Alopecia areata
Alopecia areata
Clinical features Alopecia areata is quite common, affecting up to 1% of the population. The frequency of a family history is very high, ranging from 10% up to 42% of cases. It is more common in individuals between 15 and 40 years of age, and about 60% of cases occur before the age of 20.1 The disease is very rare in newborns and young children.2 Exceptionally, however, congenital cases may occur.3
Temporal triangular alopecia has been described in association with aplasia cutis, phakomatosis pigmentovascularis, Down syndrome, Klippel-Trénaunay syndrome, mental retardation and epilepsy, in a mother and daughter, leopard syndrome, and congenital heart disease with renal and genital abnormalities.9,10–16
Pathogenesis and histologic features The genetic basis of the disease is uncertain, but a paradominant trait has been suggested.14–17
The degree of involvement is very variable and can range from very mild disease where the hair loss is difficult to detect through to very severe cases with diffuse hair loss affecting the entire scalp or even the whole body (Fig. 22.54). Any hair-bearing surface may be affected. A typical patient presents with an abrupt development of patches of nonscarring alopecia in different patterns: circumscribed, bandlike in the temporo-occipital region (ophiasic), bandlike in the frontoparietal region in a ‘sisaipho’ pattern (ophiasis inversus) (Fig. 22.55),4 and reticular. When the patches extend and become confluent, involving the entire scalp, the appearance is known as alopecia totalis (Fig. 22.56). If there is hair loss on the entire body, the condition is referred to as alopecia universalis.5,6, Even in the most severe forms of alopecia totalis and universalis, one can observe isolated small groups of unaffected hair follicles. Alopecia areata may occasionally present with a pattern mimicking acute telogen effluvium, a positive pull test, and trichodynia (alopecia areata incognita).7 The proportion of patients who eventually develop alopecia totalis and universalis varies but is around 7%.8 Alopecia totalis is more frequent in children.9
The diagnosis of temporal triangular alopecia is generally based on clinical features. A biopsy is only taken when the diagnosis is in doubt. Horizontal sections may be performed, paying particular attention to the most superficial sections at the level of the infundibulum.
The epidermis and dermis are normal, but there are almost no terminal hairs and the number of vellus hairs is increased. The sebaceous and eccrine glands are normal. Fibrous stellae and inflammation are absent (Fig. 22.53). In general, the histologic appearance is very similar to that of a normal skin biopsy.18
Differential diagnosis The differential diagnosis includes other causes of circumscribed nonscarring alopecia, particularly alopecia areata, tinea capitis, and trichotillomania. In the former, the bulbs of anagen follicles are surrounded and infiltrated by lymphocytes and there are terminal and miniaturized hair follicles cycling to catagen and telogen. In tinea capitis, the demonstration of fungal organisms
Examination of the involved scalp generally reveals that except for the absence of hair, the skin appears normal, follicular openings are preserved, and there is no evidence of scarring (Fig. 22.57). In occasional cases, however, edema and erythema are observed.
Hair color may appear normal or it may show mild lightening and loss of sheen. In the periphery of the patches of alopecia, one typically finds exclamation mark hairs, which are short and become thinner as they gradually approach the scalp. They are a very characteristic feature but may also be seen in trichotillomania.10 Sometimes, the damage to the hair follicles in
1071 Nonscarring alopecias
A
A
B
anagen is so intense that the hairs break as soon as they emerge from the scalp. A dermoscopy finding consist of yellow dots, found in 95% of cases of the disease.11 The process usually affects pigmented hairs. Nonpigmented hairs appear to be more resistant, at least temporarily. This phenomenon of selective black hair loss where the gray hair is spared may give the impression of speedy graying (Marie Antoinette syndrome).12 When the hair grows back, it is often white or light brown and slowly recovers its normal color. Exceptionally, persistent white hair is a feature.
B
Alopecia areata sparing a congenital nevus of the eyebrow and a nevus flammeus has been called Renbök phenomenon (inverse Koebner phenomenon) and interpreted as a localized form of genetic resistance.13,14
Nail changes may be present in patients with alopecia areata and include pitting, spotted lunula, and red lunula. Changes may be seen in one, several, or all of the nails (Fig. 22.58). Trachyonychia (twenty-nail dystrophy) occurs in up to 3% of patients.15–19 The dystrophy may precede, coincide with, or occur after resolution of the episode of alopecia.20
Alopecia areata has been associated with many other diseases. Some of these have an autoimmune etiology such as Hashimoto thyroiditis, type I (insulin-dependent) diabetes, Addison disease, vitiligo, hereditary thrombocytopenia (pseudo-von Willebrand disease), myasthenia gravis, polymorphism in the interleukin (IL)-1 receptor antagonist gene, lupus erythematosus, autoimmune polyendocrinopathy-candidiasis-ectodermal dysplasia syndrome (autoimmune polyglandular syndrome-1), common
variable immunodeficiency, relapsing polychondritis, kidney-pancreas transplant recipients taking ciclosporine and after allogeneic bone marrow transplantation.21–35 Other associations include lichen planus, atopy, human immunodeficiency virus (HIV) infection, twenty-nail dystrophy, Down syndrome, cytomegalovirus and Epstein-Barr virus infection, celiac disease in children, chemotherapy, interferon-alpha (IFN-α), ribavirin, ciclosporine A, rifampicin, borderline tuberculoid leprosy, and ocular alterations (keratoconus, symptomless punctate lens opacities).22,36–48 It has also been observed in Clozapine-induced hypereosinophilia, narcolepsy type 1, and as recurrent disease after vaccination.49–51 Several biological agents such as etanercept, infliximab, and adalimumab are associated with the appearance or worsening of the illness.52–54 It has also developed in a patient with pili annulati.55 Patients with severe alopecia areata appear to have an increased incidence of nuchal nevus flammeus.56
1072 Diseases of the hair
Pathogenesis and histologic features Experimental studies have shown that alopecia areata is basically an organ-specific autoimmune disease thought to result from a collapse of hair follicle immune privilege, driven by cellular immunity with autoantibody production representing a secondary phenomenon.60–62 Autoantibodies to a diverse range of antigens including smooth muscle cells, gastric parietal cells, thyroid cells, and components of anagen hair follicles have been described.62–65
It is unknown whether induction of the disease results from exposure to exogenous or endogenous antigens and whether it represents a consequence of an immune reaction to normal or aberrant epitopes. However, research suggests that the pathogenesis involves at least four events:
• failure of the anagen hair follicle to maintain its privileged immunity (the inner root sheath and hair matrix do not express, or express very low level of, major histocompatibility complex class Ia antigens and maintains an active NK cell suppression) resulting in exposure of epitopes, which initiate an immune response,66,67
• antigen presentation, activation, and response of the lymphocyte to antigen-presenting cells,
• migration of activated inflammatory cells and infiltration of hair follicles,
• damage to the hair follicle by the inflammatory cell infiltrate.68
It has been proposed that neurotrophins play a role in the pathogenesis of the disease. Since neurotrophins and their receptors are differentially expressed in subsets of immune cells in alopecia areata, a role for these proteins in the pathogenesis appears likely.69
The increased frequency of alopecia areata in genetically related individuals suggests that there is a genetic link to the disease. Among the general population the condition does not display a mendelian pattern of expression since the resulting phenotype demonstrates variable degrees of hair loss. It has been proposed that expression of alopecia areata involves a complex interaction of multiple genes, in which major genes control susceptibility to the disease while other minor ones modify the phenotype.70
Prognosis in alopecia areata is variable and not very predictable in the individual patient.57 Nevertheless, it has been observed that the prognosis tends to be good in patients who have experienced hair growth with long-lasting remissions between episodes. Spontaneous remission can be expected in 34–50% of patients within 1 year, although almost all will experience more than one episode of the disease.58 Contrariwise, those who have had persistent hair loss or brief or incomplete remissions have a poor prognosis. The severity of alopecia areata at the time of first consultation and response to therapy is an important prognostic factor.59 The outlook is particularly poor in those patients with onset of the disease before puberty, those with a family history of the disease (present in 25% of cases), and those with alopecia totalis and alopecia universalis.7 Atopic patients appear to suffer a more severe form of alopecia areata.
