疾病定義與分類
- 雄性禿 (androgenetic alopecia) 又稱為常見性禿髮 (common baldness) 以及男性與女性型態落髮 (male and female pattern hair loss)。
- 在基因易感的男性中,androgenetic alopecia 由雄激素 (androgens) 所引起;在女性中,雄激素所扮演的角色較不明確。
- 典型上,頭皮毛髮會在十二至四十歲之間發生進行性微小化 (progressive miniaturization)。
臨床特徵 (Clinical Features)
-
雄激素是正常人類毛髮生長的主要調節者。青春期後,雄激素促使毳毛毛囊 (vellus hair follicles) 轉變為大型、有色素的終毛 (terminal hairs)。然而,雄激素也可能逆轉此過程,導致終毛逐漸被毳毛取代,進而引發 androgenetic alopecia。
-
androgenetic alopecia 是一種非常常見的疾病,為成人最常見的落髮類型;在 50 歲時至少影響 50% 的男性族群,並在 70 歲時影響約 40% 的女性族群。在 40 至 70 歲男性中,頭頂 (vertex) 與完全發展型 androgenetic alopecia 的盛行率隨年齡增加,但病變侷限於額部 (frontal region) 之男性比例則相當固定。
-
androgenetic alopecia 病人通常有禿髮的家族史。缺乏此類家族史可降低風險,但無法排除發病的可能性。罕見情況下,本病與高雄激素血症 (hyperandrogenism) 相關,並伴隨雄激素過多的其他表現。
-
在男性中,本病通常在青春期後早期即開始,主要影響頭皮的頂部 (crown)、頭頂 (vertex)、額部 (frontal)、中央 (central) 與顳部 (temporal) 區域。通常不侵犯枕部 (occipital) 與下頂部 (lower parietal) 區域 (Fig. 22.35)。有些病例於青春期及兒童期出現,通常與強烈的遺傳傾向相關。曾有人提出,在第三個十年結束前即發生落髮的病人,可能比未受影響的男性有較高的冠狀動脈疾病 (coronary artery disease) 風險。然而,其他研究則將此關聯限縮於侷限在頭頂之禿髮,且有些作者則完全否定此關聯。
-
在年長的 androgenetic alopecia 病人中,已注意到本病與胰島素阻抗相關疾病 (insulin resistance-linked diseases) 之關聯,以及與糖尿病及心血管疾病較高死亡率之關聯。
-
本病似乎也是攝護腺癌 (prostate cancer) 與良性攝護腺增生 (benign prostatic hyperplasia) 的危險因子。
-
毛髮與頭皮的皮膚鏡 (dermoscopy) 與錄影皮膚鏡 (videodermoscopy) 顯示毛幹直徑有重要差異,可見不定型毛 (indeterminate hairs) 與終毛混雜存在。其應用使臨床診斷與治療反應之監測更為準確。受落髮影響最嚴重的部位易於定位,因此將是最佳的切片部位 (見 Figs 22.35–22.37)。
-
罹患 androgenetic alopecia 的男性通常不需要實驗室檢查。在受影響女性中是否進行實驗室檢查,取決於多種因素,包括家族史、臨床表現、病程演變,以及發病年齡。若女性有月經不規則、不孕病史、多囊性卵巢 (polycystic ovaries),或具提示高雄激素血症之身體徵象(多毛症 (hirsutism)、對治療無反應的囊腫型痤瘡 (cystic acne unresponsive to treatment)、黑色棘皮症 (acanthosis nigricans)、男性化 (virilization),或乳漏 (galactorrhea)),則應進一步檢查,包括游離與總睪固酮 (free and total testosterone) 濃度。若這些數值偏高,應確定其來源,尤其需注意是否存在卵巢腫瘤 (ovarian tumor) 或腎上腺增生 (adrenal hyperplasia)。在無家族史或無提示高雄激素血症之身體徵象的 androgenetic alopecia 女性中,通常不需要進行任何實驗室檢查。
-
在 androgenetic alopecia 中,輕柔的拉髮試驗 (hair pull) 為正常。只能拔下少數幾根毛髮,且這些都處於休止期 (telogen phase)。由於受影響區域休止期毛髮的計數明顯偏高,拔髮試驗 (hair pluck) 可能給出誤導性的結果。這是因為在早期階段,由於生長期 (anagen phase) 縮短,毛囊更頻繁地進入休止期。本病可能與休止期落髮 (telogen effluvium) 混淆,但鑑別容易,因為 telogen effluvium 是廣泛性的,而 androgenetic alopecia 則是侷限性的。
-
它發展得早得多 (Fig. 22.37)。女性型落髮 (female pattern hair loss) 已被發現與高泌乳素血症 (hyperprolactinemia) 相關。
-
androgenetic alopecia 中的兩種落髮型態有時被稱為 Hamilton-Norwood「男性型 (male pattern)」與 Ludwig「女性型 (female pattern)」(Fig. 22.38)。然而,兩者有相當程度的重疊。有些女性呈現男性型,反之亦然。韓國男性傾向於呈現比白種人更偏「女性型」的毛髮稀疏型態。這些相反型態的表現並不能界定個體的荷爾蒙狀態;具男性型禿髮的女性不必然伴隨高雄激素血症。
-
不同的臨床表現,以及枕部頭皮一般獲得保留之事實,乃是頭皮不同區域真皮 (dermis) 之不同胚胎起源的結果。額部/頂部頭皮的真皮源自神經嵴 (neural crest),而枕部頭皮的真皮則源自中胚層 (mesoderm)。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
-
androgenetic alopecia 起因於毛囊大小的進行性減小及其轉變為毳毛型態 (Fig. 22.39,並見 Figs 22.12 與 22.14)。然而,亦曾觀察到此微小化可能在僅僅數個週期內突然發生。此現象是 5α-reductase type II 活性的直接結果,該酵素主要存在於外根鞘 (external root sheath) 與毛球乳頭 (hair bulb papilla)。此酵素將睪固酮 (testosterone) 轉換為雙氫睪固酮 (dihydrotestosterone),後者對毛囊外根鞘與毛囊乳頭 (follicular papilla) 中的雄激素受體 (androgen receptors) 具有極高親和力。荷爾蒙-受體複合體活化負責使大型終毛逐漸轉變為微小化毛囊的相關基因。患有本病的年輕女性與男性,其額部毛囊中的 5α-reductase 與雄激素受體濃度,較枕部毛囊為高。Finasteride 抑制 5α-reductase type-2 同功酶,降低 dihydrotestosterone 濃度並促進男性的毛髮生長。
