Androgenetic alopecia
Androgenetic alopecia
Clinical features Androgenetic alopecia is also known as common baldness and male and female pattern hair loss.1 It is caused by androgens in genetically susceptible men, the role of androgens being less clear in women.1,2 Typically, there is progressive miniaturization of hairs in the scalp between the ages of 12 and 40 years.
Androgens are the main regulator of normal human hair growth. After puberty, they promote transformation of vellus hair follicles into large pigmented terminal hairs. However, androgens may also reverse this process, resulting in the gradual replacement of terminal hairs with vellus hairs and the onset of androgenetic alopecia.3
Androgenetic alopecia is a very common disorder and is the most frequent type of hair loss in adults, affecting at least 50% of the male population by the age of 50, and about 40% of the female population by the age of 70.4,5 The prevalence of vertex and full-blown androgenetic alopecia increases with age in males between 40 and 70 years, but the proportion of males with disease restricted to the frontal region remains fairly constant.6
Patients with androgenetic alopecia usually have a familial history of baldness. The absence of such a history reduces the risk but does not exclude the possibility of developing the condition. Rarely, it is associated with hyperandrogenism, and this is accompanied by other manifestations of excess androgens.7,8
In males, the condition usually starts early after puberty, mainly affecting the crown, vertex, frontal, central, and temporal areas of the scalp. There is usually no involvement of the occipital and lower parietal regions (Fig. 22.35). Some cases present in adolescence and in childhood, usually associated with a strong genetic predisposition.9,10 It has been proposed that patients who develop hair loss before the end of the third decade may have a higher risk of coronary artery disease than nonaffected males.11 However, other studies have restricted such association to alopecia localized to the vertex and some authors have totally discarded this association.12–14
An association with insulin resistance-linked diseases and with higher mortality for diabetes and cardiovascular disease has been noted in older patients with androgenetic alopecia.15,16
The condition also appears to be a risk factor for prostate cancer and benign prostatic hyperplasia.17–19
1066 Diseases of the hair
A
Dermoscopy and videodermoscopy of hair and scalp show important differences in hair shaft diameter, with a mixture of indeterminate and terminal hairs. Its use has enabled both the clinical diagnosis and the monitoring of the response to treatment to be more accurate. The site most affected by the alopecia is easily located and consequently will be the best site to biopsy (see Figs 22.35–22.37).31–33
Men suffering from androgenetic alopecia do not usually require laboratory investigations. The decision to perform laboratory tests in affected females depends on a variety of factors including family history, clinical presentation, evolution, and age at onset of the disease. A woman with menstrual irregularities, a history of infertility, polycystic ovaries, or physical signs suggesting hyperandrogenism (hirsutism, cystic acne unresponsive to treatment, acanthosis nigricans, virilization, or galactorrhea) should have further investigations including free and total testosterone levels. If these are high the source should be determined, especially with respect to the presence of an ovarian tumor or adrenal hyperplasia. In women with androgenetic alopecia without a family history or physical signs suggestive of hyperandrogenism, it is not usually necessary to perform any laboratory tests.30
B
In androgenetic alopecia, a gentle hair pull is normal. Only a few hairs are obtained, and these are all in telogen phase. Hair pluck can give misleading results due to an apparent higher count of hair in telogen in the affected areas. This occurs because, in the early stages, hair follicles more frequently enter telogen as a result of shortening of the anagen phase. Confusion with telogen effluvium is possible but distinction is easy, based on the fact that telogen effluvium is generalized and androgenetic alopecia is localized.
it develops much earlier (Fig. 22.37). Female pattern hair loss has been associated with hyperprolactinemia.26
The two patterns of hair loss in androgenetic alopecia are sometimes known as Hamilton-Norwood ‘male pattern’ and Ludwig ‘female pattern’ (Fig. 22.38).27,28 However, there is considerable overlap. Some women present with male pattern and vice versa. Korean men tend to have a more ‘female pattern’ of hair thinning than Caucasians.29 These types of inverse presentation do not define the hormonal state of the individual; a woman with a masculine pattern of alopecia does not necessarily present with hyperandrogenism.