Many illnesses with an autoimmune basis have been associated with specific human leukocytic antigens (HLA). Alopecia areata has been studied in association with both HLA class I and class II. The most relevant associations have been found with the HLA class II antigens (HLA-DR, -DQ, -DP). The molecular basis of this genetic association is supported by the fact that HLA binds and presents peptides derived from self and foreign protein antigens to the immune system for recognition and activation. More than 80% of all cases evaluated in one study were positive for the antigen DQB1*03 (DQ3), suggesting that this antigen is a marker for susceptibility. Furthermore, in patients with alopecia totalis and universalis, the frequency of the
antigens DRB10401 and DBQ10301 (DR4 and DQ7) is significantly increased.71–73 HLA-DR5 has been linked to the early-onset and severe form of alopecia areata. Other HLA genes associated are NOTCH4 and MICA. Non-HLA genes associated with the disease are PTPN22 and AIRE.74
In the last genome study supported by the genetic database of the national registry of alopecia areata in the United States, 139 nucleotides with polymorphism and significantly associated with alopecia areata were identified.64 There were eight different associated regions. One of such regions corresponds to the already well-known HLA complex. Seven loci genomes were also found. Five of them are expressed in the immunological system and two of them in the hair follicle. Interestingly, these genes were more related to illnesses such as diabetes type I, multiple sclerosis, rheumatoid arthritis, and celiac disease, rather than to psoriasis and vitiligo diseases to which they were initially thought to be associated.75–77 These diseases present a unifying mechanism known as ULBP3, which is the enhancement of the regulation of the danger signal in the target organ. Under normal circumstances, ULBP3 is not found in hair follicles, but in the affected hair follicles of alopecia areata it is prominent. These proteins attract the killer cells marked by the receptor NKG2D.78

Fig. 22.54 (A, B) Alopecia areata: typical annular noninflammatory areas of alopecia. Courtesy of L.M. Gómez, MD, UPB, Colombia.

Fig. 22.55 Alopecia areata: (A) this broad band of alopecia in the occipital region is known as ophiasis. (B) A similar pattern in the frontoparietal region it is known as ophiasis inversus, or a ‘sisaipho’ pattern. Courtesy of the Institute of Dermatology, London, UK.
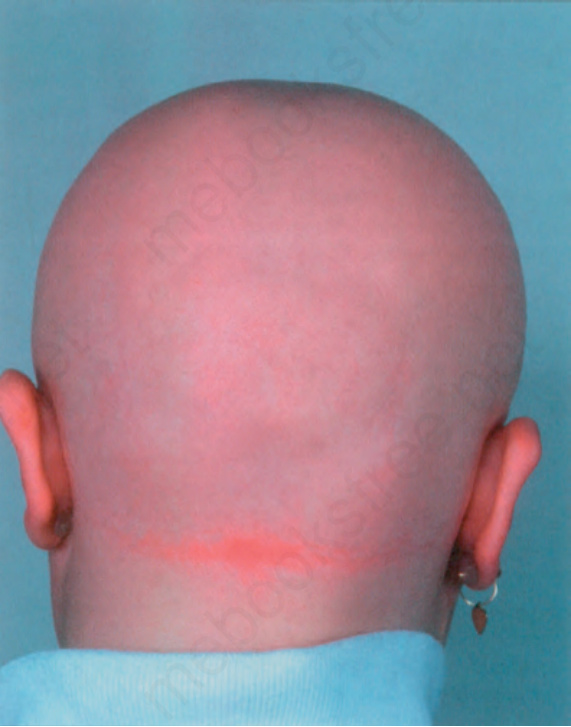
Fig. 22.56 Alopecia areata totalis: in this patient, there is complete loss of scalp hair. Courtesy of the Institute of Dermatology, London, UK.
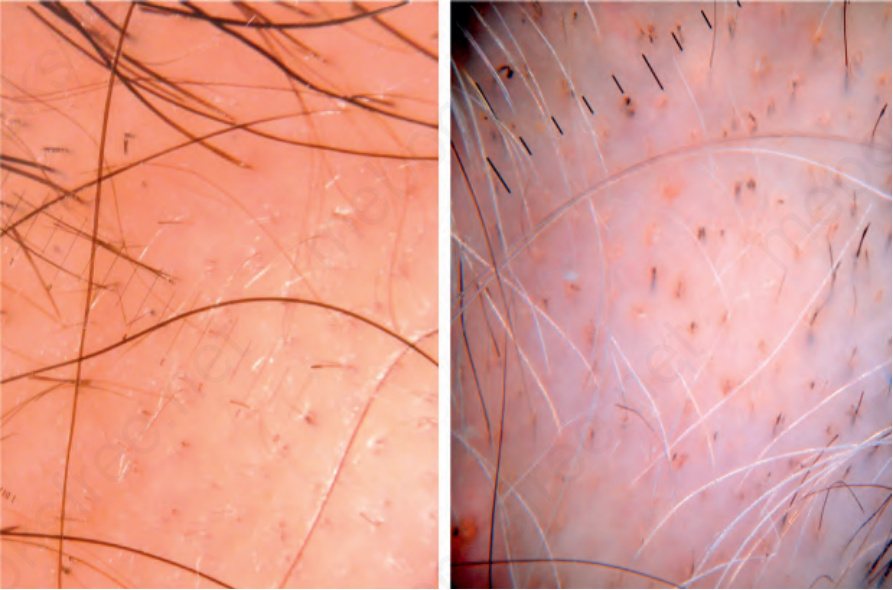
Fig. 22.57 Alopecia areata dermoscopy: note that the follicular density is normal and the opening of the follicles have not been lost. There are some miniaturized hair follicles and an exclamation mark hair. On the right panel, yellow dots are observed. The gray hairs have persisted despite the loss of the pigmented hair. There are also some exclamation mark hairs. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.

Fig. 22.58 Alopecia areata: in this patient, there is severe involvement of the nails (trachyonychia). Courtesy of P. Reygagne, MD, Centre Sabouraud, Paris, France.