-
然而,雄激素在女性型落髮變異型中所扮演的角色尚未完全確立。頭皮落髮是女性高雄激素血症的特徵之一,但許多 female pattern hair loss 的女性並無雄激素過多的其他臨床或生化證據。Female pattern hair loss 可能是一種多因子、基因決定的特質,且雄激素依賴 (androgen-dependent) 與雄激素非依賴 (androgen-independent) 機轉都可能對此表現型有所貢獻。其他可調節雄激素與雌激素 (estrogens) 作用、並作為對抗 androgenetic alopecia 之保護因子的酵素,包括 cytochrome p450 aromatase 與 17β-hydroxysteroid dehydrogenase。這些酵素會使毛囊內局部雌激素濃度增加,並隨性別、年齡與毛囊位置而有所變化。
-
在男性型與女性型落髮兩者中,皆有生長期持續時間下降、休止期毛囊百分比上升,以及空毛期 (kenogen phase) 之頻率增加與延長,尤其在毛囊高度微小化的病例中。休止期毛囊似乎走上一條替代路徑,並非接續一個新的早期生長期,而是長時間維持為一個空毛囊。最終結果是無色素的毛幹,逐漸變得更細更小,最終導致無毛幹的空毛囊(毛囊凋亡 (teloptosis))。有些毛囊可能逐漸消失,並被纖維束 (fibrous tracts) 取代。
-
為進行 androgenetic alopecia 的顯微研究,應取得兩個 4-mm 環鑽切片 (punch biopsies):一個作為對照,取自枕部健康頭皮,另一個取自受影響區域。兩個切片皆須自漏斗部 (infundibulum) 下方水平切片,以進行比較性定量。終毛與毳毛的比例約為 7:1。比例為 4:1 或更低則提示 androgenetic alopecia。
-
本病早期與晚期的組織學特徵有所不同。應計數終毛、不定型毛與毳毛。當與取自枕部之正常頭皮切片進行比較時,較易察覺毛囊的微小化與毛囊單位 (follicular units) 的脫落 (Fig. 22.40)。此過程並非以均勻方式呈現,因為起初它可能是局灶性的,甚至可能只影響一個毛囊單位內的部分毛囊 (Fig. 22.41)。toluidine blue 染色對於凸顯外根鞘與內根鞘 (outer and inner root sheaths),使其與淡染的毛幹形成對比,特別有用 (Fig. 22.42,並見 Fig. 22.15)。
-
組織學上,終毛逐漸轉變為毳毛 (Figs 22.43 與 22.44)。真皮乳頭 (dermal papilla) 與毛球 (bulb) 的大小減小。毛幹直徑亦減小,並且在不同毛囊間有明顯差異。此組織學特徵與臨床上觀察到的微小化密切相關 (Fig. 22.45)。
-
雖然毛髮總數正常,但若計數是在真皮與皮下脂肪交界處進行,則會顯得減少,因為依定義終毛數量已減少。即使這些變化在垂直切面 (vertical sections) 中亦可見到 (見 Fig. 22.39),但較難判讀與定量。
-
伴隨這些變化,毛囊週期的持續時間以生長期為代價而縮短。因此,在病程演變中或完全建立的 androgenetic alopecia 病人中,極常在微小化毛囊成分中發現退化期 (catagen) 與休止期毛囊數量的增加。女性變異型的組織學圖像與此相同。
-
輕度至中度的 T 淋巴球發炎細胞浸潤經常圍繞毛囊上三分之一,並伴隨離散的毛囊周圍同心圓性纖維化 (perifollicular concentric fibrosis),尤其在非裔病人中 (Fig. 22.46,並見 Fig. 22.17)。此現象的意義尚待確定,因為不同於原發性瘢痕性禿髮 (primary scarring alopecias),此處並無毛囊幹細胞的喪失。然而,幹細胞轉變為前驅細胞 (progenitor cells) 的過程似乎確有減少。
-
毛囊的微小化影響整個毛囊,包括在晚期影響立毛肌 (arrector pili muscle) 與皮脂腺 (sebaceous gland)。在微小化毛囊中,立毛肌的退化與被脂肪組織取代,以及與隆突部 (bulge) 接觸的喪失,似乎是決定一個 androgenetic alopecia 是否會對治療有反應的關鍵因素。這兩個結構之間結合的持續存在,是禿髮可逆性的徵象,因為即使在過程的晚期階段,它似乎仍能保護隆突部幹細胞的完整性。
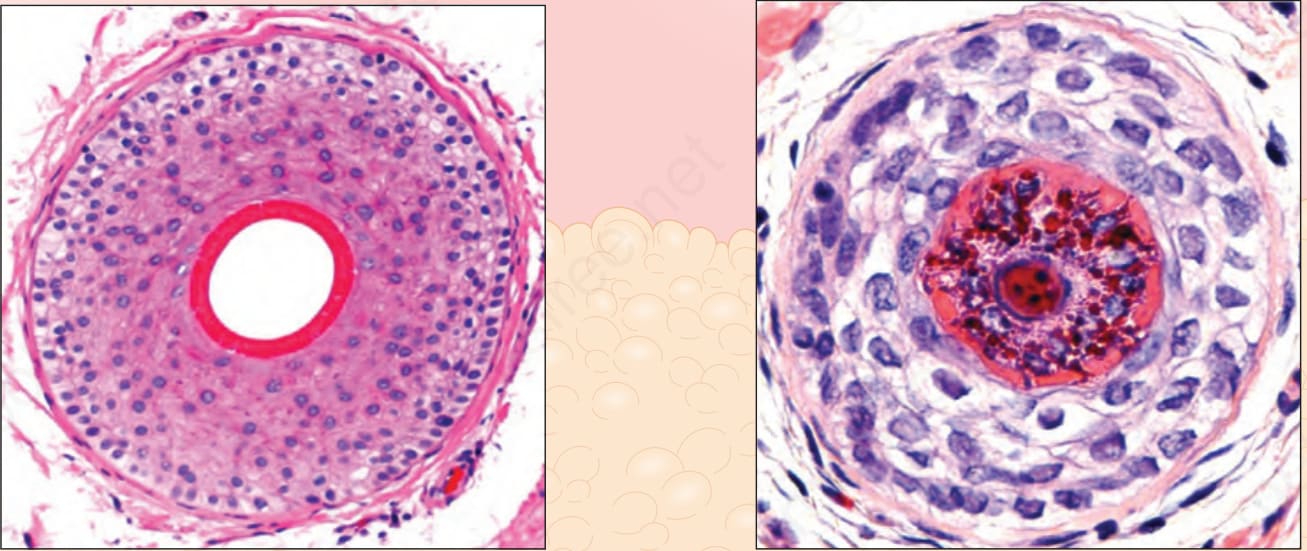
圖 22-12:終毛生長期毛囊與毳毛,垂直與水平切面:終毛毛囊到達脂肪層並深埋其中。毳毛 (vellus hairs) 與微小化毛囊 (miniaturized follicles) 位於真皮內。注意終毛與毳毛中毛幹與內根鞘 (inner root sheath) 相對大小的差異。Courtesy of M. Mejia, MD, Universidad Pontificia Bolivariana, Medellín, Colombia.
Fig. 22.12 Terminal anagen and vellus hair, vertical and horizontal sections: the terminal hair follicles reach the fat and are deeply embedded within it. The vellus hairs and miniaturized follicles are located within the dermis. Note the differences between the relative size of the hair shaft and the inner root sheath in terminal and vellus hairs. Courtesy of M. Mejia, MD, Universidad Pontificia Bolivariana, Medellín, Colombia.
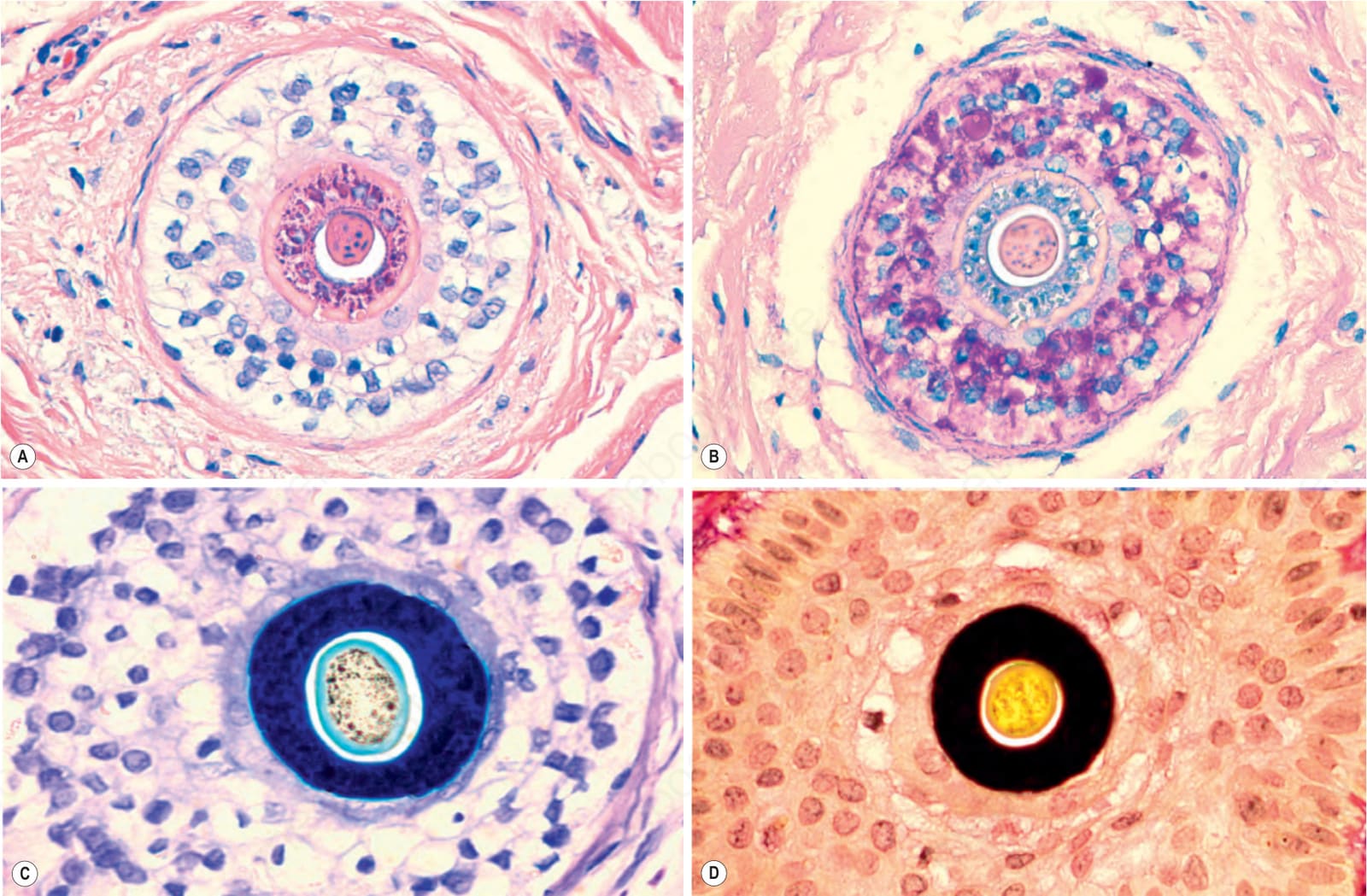
圖 22-15:毳毛,水平切面:注意毛幹相對於內根鞘 (inner root sheath) 的口徑,於:(A) 粉紅色,hematoxylin and eosin;(B) 灰色,PAS;(C) 藍色,toluidine blue;以及 (D) 黑色,elastic tissue stain。
Fig. 22.15 Vellus hair, horizontal section: note the caliber of the hair shaft compared to the inner root sheath in: (A) pink, hematoxylin and eosin; (B) gray, PAS; (C) blue, toluidine blue; and (D) black, elastic tissue stain.
