casts)、缺乏微小化毛髮,以及極少的發炎浸潤。Triangular temporal alopecia 在臨床或組織學上均無發炎證據,且休止期或退化期毛囊無過量增加。梅毒性禿髮 (alopecia syphilitica) 可能非常相似,但臨床上其斑塊鮮少顯示毛髮完全缺失。組織學檢查亦可能有困難,因為兩種情況皆顯示毛球周圍發炎細胞浸潤。嗜酸性球在梅毒中不常見,但漿細胞 (plasma cells) 傾向顯著。在困難病例中,血清學檢查往往是必要的。
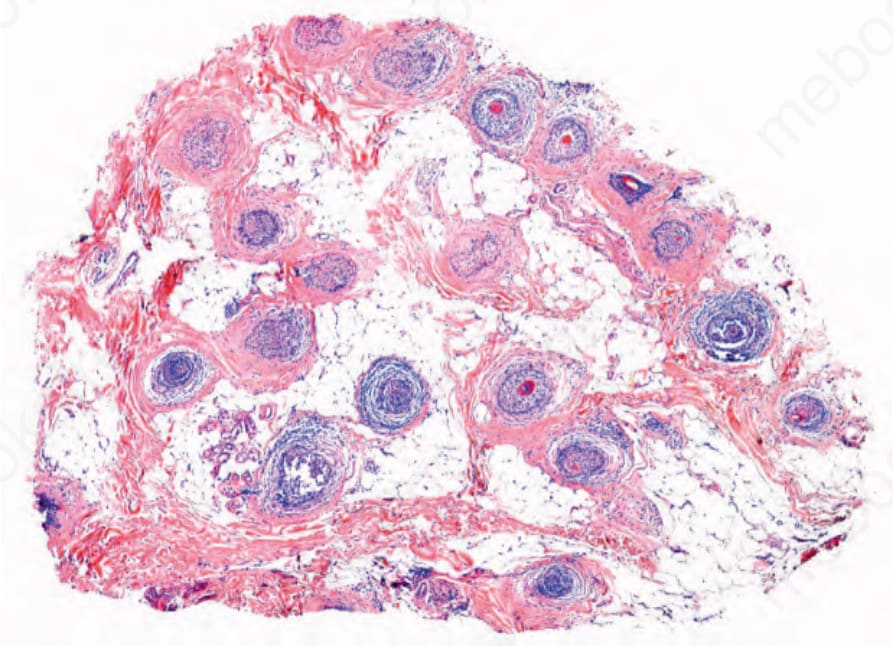
圖 22-59:圓禿 (alopecia areata):水平切片顯示毛囊密度接近正常;左上方某些毛囊處於退化期與休止期。Courtesy of J.C. Perez, MD, HPTU, Medellín, Colombia.
Fig. 22.59 Alopecia areata: Horizontal section displays a near normal density of hair follicles; some of the follicles on the left upper side are in catagen and telogen. Courtesy of J.C. Perez, MD, HPTU, Medellín, Colombia.
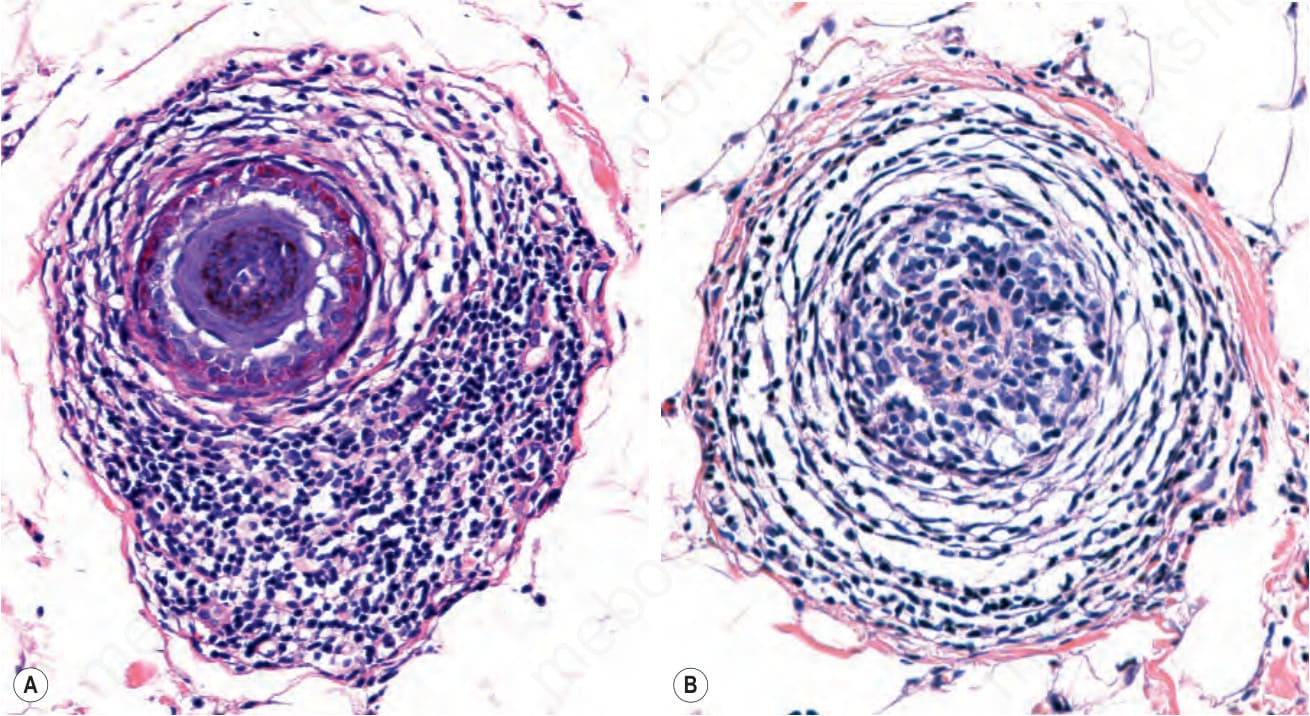
圖 22-60:(A, B) 圓禿 (alopecia areata):毛球周圍淋巴球浸潤的高倍視野,有時被稱為「蜂群 (swarm of bees)」。注意(由左至右)隨著毛球消失,發炎浸潤變得較不緻密。
Fig. 22.60 (A, B) Alopecia areata: high-power view of the peribulbar lymphocytic infiltrate, which is sometimes referred to as ‘swarm of bees’. Note (from left to right) that as the pili bulb disappears the inflammatory infiltrate becomes less dense.