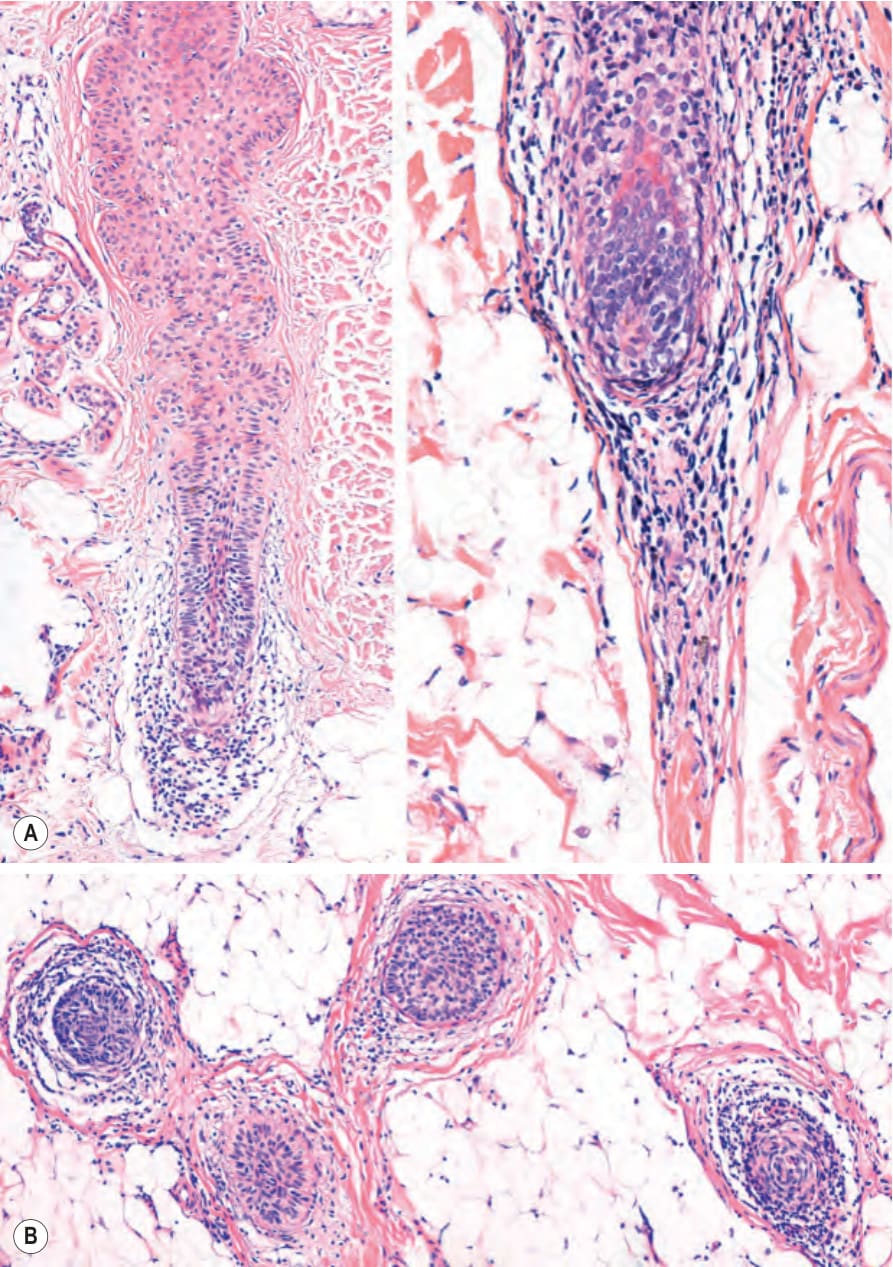
Fig. 22.62 Alopecia areata: hair follicle in involution. (A) Vertical section. In the follicle on the right there is a hair bulb lymphocytic infiltrate which also involves the follicular stella. (B) Horizontal section. Hair follicles in the subcutaneous tissue with a lymphocyte infiltrate of variable intensity.

Fig. 22-53 (caption embedded in image / 圖說烘焙於圖內)
1073 Nonscarring alopecias
It is important to remember that the histopathological features depend on the stage of the disease.82
The best site to take biopsies from is the periphery of an active lesion. The extraction (hair-pull tests) and dermoscopy are useful when it comes to selecting the most active areas as one can observe exclamation point hairs, yellow dots, or black dots.81
All the changes in alopecia areata described in vertical sections are better observed in horizontal sections (Fig. 22.59).83 This is particularly true of hair bulb lymphocytic infiltration. Nevertheless, the inflammatory infiltrate is not always visible. The frequency with which this and other histologic changes are observed depends on the stage of the illness when the biopsy is performed.
The effect of stress on the pathogenesis is unclear and controversial, although it has been suggested that it can trigger the disease. It has been observed that substance P and nerve growth factor could be acting as key mediators of stress-induced hair growth-inhibitory effects, through keratinocyte apoptosis, inhibition of hair follicle proliferation, and catagen induction.79,80
Early stages In the early stages of the disease, the peribulbar inflammatory infiltrate is intense (Fig. 22.60). However, the infiltrate gradually decreases and there
Laboratory tests are not usually necessary for the diagnosis, but they may be of value in detecting associated conditions, particularly autoimmune disease. The hair-pull and hair-pluck tests show an increase in the number of telogen and dystrophic anagen hairs. The remaining anagen hairs are dystrophic because the continuous inflammatory process results in premature transformation into catagen and telogen phase. This abbreviated growth cycle results in many terminal follicles with poorly keratinized short stems that break readily (exclamation mark hairs).81
Histologically, alopecia areata is characterized by four basic features:
• normal numbers of follicular units and hair follicles in the initial stages with loss of follicles in the recalcitrant and most chronic phases,
• an increase in the number of catagen and telogen hair follicles,
• a lymphocytic infiltrate of variable severity affecting the bulbs of the anagen hair follicles and the catagen and telogen follicular stellae,
• a tendency for hair follicles to become miniaturized in the more chronic and recalcitrants forms of the disease.
A
B
1074 Diseases of the hair
is an increase in the number of catagen and telogen hair follicles. Telogen counts may exceed those seen in telogen effluvium (Fig. 22.61). The follicles show a variable inflammatory lymphocytic infiltrate in the peribulbar region (Figs 22.60 and 22.62). This may occasionally be very mild, even in more active lesions. The latter feature is particularly noticeable in the atypical, incognita, and ophiasic forms of the disease (Fig. 22.63). The presence of eosinophils in the stellae and within the hair bulbs has been described as an early and typical feature.84 The earliest follicular changes consist of loss of structural integrity of the centrally located supramatrical upper bulbar region and shrinkage of hair bulbs.85 The hair matrix is infiltrated by lymphocytes, and there is also pigment incontinence, matrix cell necrosis, and vacuolar damage. The inflammatory infiltrate is especially prominent in terminal hair follicles, the bulbs of which are located in the subcutaneous tissue (Fig. 22.64). Pigment incontinence may be very conspicuous and lead to the formation of clumps of melanin pigment (pigment casts) in the distorted hair bulb and follicular streamer (Fig. 22.65).86 The infiltrate is composed of an admixture of CD4+ and CD8+ T lymphocytes (Fig. 22.66).87
A
In the upper part of the hair follicle within the epidermis, one can observe dilated infundibulae filled with keratin which correspond to the yellow dots seen clinically (Fig. 22.67 and see Fig. 22.57). Those in horizontal sections could display a swiss cheese pattern.88
Immunofluorescence studies have shown deposits of C3, IgG, and IgM along the basement membrane of the inferior part of the hair follicle.89 Once the follicle enters catagen stage and progresses to telogen, the inflammatory cell infiltrate decreases.90
Follicular lymphocytic infiltration is accompanied by progression to catagen and telogen. After this, the hair follicle rapidly returns to anagen and the cycle starts again. Because of this continuous cycle and the accompanying inflammatory process, the follicles go through two important morphological changes:
• trichomalacia characterized by short, incompletely keratined (pencil-point) hairs which are susceptible to trauma,
• miniaturization of some anagen follicles.
B
Late stage In the late stage of the disease, the inflammation decreases and numerous miniaturized hair follicles and telogen follicles are present. The number of miniaturized follicles increases with chronicity, and these may simulate hair follicles in late anagen stage. Such hairs are found in the middle or upper dermis and have been described as nanogen. They represent an intermediate stage between vellus and terminal anagen hair follicles. In horizontal sections there is generally no hair shaft production, although occasionally a very thin incompletely keratinized form is produced, correlating with the empty infundibula observed on the scalp. In vertical sections the proximal
1075 Nonscarring alopecias
end of the hair shaft acquires a ragged appearance instead of the normal club shape. These hair follicles can sometimes display histologic features of the anagen, catagen, and telogen phases simultaneously with evidence of growth and involution in the form of mitotic activity and apoptosis (Fig. 22.68).
nail fold, nail matrix, nail bed, and hyponychium.18 Rarely, the histology is indistinguishable from lichen planus.
Differential diagnosis The differential diagnosis of alopecia areata varies depending on whether the clinical pattern of hair loss is localized or diffuse.