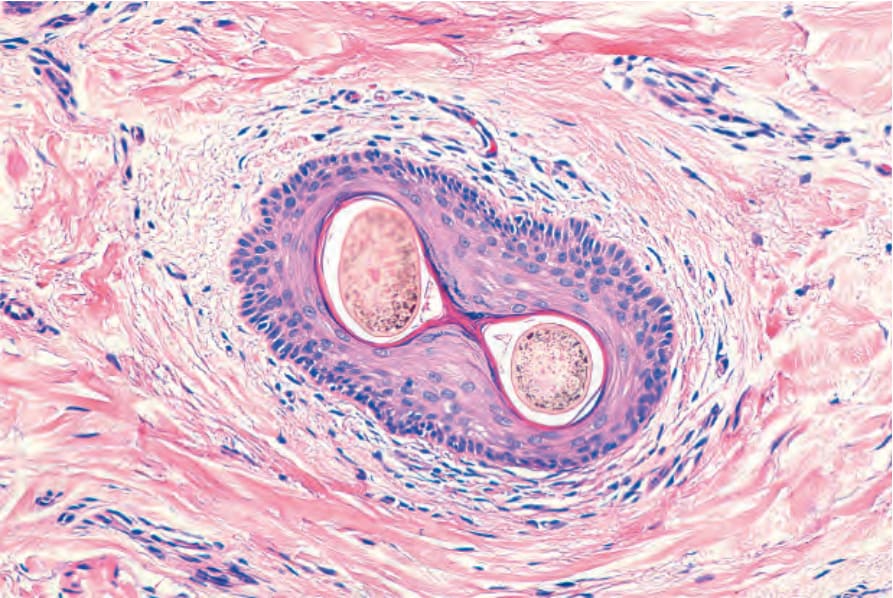
圖 22-17:漏斗部 (infundibulum)。水平切面。管壁由鱗狀複層角化上皮 (squamous stratified keratinized epithelium) 構成。周圍真皮被一些淋巴球浸潤。有兩根毛幹自單一毛孔 (ostium) 露出。
Fig. 22.17 Infundibulum. Horizontal section. The wall is made up of squamous stratified keratinized epithelium. The surrounding dermis is infiltrated by some lymphocytes. There are two hair shafts emerging from a single ostium.

圖 22-35:男性雄性禿 (male androgenetic alopecia):此病人呈現確立的男性型禿髮 (male pattern baldness),有雙額髮際線後退與頭皮頭頂 (vertex) 落髮。在右側皮膚鏡影像中,注意毛囊間口徑的差異。Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
Fig. 22.35 Male androgenetic alopecia: this patient shows well-established male pattern baldness with bifrontal hair line recession and hair loss on the scalp vertex. In the dermoscopic image on the right, note the difference in caliber between hair follicles. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
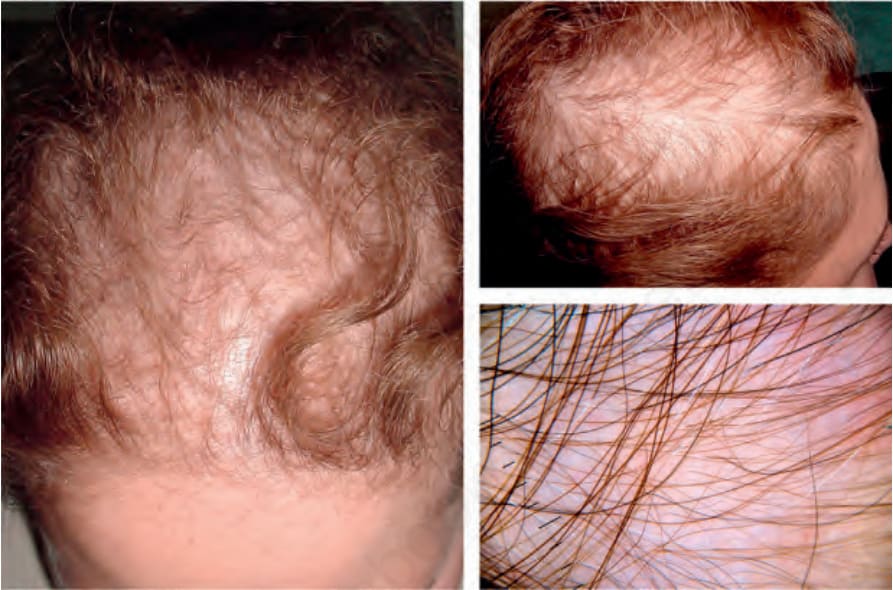
圖 22-36:女性型落髮 (female pattern hair loss):此例顯示一個典型範例,呈現頂部 (parietal) 與後額部落髮。注意額部髮際線 (frontal hairline) 的保留。在右下方皮膚鏡影像中,注意在無發炎背景上因廣泛微小化所致的落髮。Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
Fig. 22.36 Female pattern hair loss: this example shows a typical example with parietal and posterior frontal hair loss. Note the sparing of the frontal hairline. In the dermoscopic image on the right lower panel, note the hair loss due to extensive miniaturization on a noninflammatory background. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.