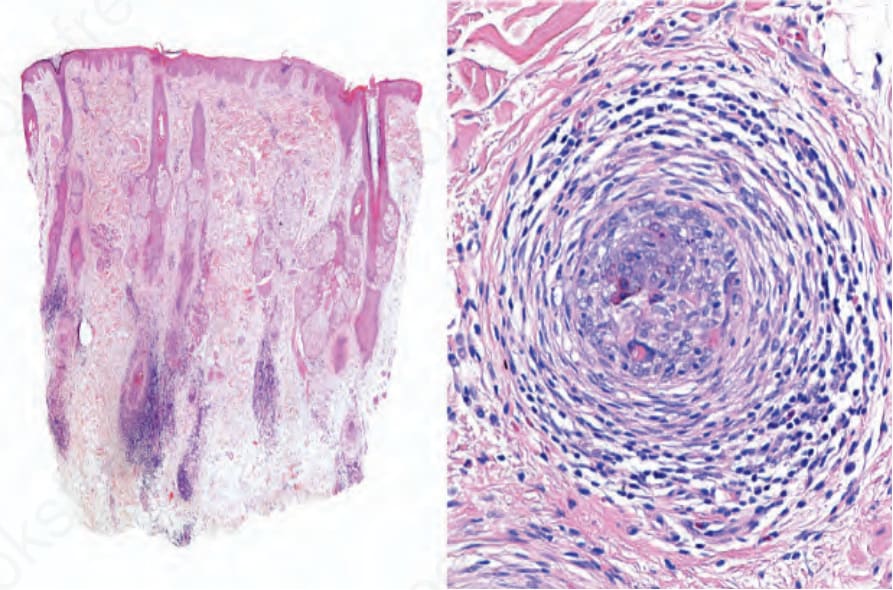
圖 22-61:圓禿 (alopecia areata):退化期-休止期毛球的垂直與水平切片。休止期殘餘中仍存在發炎浸潤。
Fig. 22.61 Alopecia areata: vertical and horizontal sections of catagen-telogen hair bulbs. The inflammatory infiltrate is still present in the telogen remnants.
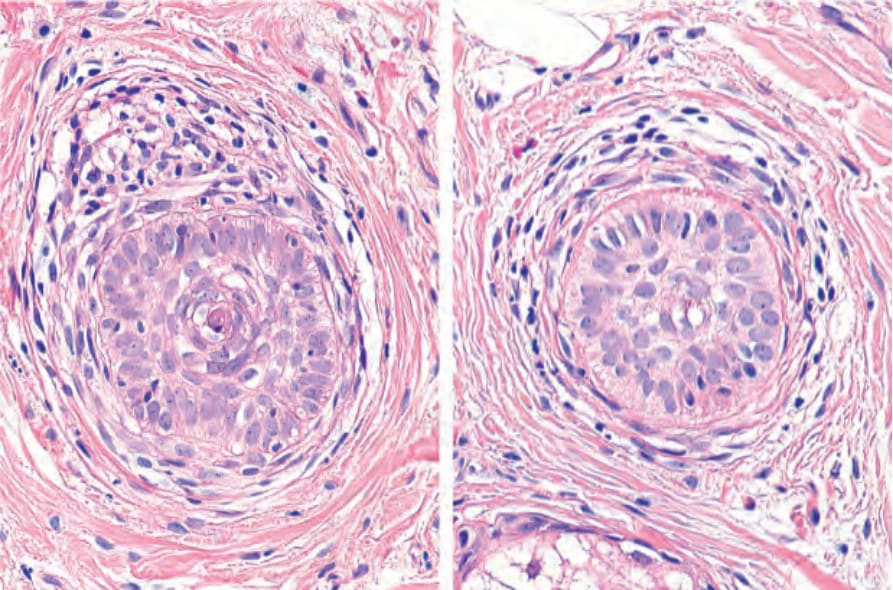
圖 22-63:Alopecia areata incognita:處於休止期的毛囊。右側毛囊呈現 nanogen 毛囊的特徵。可見伴隨嗜酸性球與肥大細胞 (mast cells) 的淋巴球浸潤。
Fig. 22.63 Alopecia areata incognita: follicles in telogen. The hair follicle on the right displays features of a follicle in nanogen. There is a lymphocytic infiltrate associated with eosinophils and masts cells.