In longstanding alopecia areata, the majority of the hair follicles are in catagen and telogen. Since the inflammatory infiltrate does not affect hair follicles in these growth phases, inflammation may be absent in the subcutaneous tissue (Fig. 22.69).82,91
Inactive alopecia areata can resemble androgenetic alopecia with many miniaturized hair follicles (Fig. 22.70).
Numerous stellae are present in the deep dermis and the subcutaneous tissue, and these may be accompanied by an inflammatory cell infiltrate and melanin pigment (Fig. 22.71). In some cases, there may be destruction of the hair follicle by the inflammatory cell infiltrate and this is associated with histiocytes and giant cells (see Fig. 22.64).
In patients presenting with trachyonychia, a nail biopsy usually shows a lymphocytic infiltrate with exocytosis and spongiosis involving the proximal
In cases with localized areas of hair loss, the differential diagnosis includes trichotillomania, triangular temporal alopecia, syphilis, discoid lupus erythematosus, lichen planopilaris, frontal fibrosing alopecia, pseudopélade, tinea capitis, and psoriatic alopecia.
Trichotillomania may closely simulate alopecia areata but microscopic examination in the former condition shows more pigmented casts, an absence of miniaturized hairs, and minimal inflammatory infiltrate. Triangular temporal alopecia shows no clinical or histologic evidence of inflammation and there is no excess of hair follicles in telogen or catagen. Alopecia syphilitica may be very similar but clinically the plaques rarely show complete absence of hairs. Histologic examination can also be problematical since both conditions show a peribulbar inflammatory cell infiltrate. Eosinophils are not frequent in syphilis but plasma cells tend to be prominent. Serology is often essential in difficult cases.
1076 Diseases of the hair
B A
Discoid lupus erythematosus, lichen planopilaris, and frontal fibrosing alopecia display more prominent inflammation in the upper segment of the follicle, around the bulge, and result in scarring alopecia with interface change and permanent loss of terminal hair follicles.92 Direct immunofluorescence is useful to confirm the diagnosis in the first two conditions. Equally, the presence of dermal mucin is a diagnostic clue in discoid and systemic lupus. It is important however, to keep in mind that both entities
may coexist. The incidence of alopecia areata in patients with lupus erythematosus may even reach 10%.93 Cases of lupus panniculitis clinically simulating alopecia areata have also been described.94 In pseudopélade, there is extensive scarring, with loss of terminal hair follicles and a mild inflammatory cell infiltrate localized to the upper segment of the follicle. Tinea capitis also shows an inflammatory infiltrate in the upper segment of the hair follicle with neutrophils, lymphocytes, and histiocytes. The fungi are usually easily found in association to the hair shaft with a PAS stain and may be grown in Sabouraud agar. Psoriatic alopecia may be distinguished by the presence of typical changes of psoriasis in the interfollicular epidermis and the atrophy of the sebaceous glands. It is important to highlight that there is a type of psoriatic alopecia/alopecia areata-like reaction secondary to antitumor necrosis factor-α therapy with simultaneous histologic changes of alopecia areata and psoriatic alopecia associated with an inflammatory cell infiltrate of plasma cells and eosinophils. 95,96
The differential diagnosis of diffuse alopecia areata is mainly telogen effluvium and androgenetic alopecia. Clinically, telogen effluvium and androgenetic alopecia never produce such extensive hair loss as that seen in the most severe variants of alopecia areata including alopecia totalis and alopecia universalis. In the less severe cases, histologically, telogen effluvium lacks inflammation and there is only an increase in the number of telogen hair follicles. In androgenetic alopecia, the histologic presentation may be very similar to that of chronic areata alopecia as in the former the miniaturization of hairs may be very extensive. However, the lack of lymphocytic infiltration and the different clinical picture are aids in the differential diagnosis.
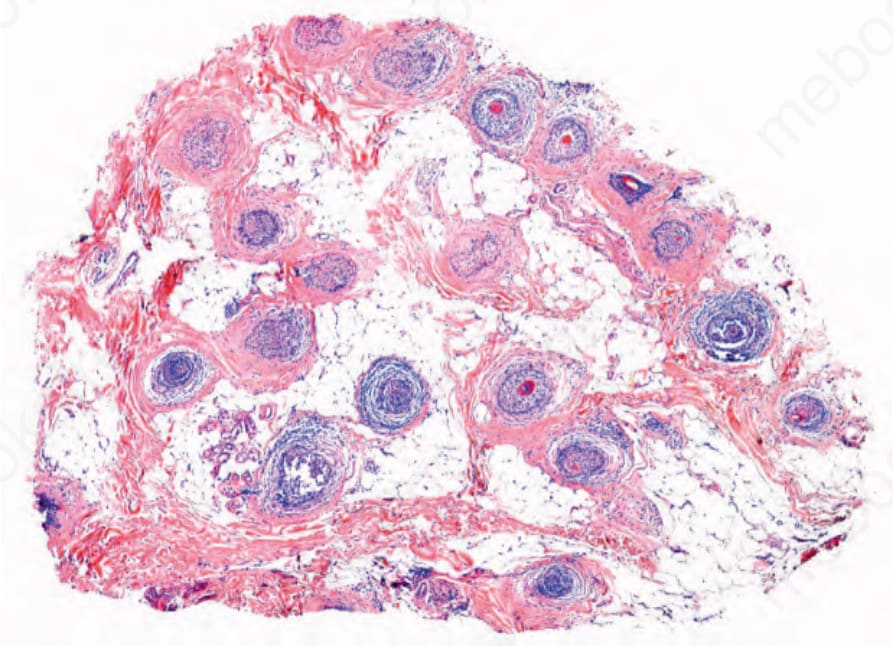
Fig. 22.59 Alopecia areata: Horizontal section displays a near normal density of hair follicles; some of the follicles on the left upper side are in catagen and telogen. Courtesy of J.C. Perez, MD, HPTU, Medellín, Colombia.
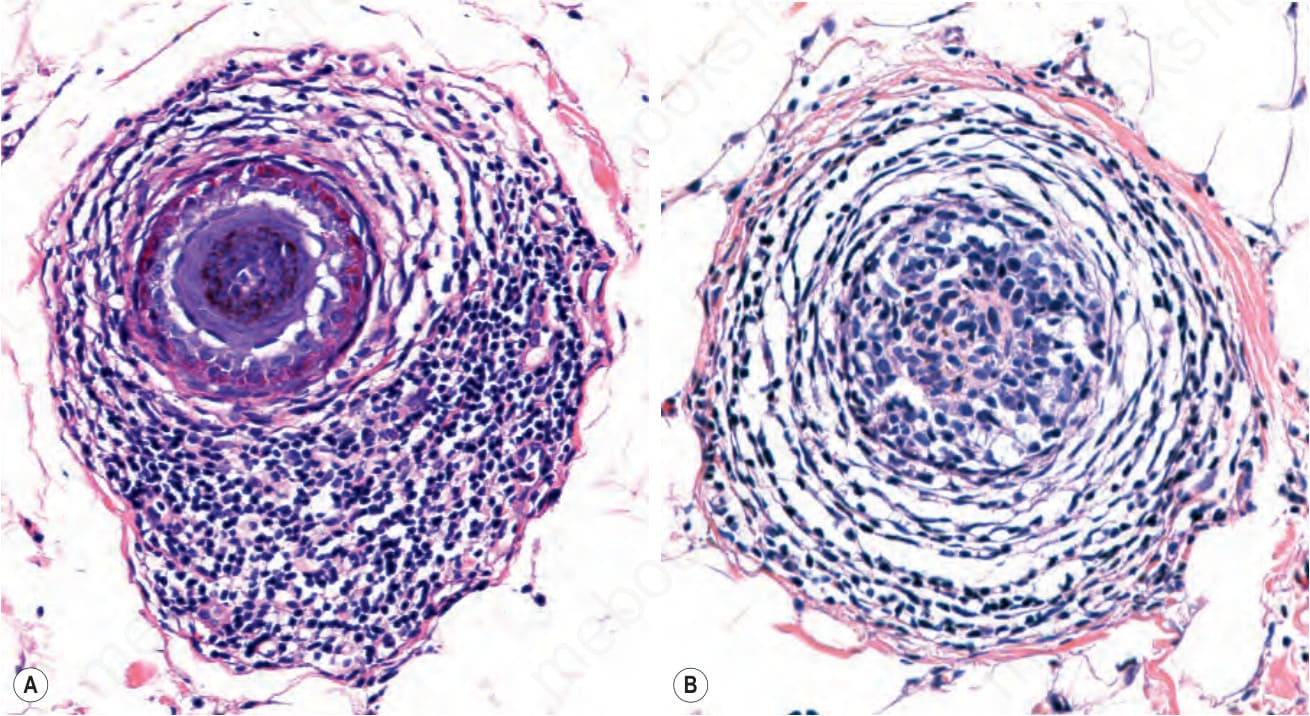
Fig. 22.60 (A, B) Alopecia areata: high-power view of the peribulbar lymphocytic infiltrate, which is sometimes referred to as ‘swarm of bees’. Note (from left to right) that as the pili bulb disappears the inflammatory infiltrate becomes less dense.