圖 22-37:女孩的女性型落髮 (female pattern hair loss):可觀察到早期落髮,伴隨頂間線 (interparietal line) 的變寬。在右下方皮膚鏡影像中,注意有微小化的傾向,毛囊呈現不同口徑。Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
Fig. 22.37 Female pattern hair loss in a girl: early hair loss is observed with widening of the interparietal line. In the dermoscopic image on the right lower panel, note a tendency to miniaturization with hair follicles of different calibers. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
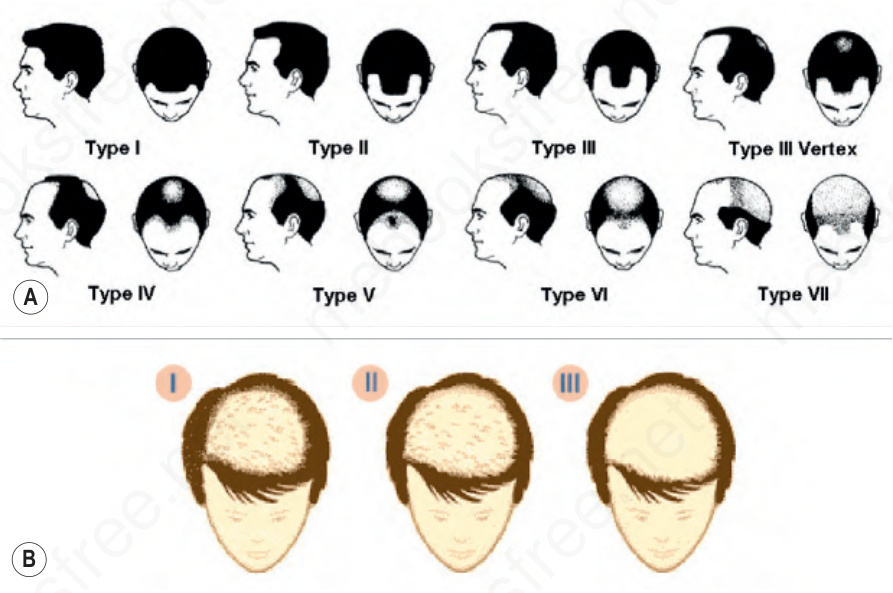
圖 22-38:(A) 男性型雄性禿的 Hamilton-Norwood 分類(上)。Reproduced with permission from Norwood, O.T. (1984) Hair transplant surgery. Springfield: Charles C. Thomas, p 6. (B) 女性型落髮的 Ludwig 型態(下)。Reproduced with permission from Ludwig, E. (1977) Classification of the types of androgenetic alopecia occurring in the female sex. British Journal of Dermatology, 97;247–254.
Fig. 22.38 (A) Hamilton-Norwood classification of male pattern androgenetic alopecia (top). Reproduced with permission from Norwood, O.T. (1984) Hair transplant surgery. Springfield: Charles C. Thomas, p 6. (B) Ludwig patterns of female pattern hair loss (bottom). Reproduced with permission from Ludwig, E. (1977) Classification of the types of androgenetic alopecia occurring in the female sex. British Journal of Dermatology, 97;247–254.
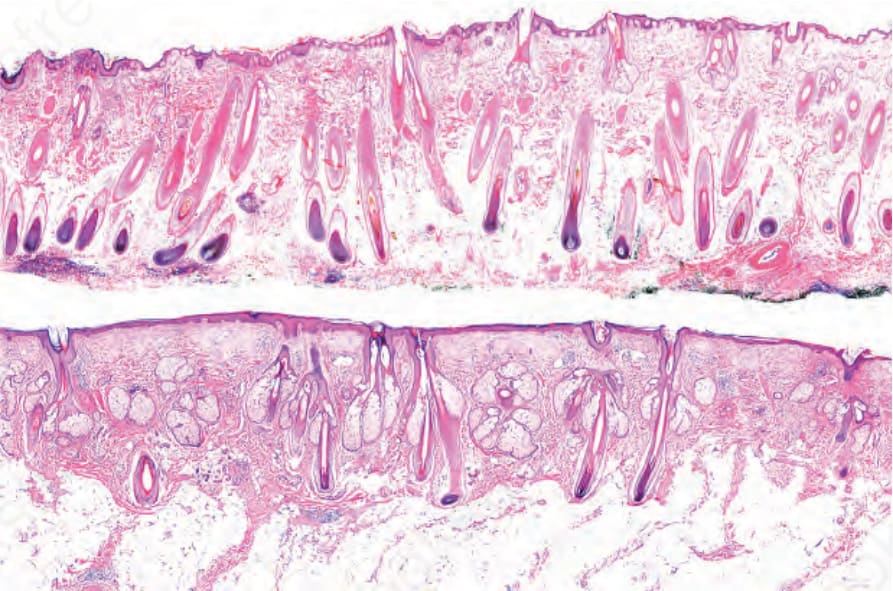
圖 22-39:雄性禿 (androgenetic alopecia)。垂直切面。上圖為正常頭皮,有大量終毛毛囊延伸至深部皮下脂肪。下圖中,注意一名晚期 androgenic alopecia 病人的頭皮切片。勉強可見有少數細小的毛囊,僅僅到達真皮與皮下組織之間的界線。
Fig. 22.39 Androgenetic alopecia. Vertical sections. In the top panel normal scalp with numerous terminal hair follicles extending into the deep subcutaneous fat. In the lower panel, note a scalp biopsy from a patient with advanced androgenic alopecia. Barely visible, are a few thin follicles which only just reach the limit between the dermis and the subcutaneous tissue.
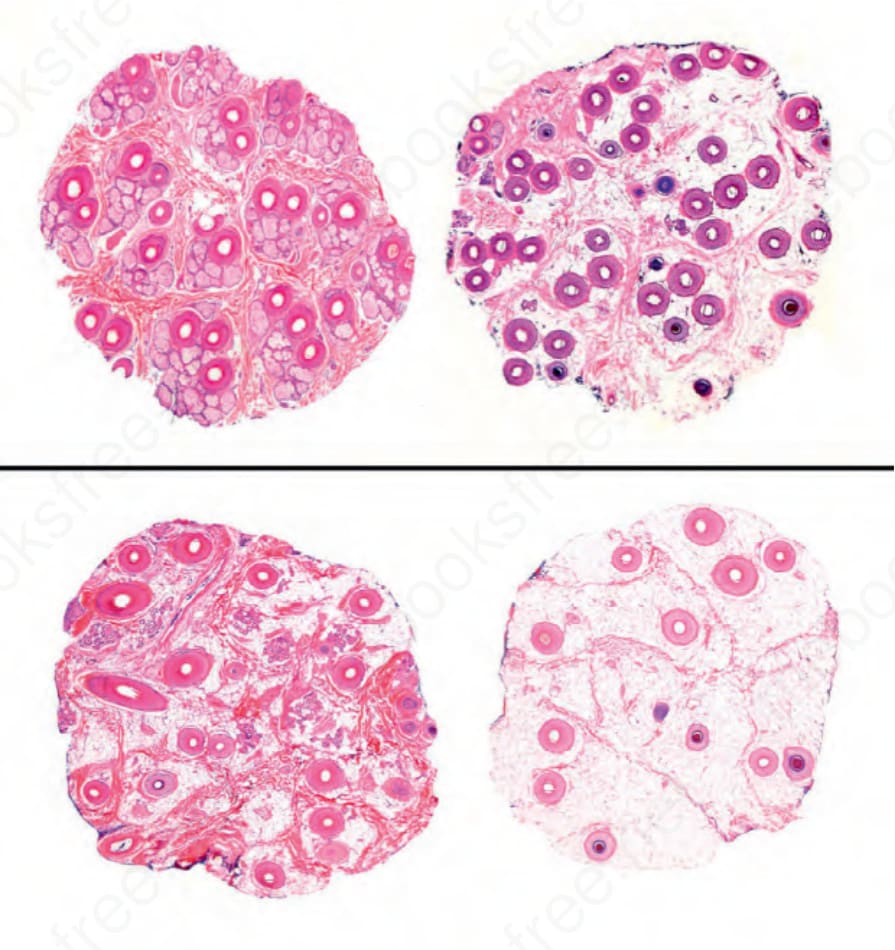
圖 22-40:雄性禿 (androgenetic alopecia),水平切面:上圖為取自枕部之正常頭皮切片。有大量由大小一致之毛囊所構成的毛囊單位 (follicular units)。下方為取自額部禿髮區域的切面,超過半數的毛囊已微小化(毳毛 (vellus))或正處於微小化過程中。毛囊單位已消失,且皮下脂肪中有大量星狀殘跡 (stellae)。
Fig. 22.40 Androgenetic alopecia, horizontal sections: in the upper panel, a biopsy of normal scalp taken from the occipital area. There are numerous follicular units formed by follicles of uniform size. Below are sections from an area of frontal alopecia with more than half of the follicles miniaturized (vellus) or in the process of miniaturization. The follicular units have disappeared and in the subcutaneous fat there are numerous stellae.