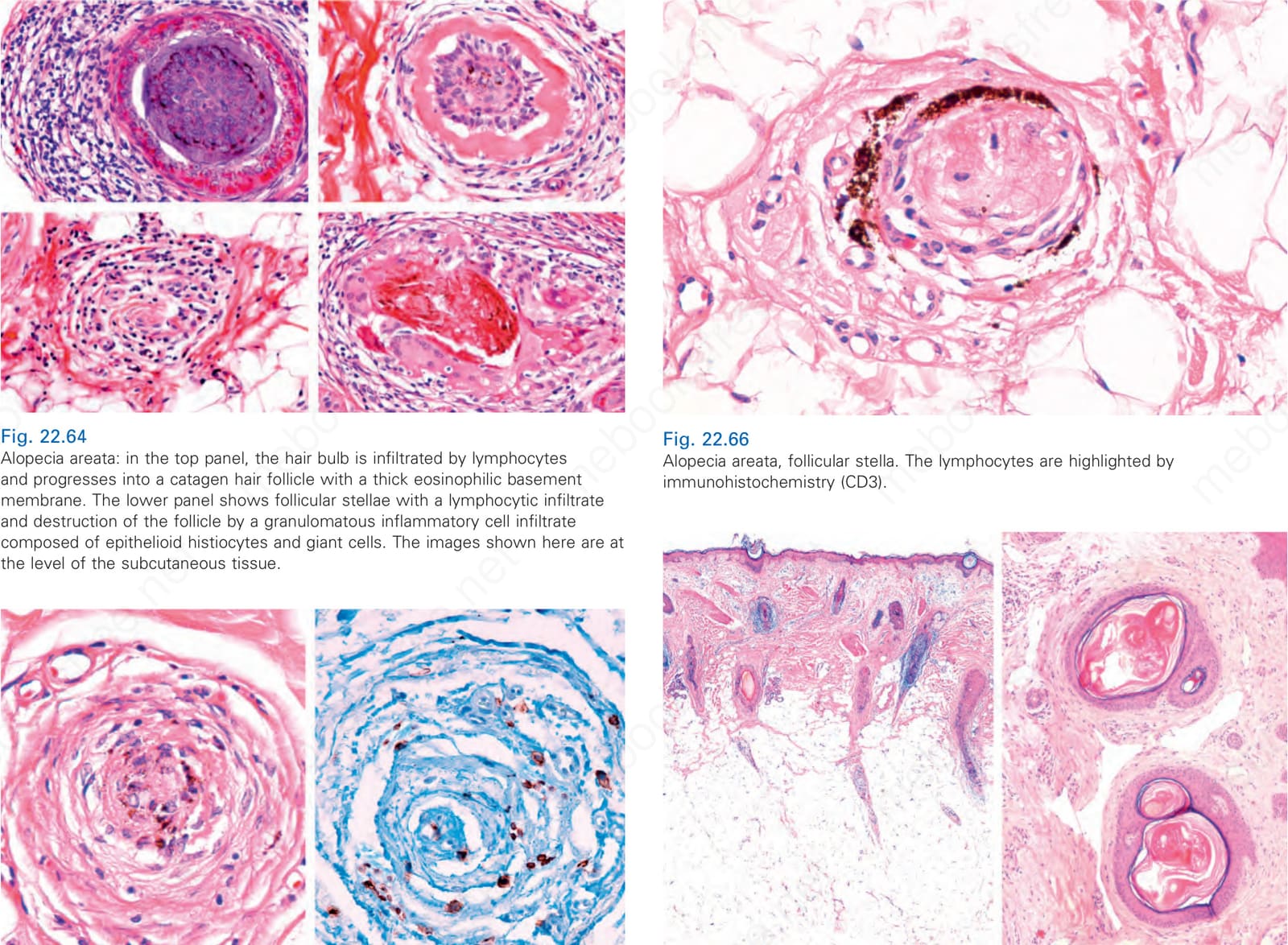
圖 22-64:圓禿 (alopecia areata):上方影像中,毛球被淋巴球浸潤並進展為具有厚嗜酸性基底膜的退化期毛囊。下方影像顯示帶有淋巴球浸潤的毛囊殘跡,以及由上皮樣組織球 (epithelioid histiocytes) 與巨細胞組成的肉芽腫性發炎細胞浸潤對毛囊的破壞。此處所示影像位於皮下組織層級。
Fig. 22.64 Alopecia areata: in the top panel, the hair bulb is infiltrated by lymphocytes and progresses into a catagen hair follicle with a thick eosinophilic basement membrane. The lower panel shows follicular stellae with a lymphocytic infiltrate and destruction of the follicle by a granulomatous inflammatory cell infiltrate composed of epithelioid histiocytes and giant cells. The images shown here are at the level of the subcutaneous tissue.
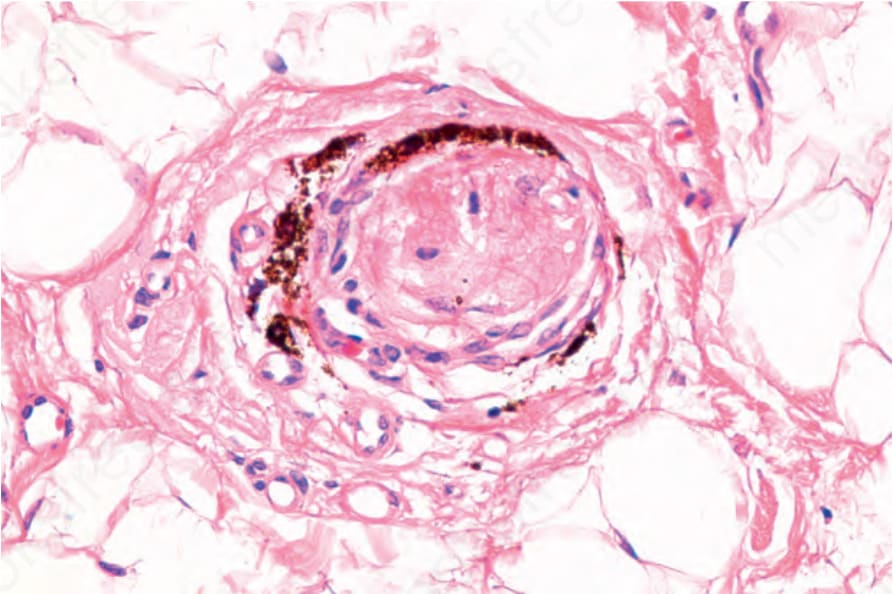
圖 22-66:圓禿 (alopecia areata),毛囊殘跡 (follicular stella)。淋巴球以免疫組織化學 (CD3) 標示。
Fig. 22.66 Alopecia areata, follicular stella. The lymphocytes are highlighted by immunohistochemistry (CD3).