Fig. 22.61 Alopecia areata: vertical and horizontal sections of catagen-telogen hair bulbs. The inflammatory infiltrate is still present in the telogen remnants.
Fig. 22.63 Alopecia areata incognita: follicles in telogen. The hair follicle on the right displays features of a follicle in nanogen. There is a lymphocytic infiltrate associated with eosinophils and masts cells.
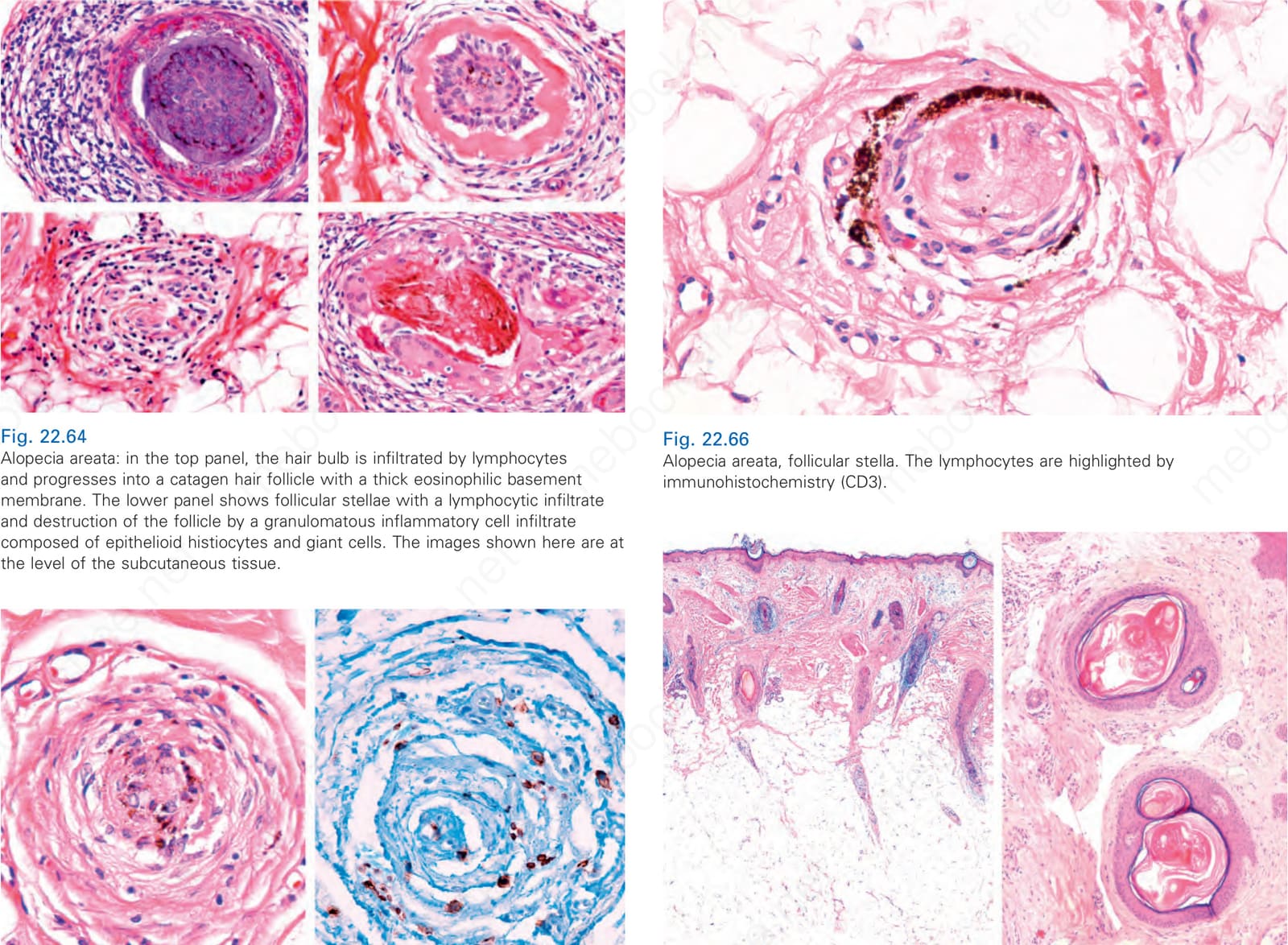
Fig. 22.64 Alopecia areata: in the top panel, the hair bulb is infiltrated by lymphocytes and progresses into a catagen hair follicle with a thick eosinophilic basement membrane. The lower panel shows follicular stellae with a lymphocytic infiltrate and destruction of the follicle by a granulomatous inflammatory cell infiltrate composed of epithelioid histiocytes and giant cells. The images shown here are at the level of the subcutaneous tissue.
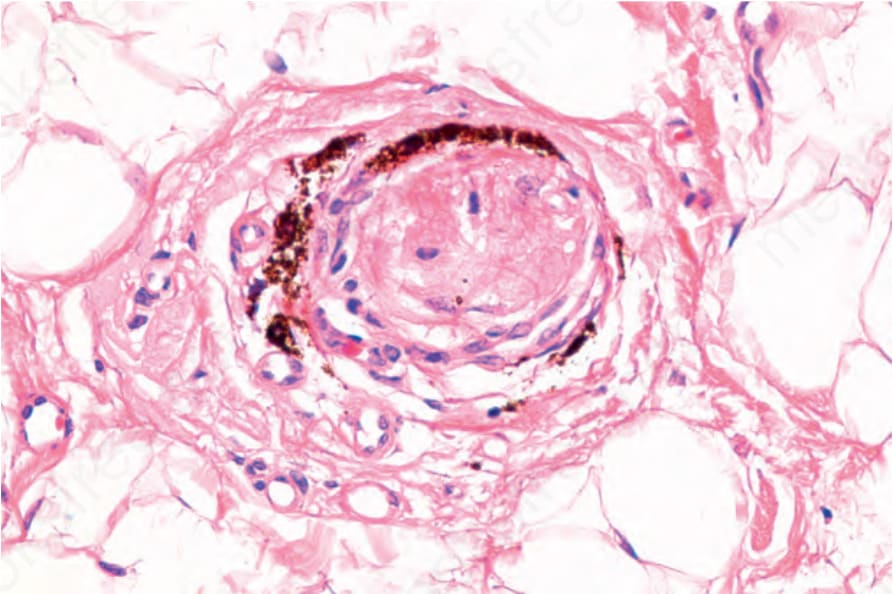
Fig. 22.66 Alopecia areata, follicular stella. The lymphocytes are highlighted by immunohistochemistry (CD3).