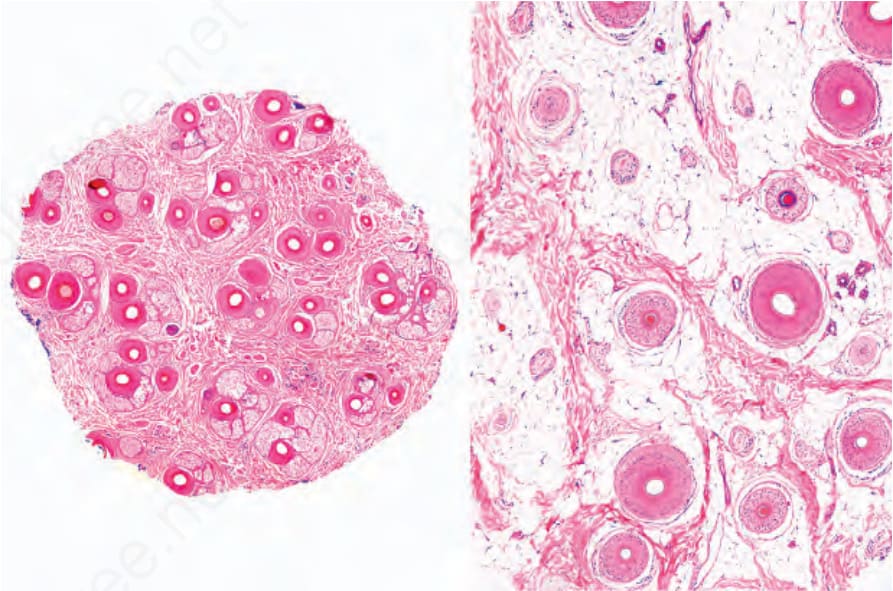
圖 22-41:雄性禿 (androgenetic alopecia),水平切面。此影像凸顯微小化現象並非均勻,而是影響局灶區域,並在其間留下正常區域。右圖顯示更深層次的切面。
Fig. 22.41 Androgenetic alopecia, horizontal sections. This image highlights how the miniaturization phenomenon is not uniform but affects focal areas leaving normal areas in between. A section at a deeper level is shown in the right panel.
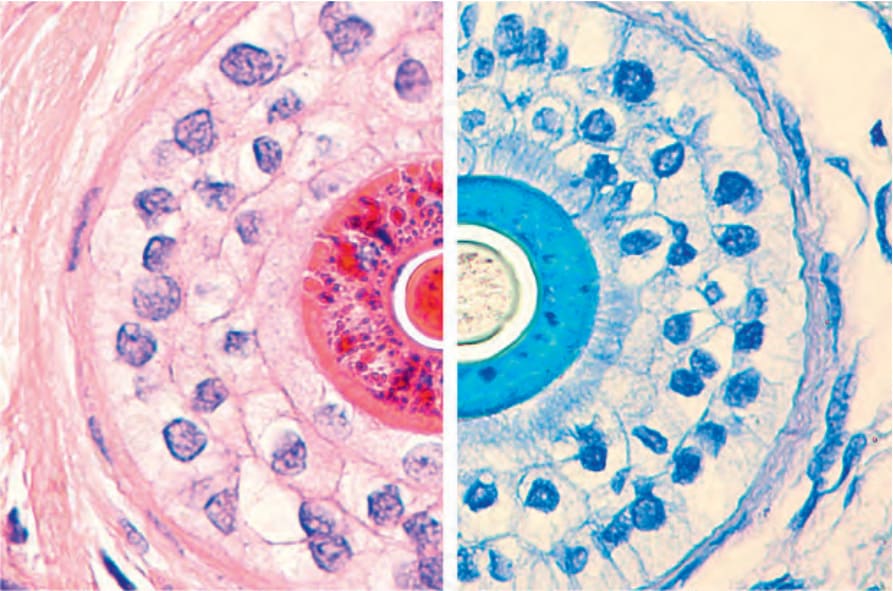
圖 22-42:微小化毛囊 (miniaturized hair follicle)。比較左側內根鞘的染色(hematoxylin and eosin 染呈紅色)與右側(toluidine blue 染呈藍色)。
Fig. 22.42 Miniaturized hair follicle. Compare the staining of the inner root sheath on the left (red with hematoxylin and eosin) with the one on the right (blue with toluidine blue).
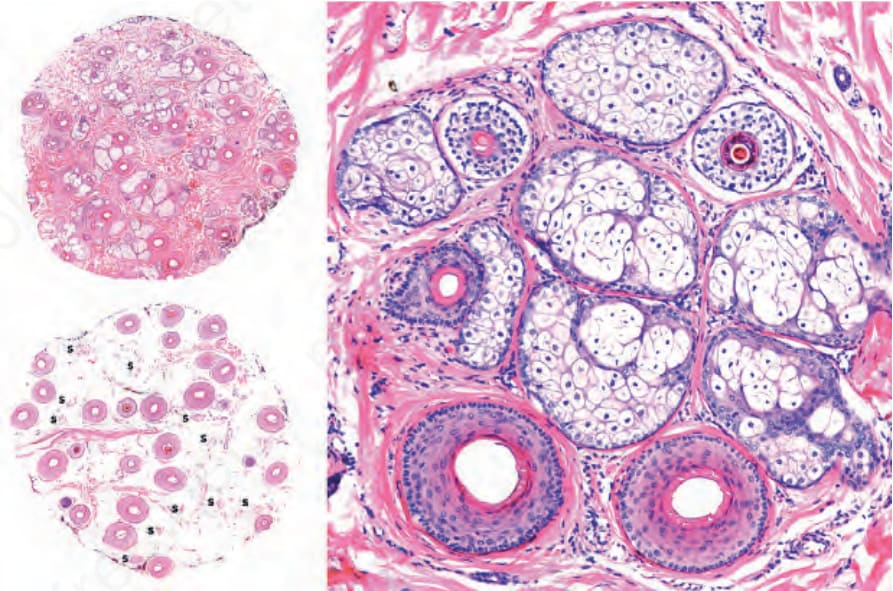
圖 22-43:雄性禿 (androgenetic alopecia),水平切面:(左)此為取自頂間區域的頭皮切片。在淺層切面(上)中,有大量微小化毛囊。在皮下組織層次的切面(下)中,許多毛囊已被毛囊星狀殘跡 (follicular stellae, S) 取代;(右)毛囊單位於底部有兩個終毛毛囊,頂部有三個微小化毛囊。
Fig. 22.43 Androgenetic alopecia, horizontal sections: (left) this is a scalp biopsy taken from the interparietal area. In the superficial section (top), there are numerous miniaturized hair follicles. In the section at the level of the subcutaneous tissue (bottom), many of the follicles have been replaced by follicular stellae (S); (right) follicular units with two terminal follicles at the bottom and three miniaturized follicles at the top.
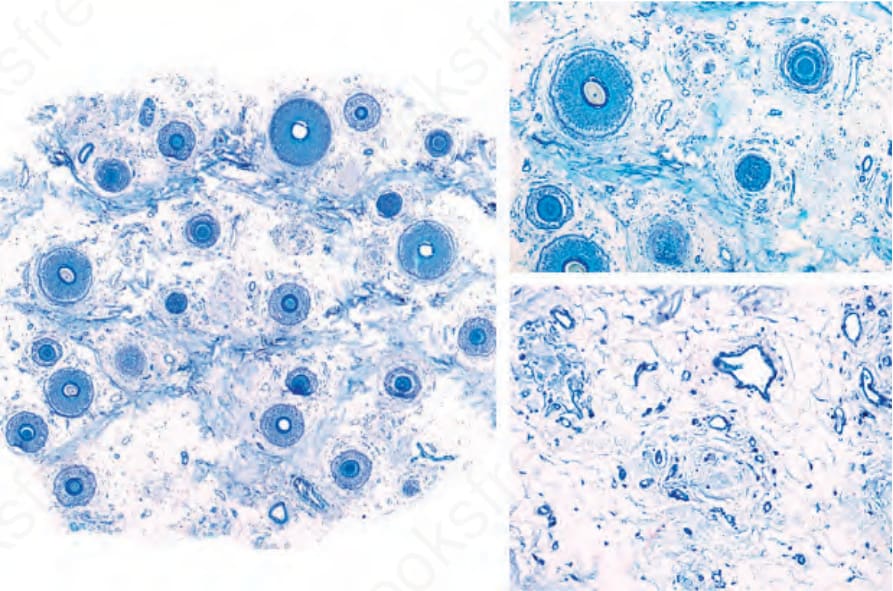
圖 22-44:雄性禿 (androgenetic alopecia):在此較晚期的範例中,毛囊密度大幅減少,有許多微小化毛囊(左)與大量星狀殘跡 (stellae)(右)。Toluidine blue 染色。
Fig. 22.44 Androgenetic alopecia: in this more advanced example, the follicular density is greatly reduced with many miniaturized hair follicles (left) and numerous stellae (right). Toluidine blue stain.