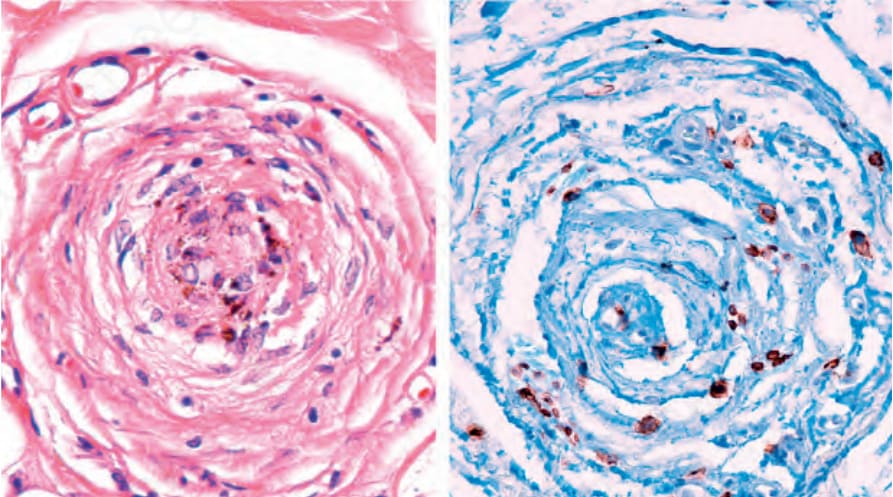
圖 22-67:圓禿 (alopecia areata),擴張漏斗部 (dilated infundibulae)。左側為垂直切片,右側為水平切片,因擴張的毛囊而顯示瑞士起司外觀 (swiss cheese appearance)。這些對應臨床所見的黃點。
Fig. 22.67 Alopecia areata, dilated infundibulae. On the left vertical sections and on the right horizontal sections showing a swiss cheese appearance due to dilated follicles. These correspond to the yellow dots seen clinically.
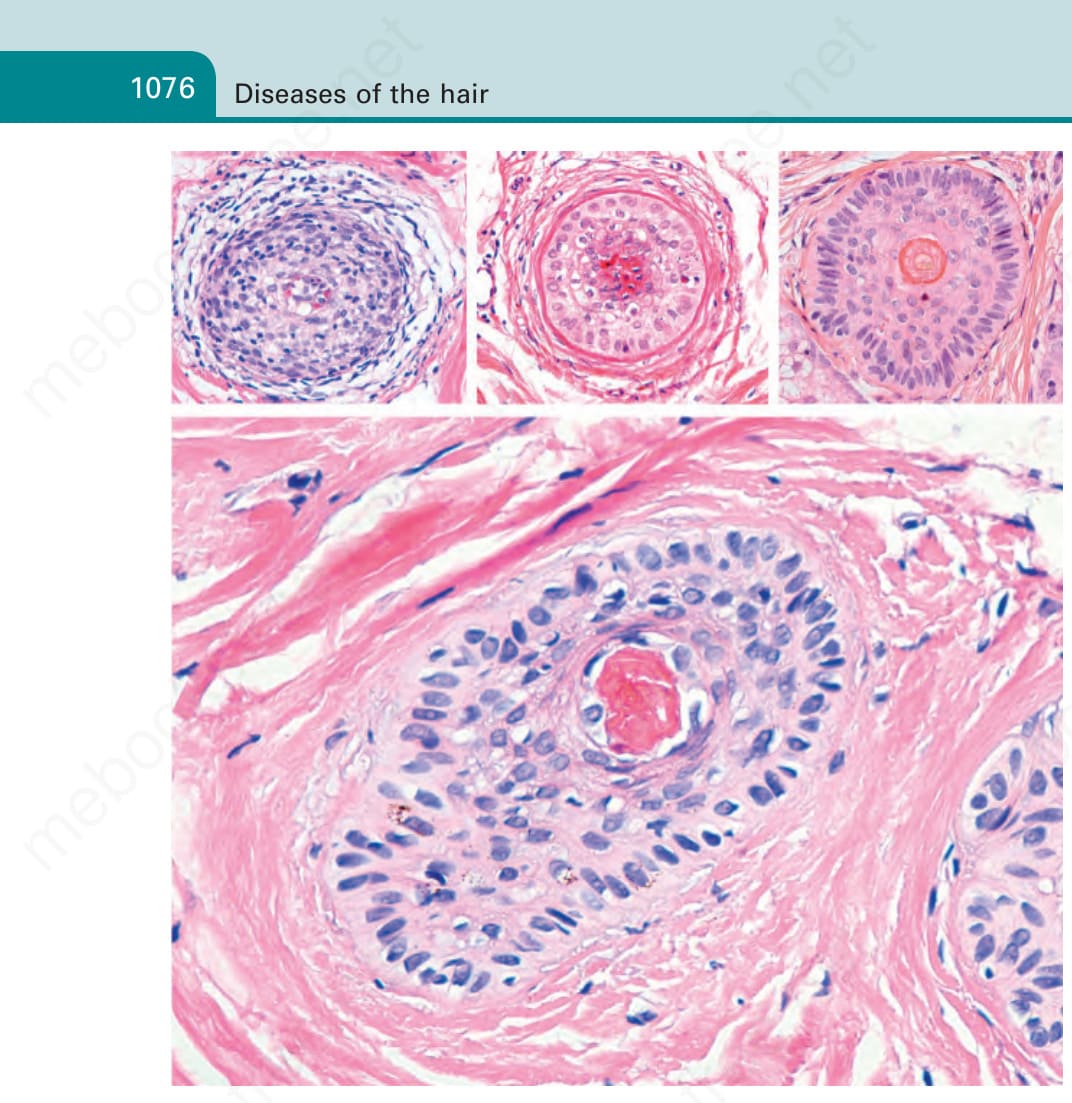
圖 22-68:圓禿 (alopecia areata),nanogen 毛:毛囊顯示上皮成分厚度減少,伴有內、外毛根鞘融合。在毛幹的位置上,注意無定形角質碎屑 (detritus of amorphous keratin)。中央與右上方影像顯示一處休止期毛囊,具有放射狀內毛根鞘 (radicular internal root sheath) 與畸形毛囊。
Fig. 22.68 Alopecia areata, nanogen hair: the hair follicle shows a decrease in the thickness of the epithelial component with fusion of the internal and external root sheaths. In place of a hair shaft, note detritus of amorphous keratin. The central and right top images display a follicle in telogen with a radicular internal root sheath and a malformed hair follicle.