The different clinical presentations and the fact that the occipital scalp is generally respected is a consequence of the different embryological origins of the dermis in the different areas of the scalp. The dermis of the frontal/ parietal scalp is of neural crest origin, whereas the dermis of the occipital scalp is of mesodermal origin.30
Pathogenesis and histologic features Androgenetic alopecia results from a progressive decrease in the size of hair follicles and their transformation into vellus forms (Fig. 22.39 and see Figs 22.12 and 22.14). However, it has also been observed that this miniaturization may occur suddenly within only a few cycles.34 This phenomenon is the direct result of 5α-reductase type II activity, which is mainly found in the external root sheath and the hair bulb papilla. The enzyme converts testosterone into dihydrotestosterone, which has a great affinity for the androgen receptors in the outer root sheath and follicular papilla of the hair follicle.35 The hormone receptor complex activates the genes responsible for the gradual transformation of large terminal hairs into miniaturized hair follicles. Young women and men with this condition have higher levels of 5α-reductase and androgen receptor in frontal hair follicles when compared with occipital follicles.34 Finasteride inhibits 5α-reductase type-2 isozyme, lowering the levels of dihydrotestosterone and promoting hair growth in men.
However, the role of androgens in the female pattern hair loss variant is not fully established. Scalp hair loss is a feature of hyperandrogenism in females but many women with female pattern hair loss have no other clinical or biochemical evidence of androgen excess. Female pattern hair loss is probably a multifactorial, genetically determined trait and it is possible that both androgen-dependent and androgen-independent mechanisms contribute to the phenotype.36–38 Other enzymes that modulate the effect of the androgens and estrogens and serve as protecting factors against androgenetic alopecia are cytochrome p450 aromatase and 17β-hydroxysteroid dehydrogenase. These lead to increase in the level of local estrogen in the hair follicle with variations in relation to sex, age, and location of the hair follicles. 39
1067 Nonscarring alopecias
In both, male and female pattern hair loss there is a decline in anagen duration, increase in the percentage of hair follicles in telogen, and a higher frequency and prolongation of the kenogen phase, particularly in cases of high miniaturization of the hair follicles. It would seem that the telogen hair follicle follows an alternative route, one not followed by a new early anagen phase but rather remaining for a prolonged period as an empty follicle. The final result is nonpigmented hair shafts, which progressively become thinner and smaller, and this finally results in empty follicles without stems (teloptosis). Some follicles could fade away and be replaced by fibrous tracts.40–42
For the microscopic study of androgenetic alopecia, two 4-mm punch biopsies should be obtained: a control from healthy scalp in the occipital region and the other from the affected area. Both biopsies must be sectioned horizontally from the lower part of the infundibulum for comparative quantification purposes. The ratio between terminal and vellus hairs is approximately 7 : 1. A ratio of 4 : 1 or less is suggestive of androgenetic alopecia.
The histologic features are different in the early and late stages of the disease. Terminal, indeterminate, and vellus hairs should be counted. It is easier to appreciate the miniaturization of hair follicles and dropping out of follicular units when a comparison is made with the biopsy of normal scalp taken from the occipital area (Fig. 22.40). This process does not present in a uniform manner as initially it can be focal and may even only affect some of the follicles within a follicular unit (Fig. 22.41). A toluidine blue stain is particularly useful to highlight the outer and inner root sheaths in contrast to the pale staining of the hair shaft (Fig. 22.42 and see Fig. 22.15).43,44
Histologically, terminal hairs progressively transform to vellus hairs (Figs 22.43 and 22.44). There is a decrease in the size of the dermal papilla and bulb.34 The diameter of the hair shaft also decreases and varies noticeably from one follicle to another. This histologic feature is closely related to the miniaturization observed clinically (Fig. 22.45).45
Although the total hair count is normal, it will appear reduced if the count is taken at the junction of the dermis and subcutaneous fat, since by definition terminal hairs are diminished in number. Even though these changes may also be seen in vertical sections (see Fig. 22.39), they are more difficult to interpret and quantify.