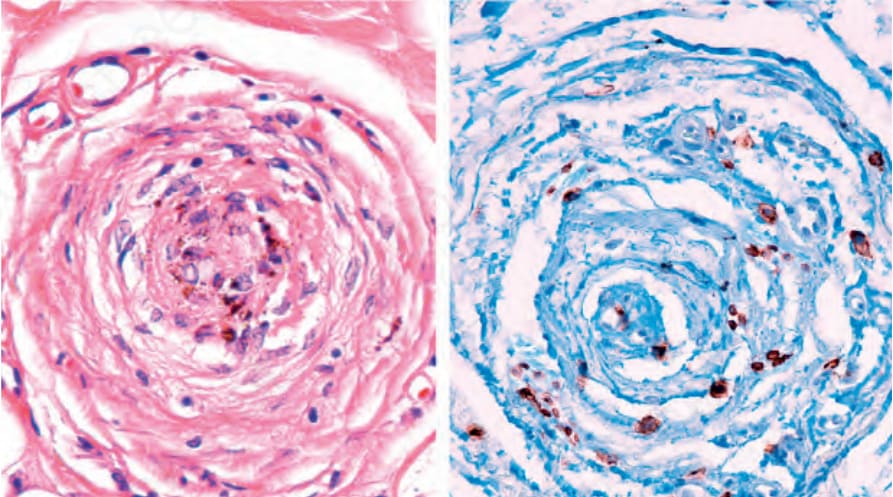
Fig. 22.67 Alopecia areata, dilated infundibulae. On the left vertical sections and on the right horizontal sections showing a swiss cheese appearance due to dilated follicles. These correspond to the yellow dots seen clinically.
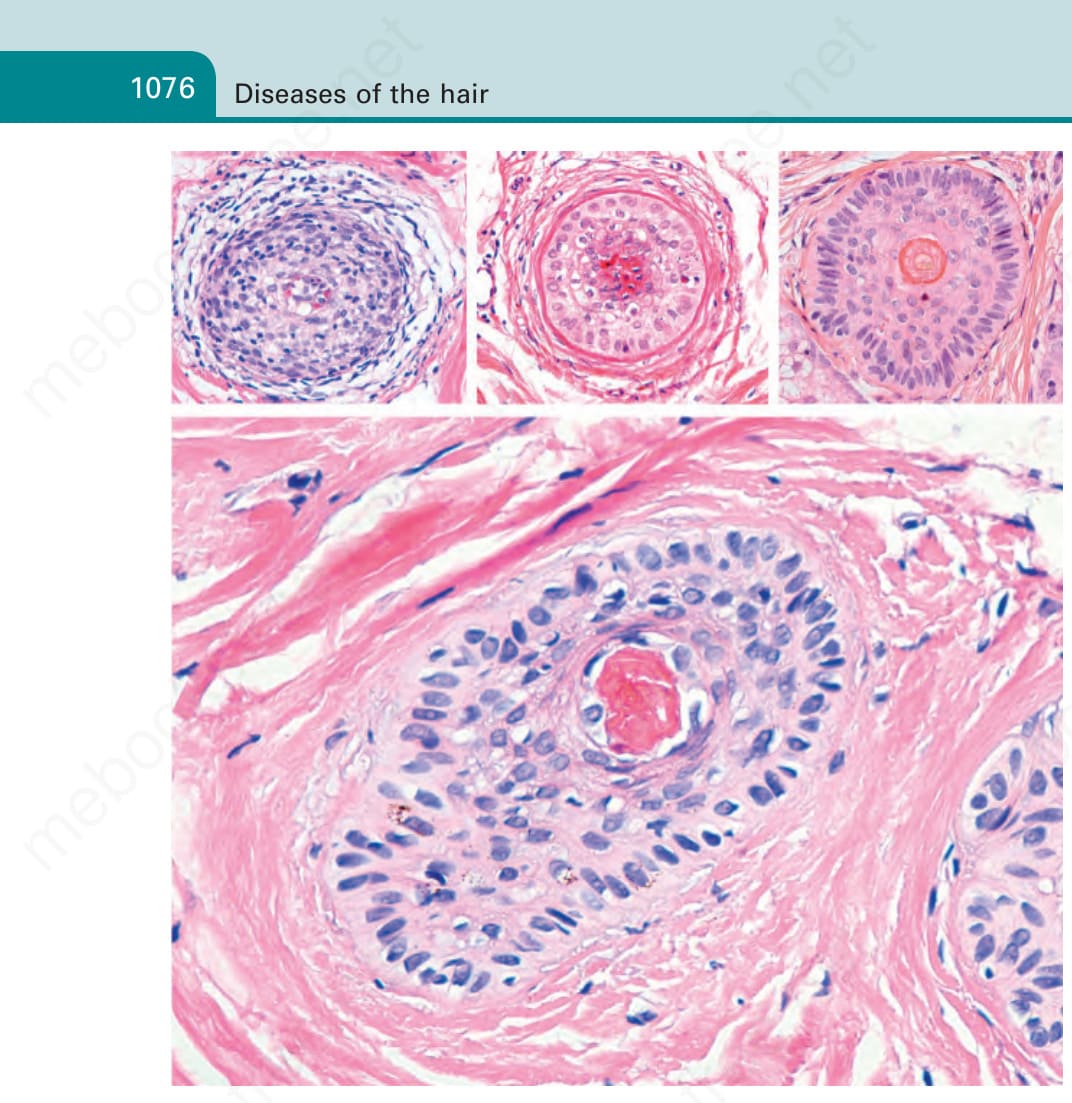
Fig. 22.68 Alopecia areata, nanogen hair: the hair follicle shows a decrease in the thickness of the epithelial component with fusion of the internal and external root sheaths. In place of a hair shaft, note detritus of amorphous keratin. The central and right top images display a follicle in telogen with a radicular internal root sheath and a malformed hair follicle.