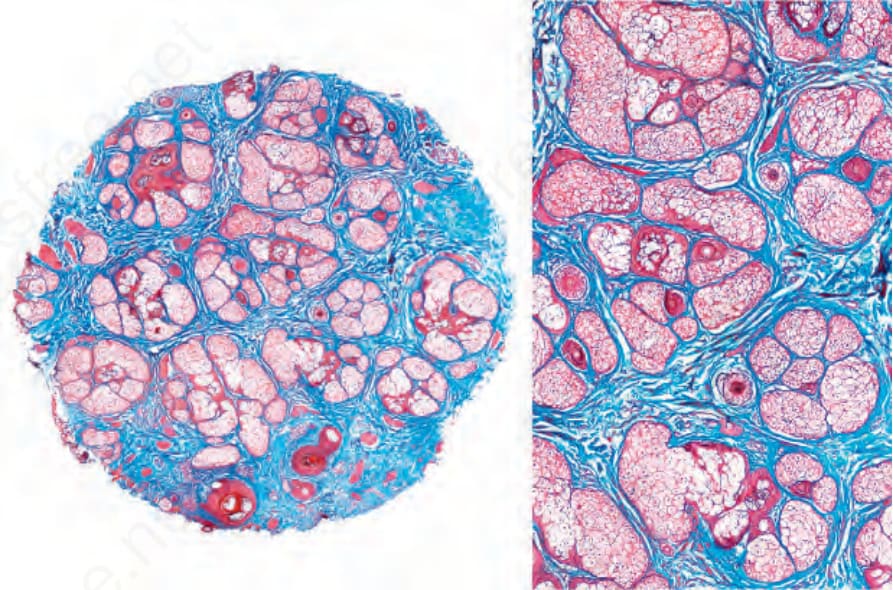
圖 22-45:雄性禿 (androgenetic alopecia):幾乎所有毛囊都已微小化,皮脂腺 (sebaceous glands) 顯得突出。毛幹幾乎難以辨識。Masson trichrome 染色。
Fig. 22.45 Androgenetic alopecia: almost all hair follicles are miniaturized and the sebaceous glands appear prominent. The hair shafts are barely visible. Masson trichrome stain.
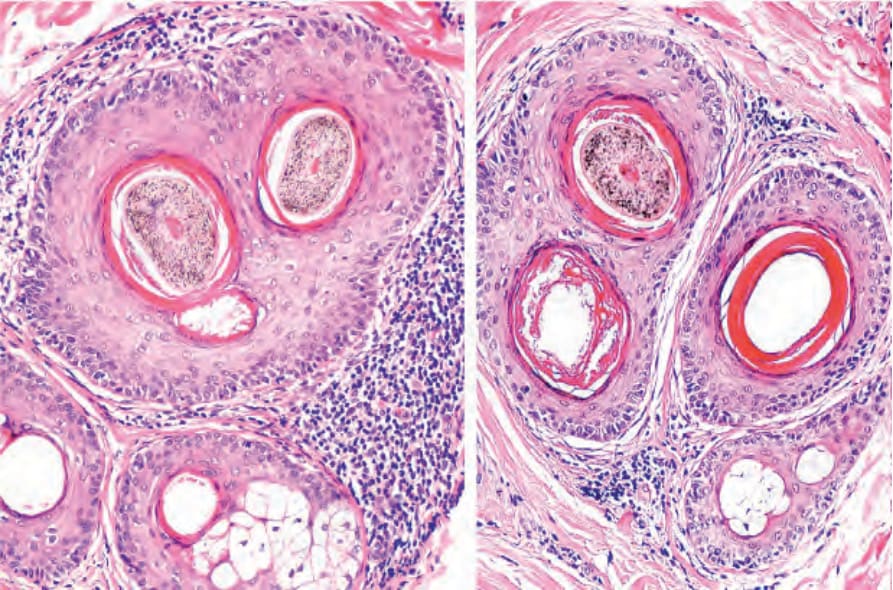
圖 22-46:複合毛漏斗部 (compound hair infundibulum) 被淋巴球浸潤與輕度同心圓性纖維化 (concentric fibrosis) 圍繞,見於一名 androgenetic alopecia 病人。
Fig. 22.46 Compound hair infundibulum surrounded by a lymphocytic infiltrate and mild concentric fibrosis in a patient with androgenetic alopecia.
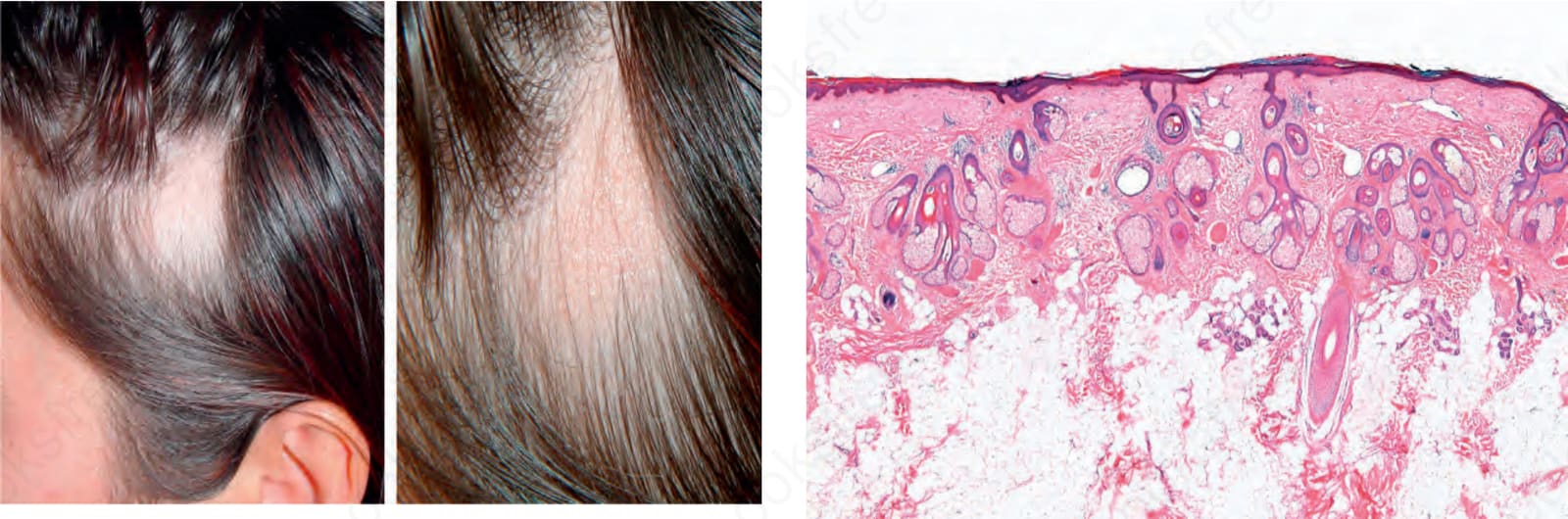
圖 22-52:三角形禿髮 (triangular alopecia):注意特徵性的三角形禿髮斑塊。在右圖中,特寫顯示無發炎變化。Courtesy of A.M. Aristizábal, MD, CES, Medellín, Colombia.
Fig. 22.52 Triangular alopecia: note the characteristic triangular patch of alopecia. In the right panel, a close-up view shows absence of inflammatory changes. Courtesy of A.M. Aristizábal, MD, CES, Medellín, Colombia.