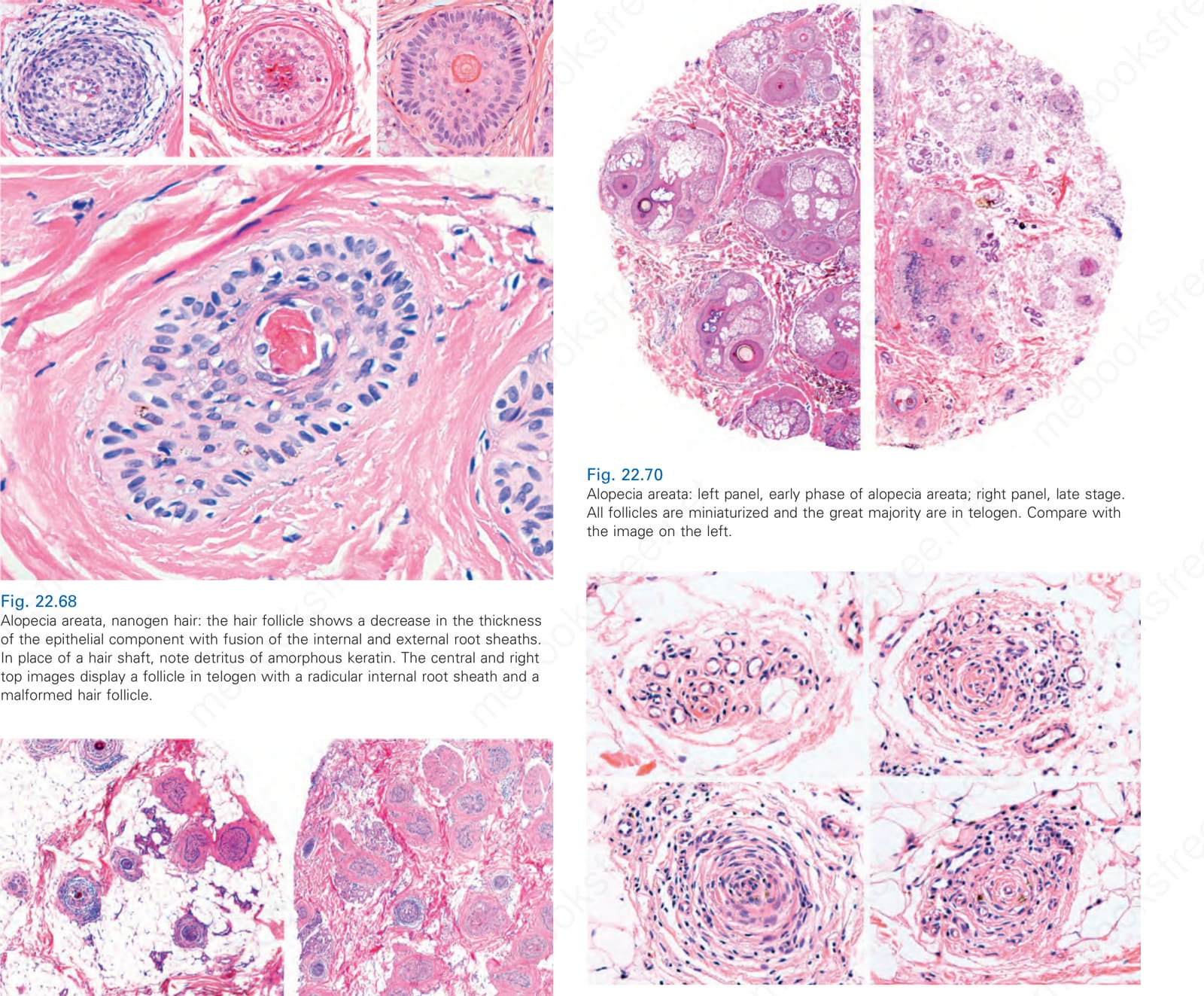
圖 22-69:(A, B) 圓禿 (alopecia areata),晚期階段:退化期/休止期毛囊顯著增加,並有稀疏的毛球周圍淋巴球浸潤伴隨殘跡 (stellae) 形成。
Fig. 22.69 (A, B) Alopecia areata, late stage: there is a remarkable increase in catagen/ telogen follicles, and a sparse peribulbar lymphocytic infiltrate with formation of stellae.