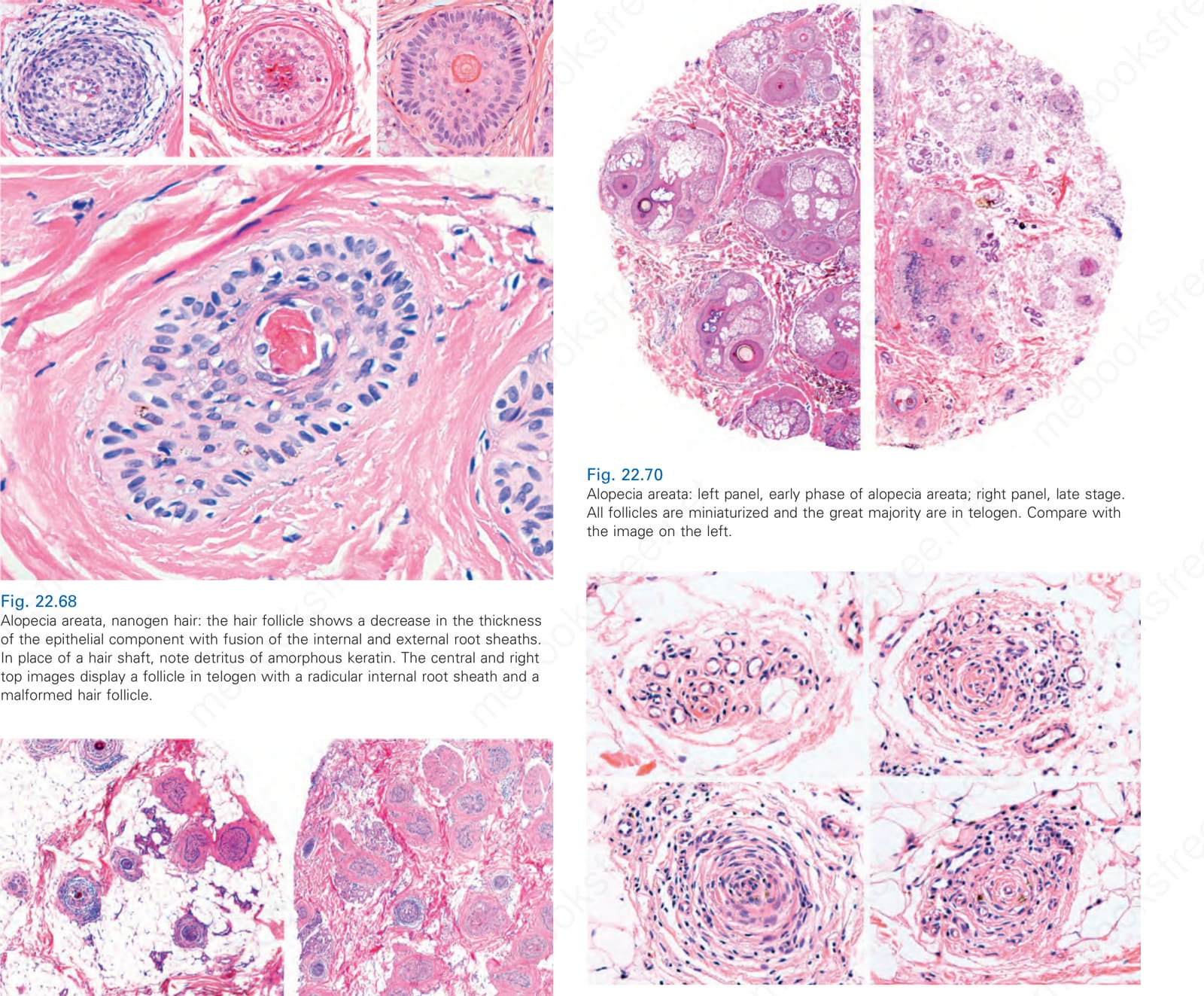
Fig. 22.69 (A, B) Alopecia areata, late stage: there is a remarkable increase in catagen/ telogen follicles, and a sparse peribulbar lymphocytic infiltrate with formation of stellae.
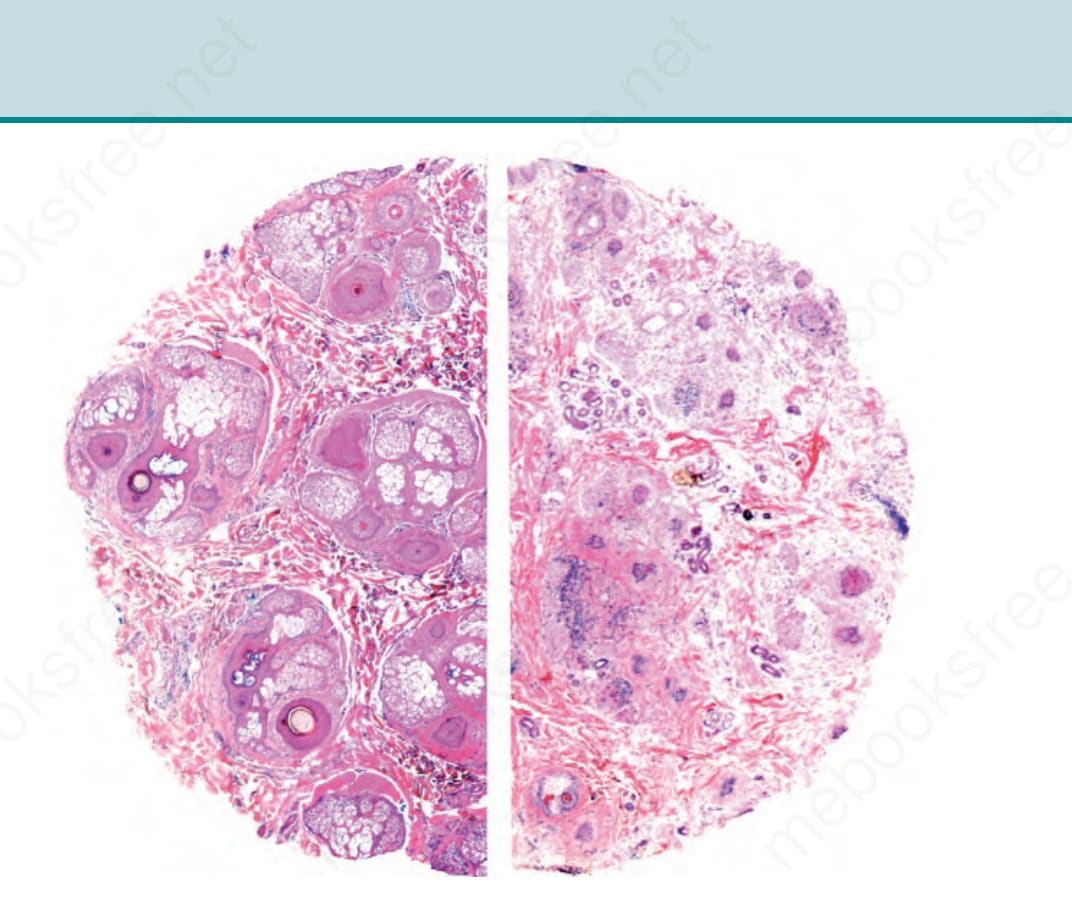
Fig. 22.70 Alopecia areata: left panel, early phase of alopecia areata; right panel, late stage. All follicles are miniaturized and the great majority are in telogen. Compare with the image on the left.
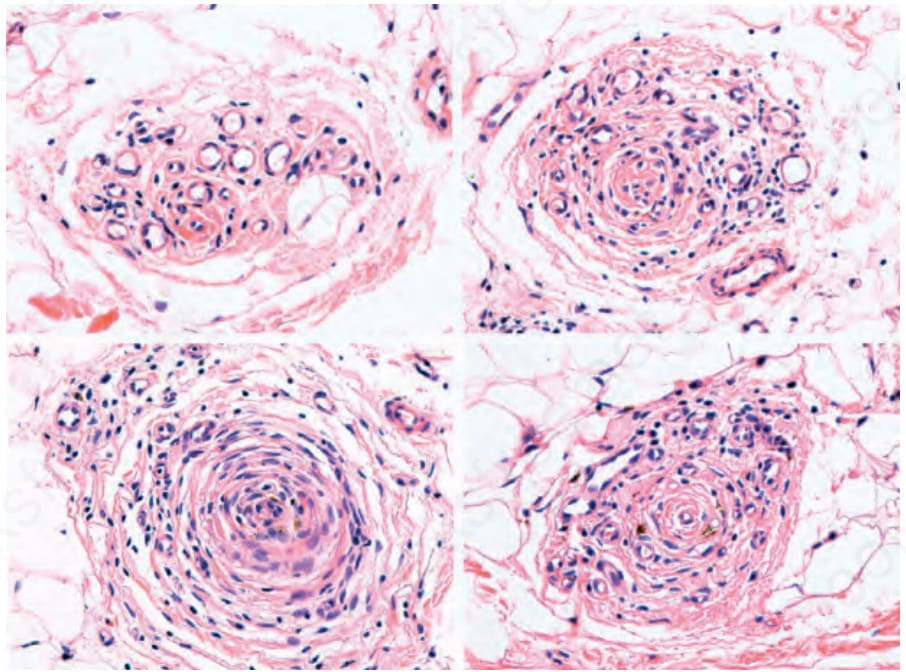
Fig. 22.71 Alopecia areata: different images of follicular stellae infiltrated by lymphocytes.