- 此過程。皮脂腺保持正常,但在病程長久的 androgenetic alopecia 中,可能觀察到外分泌腺 (eccrine glands) 增生,有時形成類似汗管瘤 (syringoma-like) 的結構 (Fig. 22.47)。
- 在較深的切面中,毛球出現於不同深度,且可能局灶性完全缺失,僅留下毛囊星狀殘跡 (follicular stellae)。這些星狀殘跡見於多種情況中,反映出微小化的毛囊,或是已進入退化期 (catagen) 或休止期 (telogen) 階段的毛囊 (Fig. 22.48)。隨著星狀殘跡成熟,它們的血管化程度降低,呈現為帶藍灰色調的纖維性瘢痕,這對應於彈性組織的濃縮物,稱為 Arao-Perkins bodies (Fig. 22.49)。在晚期 androgenic alopecia 中,星狀殘跡變得異常增厚,可能阻礙毛囊的生長。
- 終毛/毳毛比例 (7:1) 大幅降低,可變化為 1:1 甚至 1:2。雖然起初毛囊數量正常,但在病程長久的疾病中可能有真正的減少。因此,切片除了顯示個別毛囊大小的減小外,也可能顯示毛囊密度的下降。有時其外觀可能更提示瘢痕性禿髮 (scarring alopecia) (Fig. 22.50)。
鑑別診斷 (Differential Diagnosis)
- 最重要的鑑別診斷是與呈現瀰漫性非瘢痕性禿髮 (diffuse nonscarring alopecia) 的疾病鑑別,包括慢性休止期落髮 (chronic telogen effluvium)、圓禿 (alopecia areata),以及型態分布性纖維化禿髮 (fibrosing alopecia in a pattern distribution)。在這些情況下,切片對於達成準確診斷至關重要。
- 雖然 androgenetic alopecia 可能顯示休止期毛髮數量增加,但 telogen effluvium 在臨床上更為瀰漫,且無微小化毛囊。取自枕部區域的切片極具價值,可用以記錄毛囊侵犯是否為瀰漫性。然而,重要的是要注意,兩種疾病可能同時出現,且 chronic telogen effluvium 可能揭露潛伏的 androgenetic alopecia。
- alopecia areata 可能顯示微小化毛囊,尤其在其瀰漫型 (diffuse form) 與非常慢性的病例中。然而,其特徵性表現為退化期與休止期毛囊數量的顯著增加,且通常存在稀疏的毛球周圍 (peribulbar) 淋巴球浸潤,有時伴隨嗜伊紅性球 (eosinophils)。然而,若無適當的臨床資訊,鑑別可能無法達成。
- 在型態分布性纖維化禿髮 (fibrosing alopecia in pattern distribution) 中 (Fig. 22.51),淋巴球發炎細胞浸潤影響漏斗部與毛囊峽部 (follicular isthmus),並有上皮與隆突細胞 (bulge cell) 的破壞。此外,
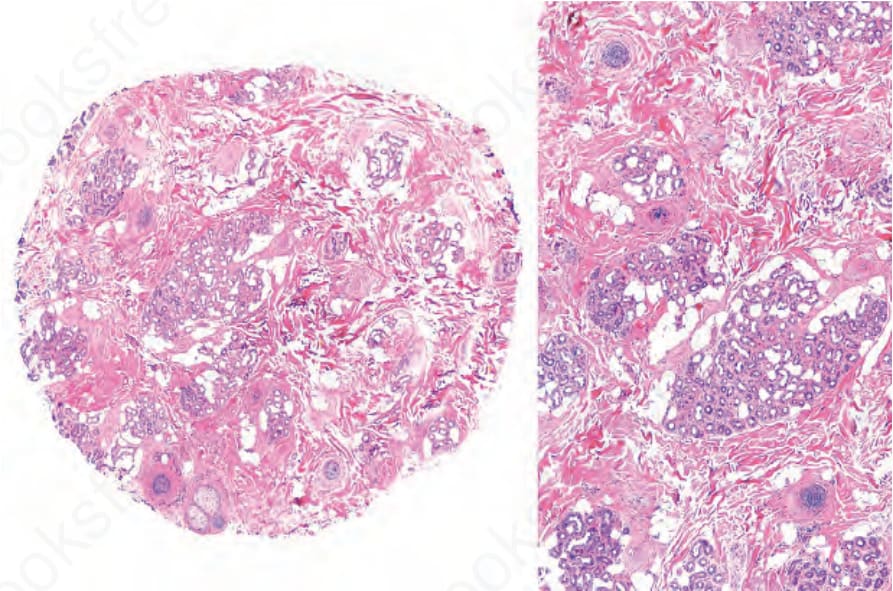
圖 22-47:汗腺導管增生 (sweat gland duct proliferation)。一例晚期 androgenetic alopecia,其毛囊結構被增生汗腺與導管之小葉所取代。
Fig. 22.47 Sweat gland duct proliferation. Case of advanced androgenetic alopecia with follicular structures replaced by lobules of hyperplastic sweat glands and ducts.
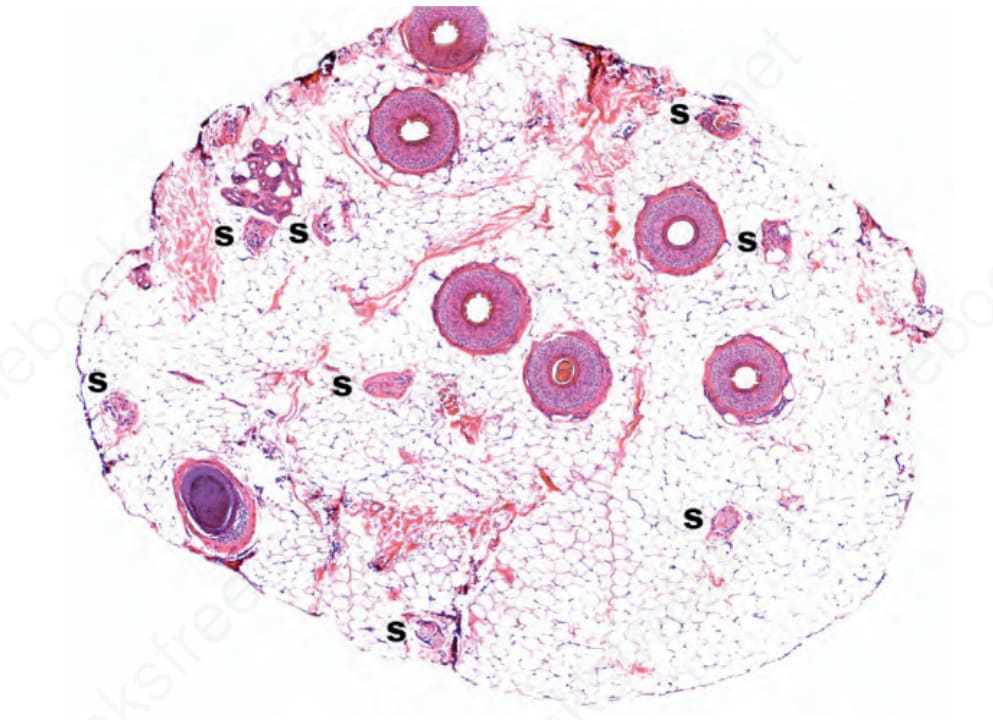
圖 22-48:雄性禿 (androgenetic alopecia),毛囊星狀殘跡 (follicular stellae);當毛囊經歷微小化時,它們留下大量的毛囊星狀殘跡 (S)。
Fig. 22.48 Androgenetic alopecia, follicular stellae; as the follicles undergo miniaturization they leave behind numerous follicular stellae (S).