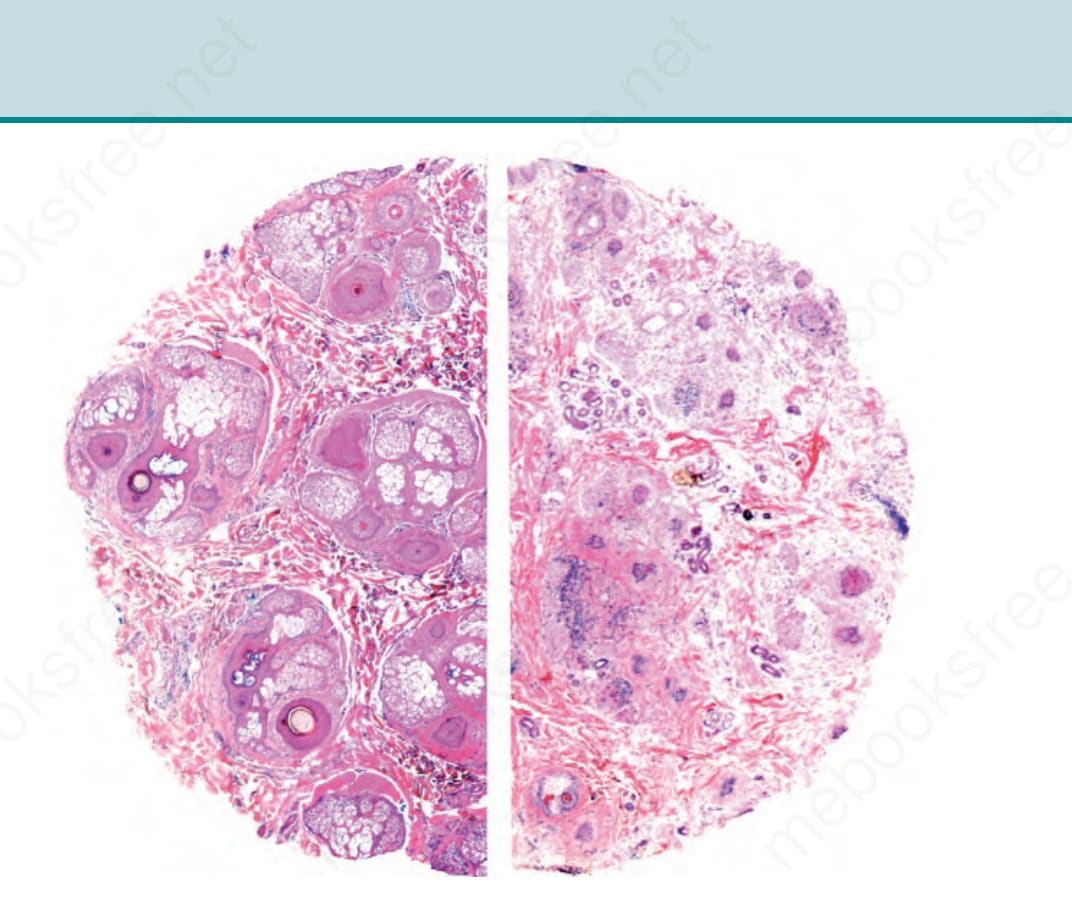
圖 22-70:圓禿 (alopecia areata):左側影像為 alopecia areata 早期;右側影像為晚期階段。所有毛囊均微小化,且絕大多數處於休止期。與左側影像比較。
Fig. 22.70 Alopecia areata: left panel, early phase of alopecia areata; right panel, late stage. All follicles are miniaturized and the great majority are in telogen. Compare with the image on the left.
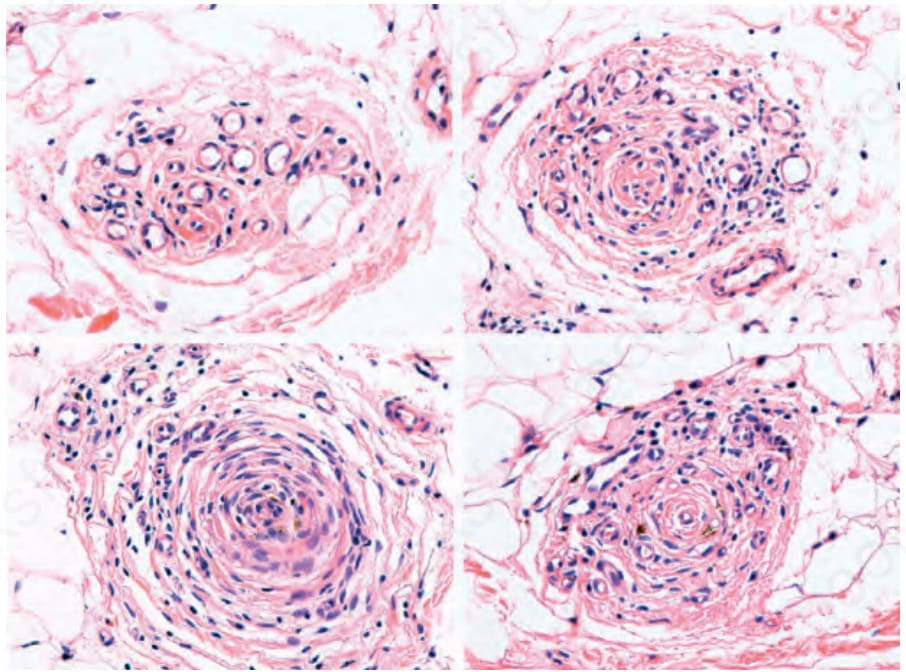
圖 22-71:圓禿 (alopecia areata):被淋巴球浸潤之毛囊殘跡 (follicular stellae) 的不同影像。
Fig. 22.71 Alopecia areata: different images of follicular stellae infiltrated by lymphocytes.