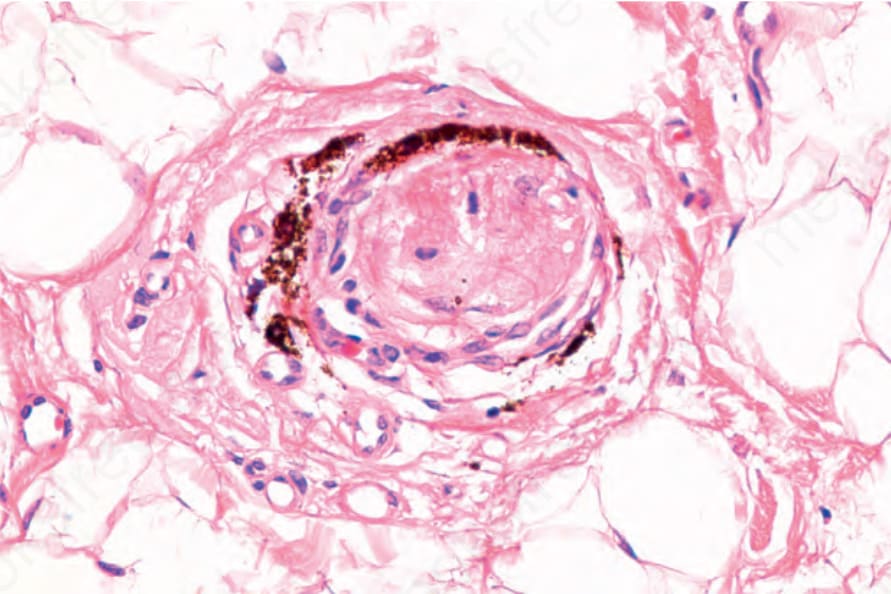
Fig. 22-65 (caption embedded in image / 圖說烘焙於圖內)
1077 Nonscarring alopecias
Pathogenesis and histologic features The mechanism leading to atrophy and loss of sebaceous glands in psoriasis is unknown. An explanation could be that some of the numerous cytokines secreted in psoriasis are responsible for the damage to the sebaceous glands or that they are lost because of the inflammation around the superior segment of the hair follicle.3
Histologic changes in both scarring alopecia and nonscarring psoriatic alopecia include typical features of psoriasis in the interfollicular epithelium, namely, psoriasiform hyperplasia of the epidermis, hyper- and parakeratosis with hypogranulosis, and exocytosis of neutrophils to the areas of parakeratosis. The infundibulum becomes dilated and there is a noticeable increase in the number of catagen and telogen hair follicles, pronounced atrophy and eventual loss of sebaceous glands, and a perifollicular lymphocyte inflammatory cell infiltrate in the superior and inferior segments of the hair follicle, including the hair bulb. There may be some miniaturization. The inflammation may lead to a granulomatous foreign body reaction with follicular destruction. At a later stage perifollicular fibrosis and fibrous tracts with inflammation may be observed (Fig. 22.73). Sometimes the changes in the superficial epidermis closely simulate those seen in seborrheic dermatitis (Fig. 22.74).3,4,7,19 Psoriatic alopecia associated with tumor necrosis factor-alpha inhibitors is histologically very similar to conventional psoriatic alopecia but more severe with a more prominent inflammatory cell infiltrate including plasma cells and eosinophils.
Alopecia areata incognita may be particularly difficult to differentiate from chronic telogen effluvium as both share a large number of hair follicles in telogen.7,97 However, dermoscopy in the former shows the presence of a larger number of yellow dots; furthermore, there may be a greater tendency to miniaturization.88 Recently, with the use of immunohistochemistry there has also been an emphasis in the detection of high levels of UL16 binding protein-3 (ULBP3) as an aid in the diagnosis of alopecia areata incognita88,98
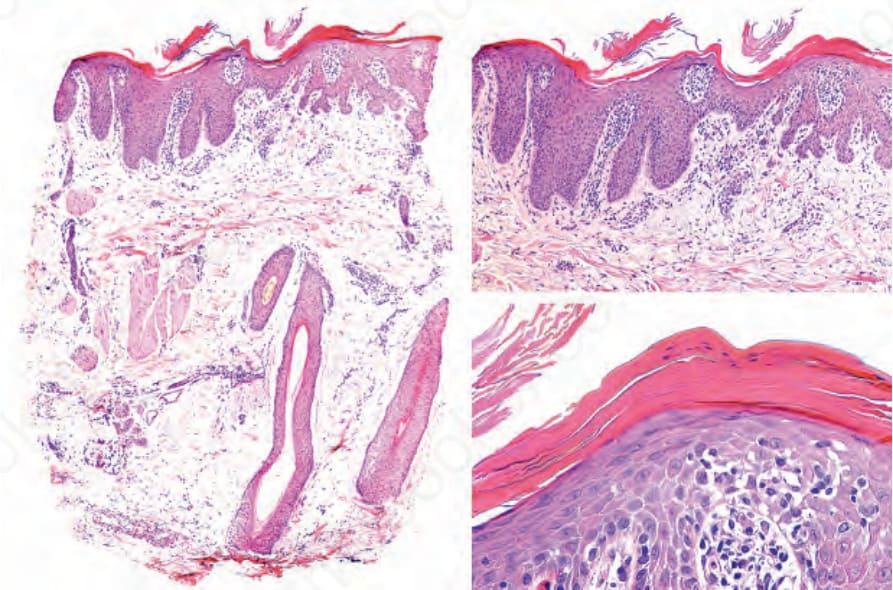
Fig. 22.73 Psoriasis. On the left the loss of sebaceous glands and follicular units is evident. On the right panel epidermal psoriatic changes including elongation of the rete ridges, hyperkeratosis, parakeratosis, hypogranulosis and corneal neutrophils.
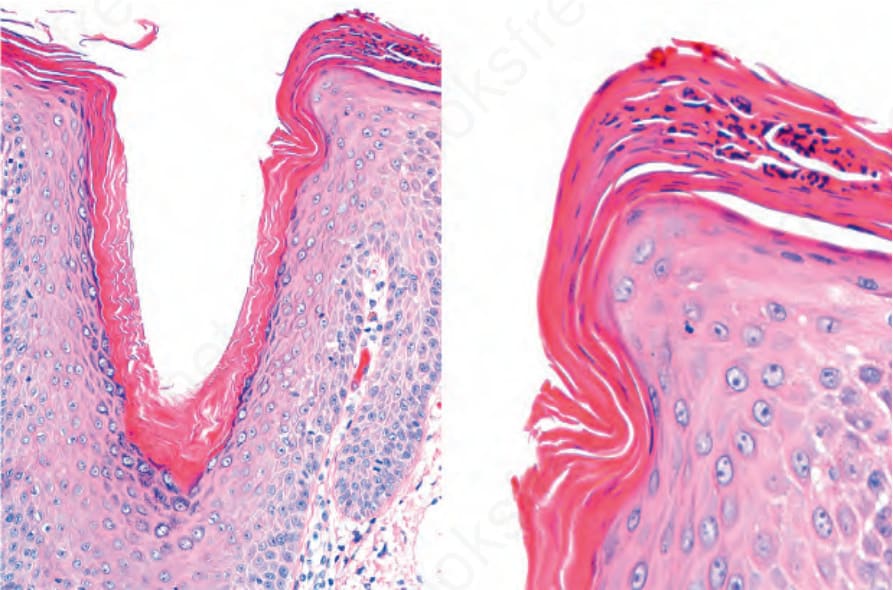
Fig. 22.74 Psoriasis of the scalp with changes simulating of seborrheic dermatitis. There is hyperkeratosis and parakeratosis with collections of neutrophils, more pronounced at the lip of the follicular ostium.