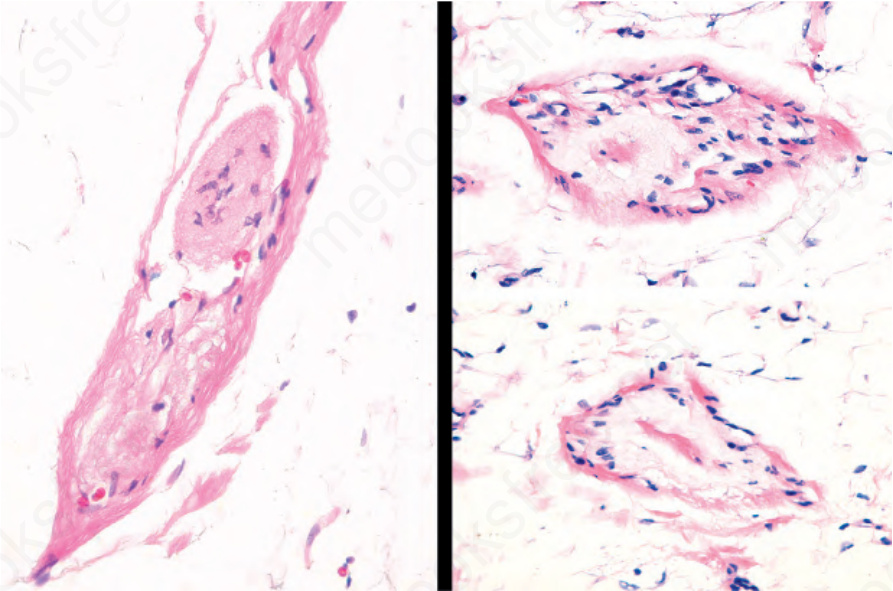
圖 22-49:Arao-Perkins bodies,於垂直(左)與水平(右)切面。注意沉積於毛囊星狀殘跡中心的膠原性與彈性變性物質。
Fig. 22.49 Arao-Perkins bodies, in vertical (left) and horizontal (right) sections. Note the collagenous and elastotic material deposited in the center of the follicular stellae.
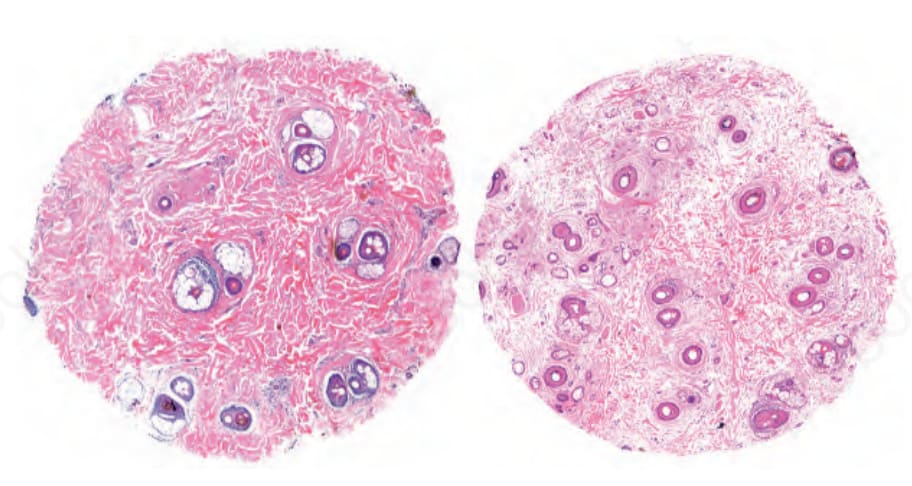
圖 22-50:雄性禿 (androgenetic alopecia),最終階段:毛囊單位與微小化毛囊罕見。在此晚期階段,結締組織幾乎完全取代了毛囊結構,外觀類似瘢痕性禿髮 (scarring alopecia)。在右側切面上部,可觀察到汗管類似汗管瘤 (syringoma-like) 的增生。
Fig. 22.50 Androgenetic alopecia, final stage: follicular units and miniaturized hair follicles are rare. In this advanced stage, connective tissue has almost completely replaced follicular structures and the appearance resembles a scarring alopecia. In the section on the right, upper part, a syringoma-like proliferation of sweat ducts is observed.
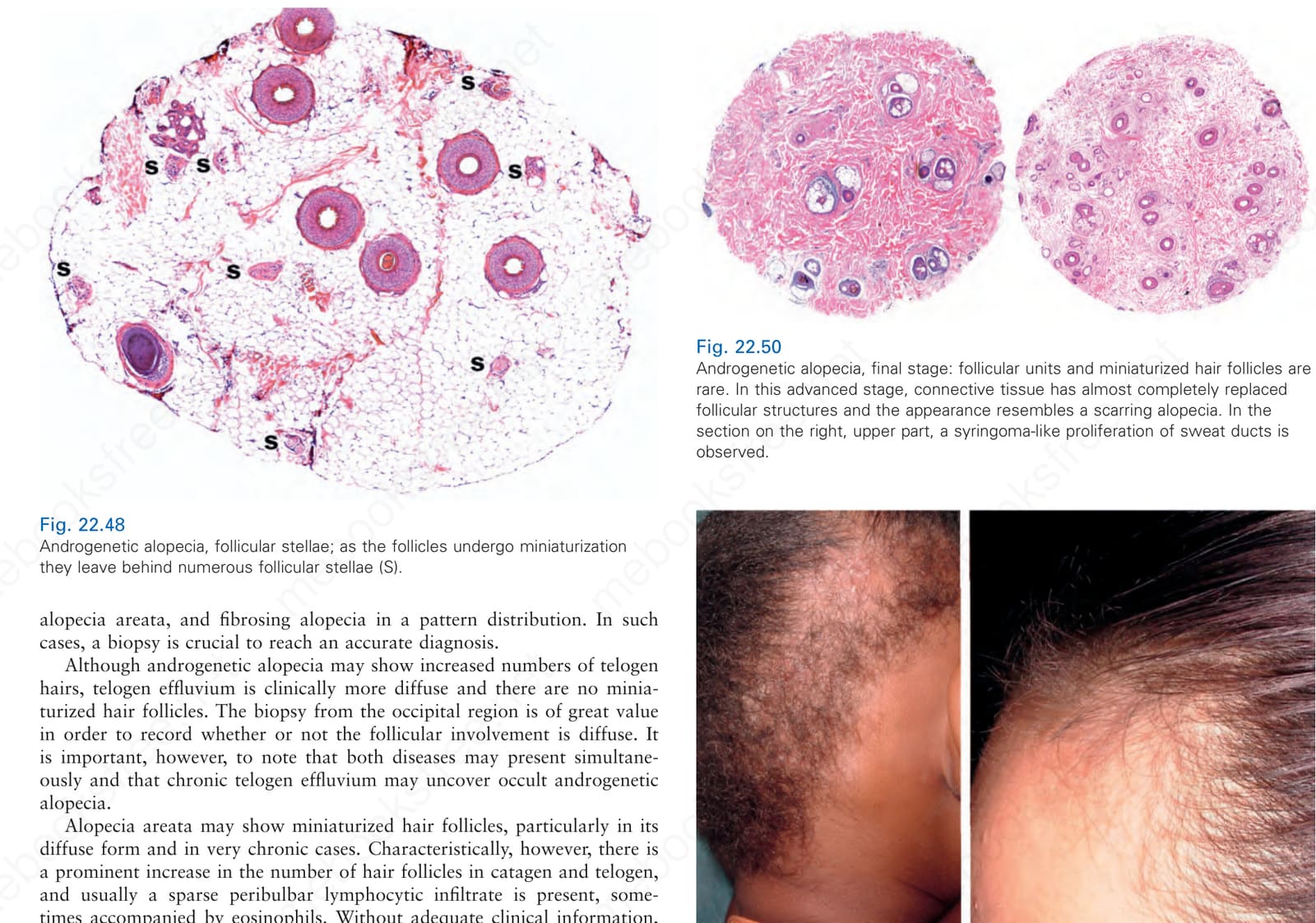
圖 22-51:牽引性禿髮 (traction alopecia)、蛇行狀禿髮 (ophiasis) 與額部纖維化禿髮 (frontal fibrosing alopecia) 之落髮型態。左側具蛇行狀 (ophiasis) 型態的病人也合併有疊加的癬 (tinea)。Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
Fig. 22.51 Traction alopecia, ophiasis and frontal fibrosing alopecia pattern of hair loss. The patient on the left with the ophiasis pattern also has a superimposed tinea. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.