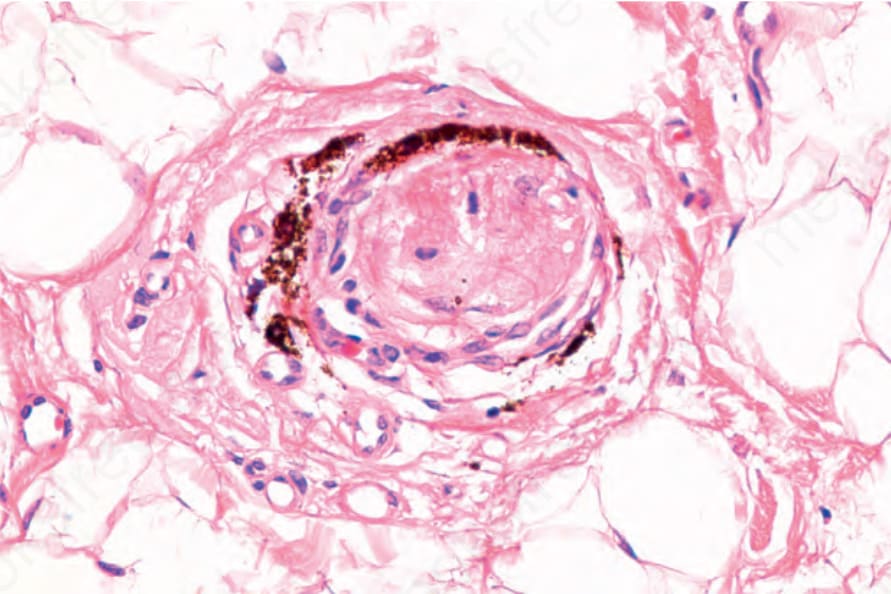
圖 22-65:(圖說烘焙於圖內)
Fig. 22-65 (caption embedded in image / 圖說烘焙於圖內)
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
乾癬 (psoriasis) 中導致皮脂腺萎縮與喪失的機轉尚不明。一種解釋可能是乾癬中分泌的眾多細胞激素 (cytokines) 中有部分負責對皮脂腺的損傷,或是因毛囊上段周圍的發炎而導致皮脂腺喪失。
瘢痕性禿髮與非瘢痕性乾癬性禿髮 (nonscarring psoriatic alopecia) 兩者的組織學變化,皆包括毛囊間表皮 (interfollicular epithelium) 的典型乾癬特徵,即:表皮的乾癬樣增生 (psoriasiform hyperplasia)、過度角化 (hyperkeratosis) 與角化不全 (parakeratosis) 伴顆粒層減少 (hypogranulosis),以及嗜中性球外滲至角化不全的區域。漏斗部變為擴張,退化期與休止期毛囊數量明顯增加,皮脂腺顯著萎縮並最終喪失,且毛囊上段與下段(包括毛球)有毛囊周圍淋巴球發炎細胞浸潤。可能有些許微小化。發炎可能導致肉芽腫性異物反應 (granulomatous foreign body reaction) 伴毛囊破壞。在較晚期,可觀察到毛囊周圍纖維化與伴有發炎的纖維束 (Fig. 22.73)。有時表淺表皮的變化與脂漏性皮膚炎 (seborrheic dermatitis) 所見極為相似 (Fig. 22.74)。與 tumor necrosis factor-alpha 抑制劑相關的乾癬性禿髮,組織學上與傳統乾癬性禿髮非常相似,但更為嚴重,且發炎細胞浸潤更顯著,包括漿細胞與嗜酸性球。
Alopecia areata incognita 可能特別難以與慢性休止期落髮 (chronic telogen effluvium) 區別,因為兩者皆有大量處於休止期的毛囊。然而,前者的皮膚鏡顯示有較多數量的黃點;此外,可能有較大的微小化傾向。近來,藉由免疫組織化學的使用,亦強調偵測高量的 UL16 結合蛋白-3 (UL16 binding protein-3, ULBP3) 作為診斷 alopecia areata incognita 的輔助。
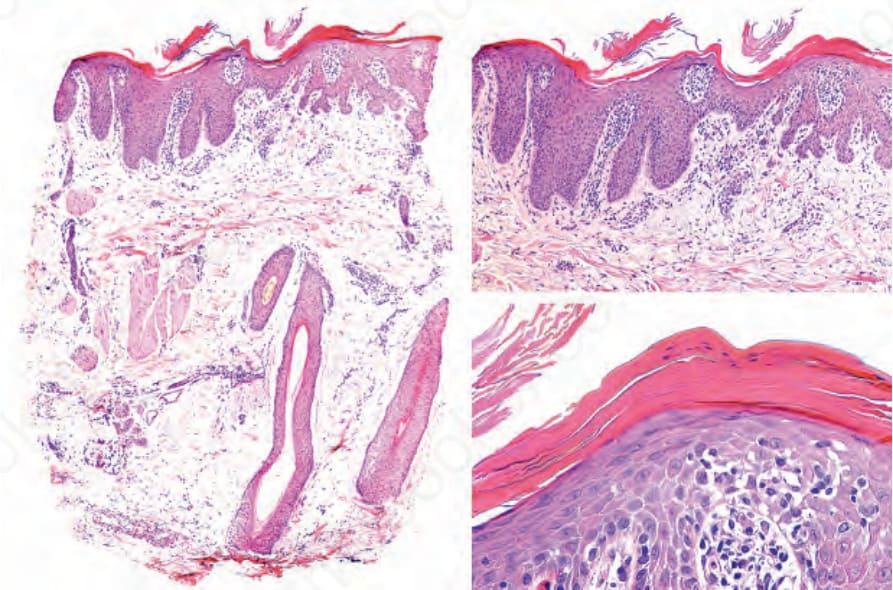
圖 22-73:乾癬 (psoriasis)。左側可明顯見到皮脂腺與毛囊單位的喪失。右側影像為表皮的乾癬性變化,包括表皮突 (rete ridges) 延長、過度角化、角化不全、顆粒層減少與角質層嗜中性球 (corneal neutrophils)。
Fig. 22.73 Psoriasis. On the left the loss of sebaceous glands and follicular units is evident. On the right panel epidermal psoriatic changes including elongation of the rete ridges, hyperkeratosis, parakeratosis, hypogranulosis and corneal neutrophils.
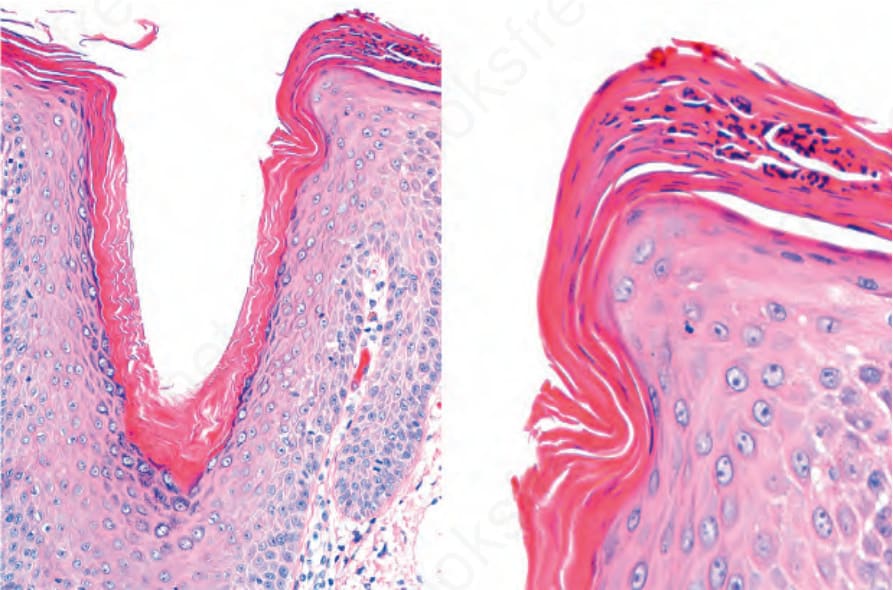
圖 22-74:頭皮乾癬 (psoriasis of the scalp),其變化類似脂漏性皮膚炎。有過度角化與角化不全伴嗜中性球聚集,在毛囊口緣 (lip of the follicular ostium) 更為顯著。
Fig. 22.74 Psoriasis of the scalp with changes simulating of seborrheic dermatitis. There is hyperkeratosis and parakeratosis with collections of neutrophils, more pronounced at the lip of the follicular ostium.
Discoid lupus erythematosus、lichen planopilaris 與 frontal fibrosing alopecia 在毛囊上段、隆突 (bulge) 周圍顯示較顯著的發炎,並導致瘢痕性禿髮 (scarring alopecia),伴有介面變化 (interface change) 與終端毛囊的永久性喪失。直接免疫螢光 (direct immunofluorescence) 對於確認前兩種情況的診斷很有用。同樣地,真皮黏液 (dermal mucin) 的存在是盤狀與全身性狼瘡的診斷線索。然而,重要的是要記住這兩種疾病實體可能並存。紅斑性狼瘡病人中 alopecia areata 的發生率甚至可達 10%。亦曾有狼瘡性脂膜炎 (lupus panniculitis) 臨床上類似 alopecia areata 的病例描述。在 pseudopélade 中,有廣泛的瘢痕化,伴有終端毛囊喪失,以及侷限於毛囊上段的輕度發炎細胞浸潤。Tinea capitis 亦在毛囊上段顯示發炎浸潤,含嗜中性球、淋巴球與組織球。真菌通常以 PAS 染色易於在毛幹周圍找到,並可於 Sabouraud 培養基中培養生長。乾癬性禿髮可藉由毛囊間表皮中乾癬的典型變化以及皮脂腺萎縮加以區別。重要的是要強調,有一種繼發於 antitumor necrosis factor-α 治療的乾癬性禿髮/alopecia areata 樣反應,同時具有 alopecia areata 與乾癬性禿髮的組織學變化,並伴有漿細胞與嗜酸性球的發炎細胞浸潤。
瀰漫性 alopecia areata 的鑑別診斷主要為休止期落髮 (telogen effluvium) 與雄性禿。臨床上,telogen effluvium 與雄性禿從不產生像 alopecia areata 最嚴重變異型(包括 alopecia totalis 與 alopecia universalis)所見的那般廣泛之落髮。在較不嚴重的病例中,組織學上,telogen effluvium 缺乏發炎,僅有休止期毛囊數量的增加。在雄性禿中,其組織學表現可能與慢性 areata alopecia 非常相似,因為前者毛髮的微小化可能非常廣泛。然而,缺乏淋巴球浸潤以及不同的臨床表現有助於鑑別診斷。