Along with these changes, there is a reduction in the duration of the hair follicle cycle at the expense of the anagen phase. Therefore, in patients with evolving or fully established androgenetic alopecia, it is very common to find an increment in the number of catagen and telogen follicles in the miniaturized follicles component. 46 The histologic picture of the female variant is identical.
A mild to moderate T lymphocytic inflammatory cell infiltrate frequently surrounds the upper third of the hair follicle, associated with discrete perifollicular concentric fibrosis particularly in patients of African descent (Fig. 22.46 and see Fig. 22.17).47,48 The significance of this phenomenon has yet to be ascertained as, unlike primary scarring alopecias, there is no loss of hair follicle stem cells. However, there does seem to be a decrease in the conversion of stem cells to progenitor cells.49
The miniaturization of hair follicles affects the whole of the hair follicle including, in late stages, the arrector pili muscle and the sebaceous gland. The degeneration and replacement of the arrector pili muscle by fat tissue and the loss of contact with the bulge occurring in the miniaturized follicle seems to be a critical factor in defining whether an androgenetic alopecia will respond to treatment. The persistence of the union between these two structures is a sign of the reversibility in alopecia as it appears to protect the integrity of the stem cells in the bulge even in the advanced stages of
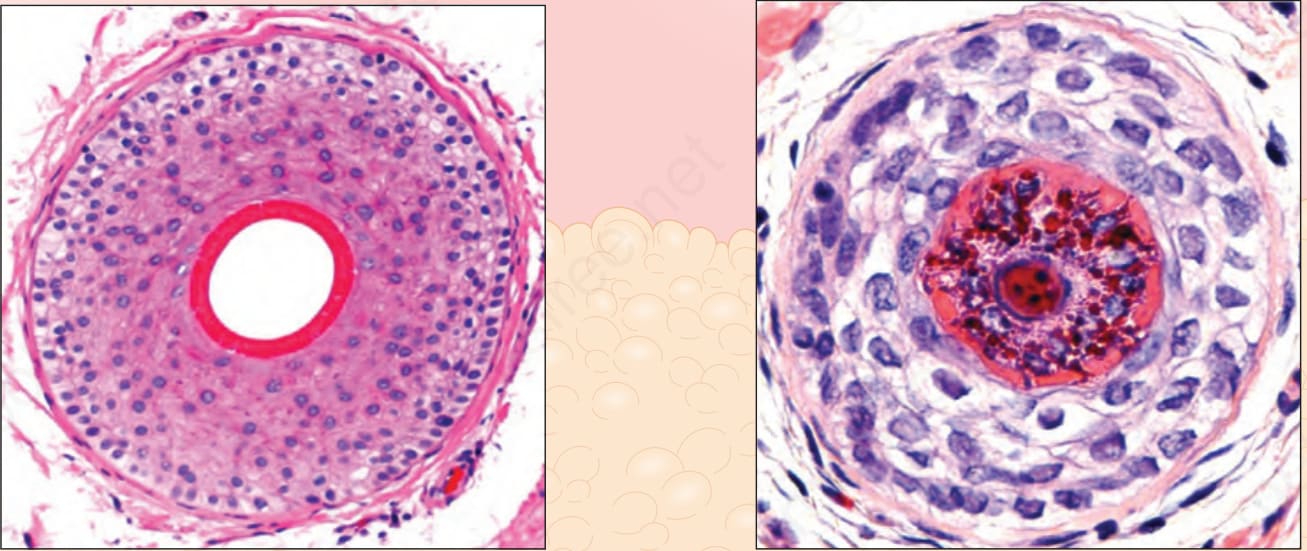
Fig. 22.12 Terminal anagen and vellus hair, vertical and horizontal sections: the terminal hair follicles reach the fat and are deeply embedded within it. The vellus hairs and miniaturized follicles are located within the dermis. Note the differences between the relative size of the hair shaft and the inner root sheath in terminal and vellus hairs. Courtesy of M. Mejia, MD, Universidad Pontificia Bolivariana, Medellín, Colombia.
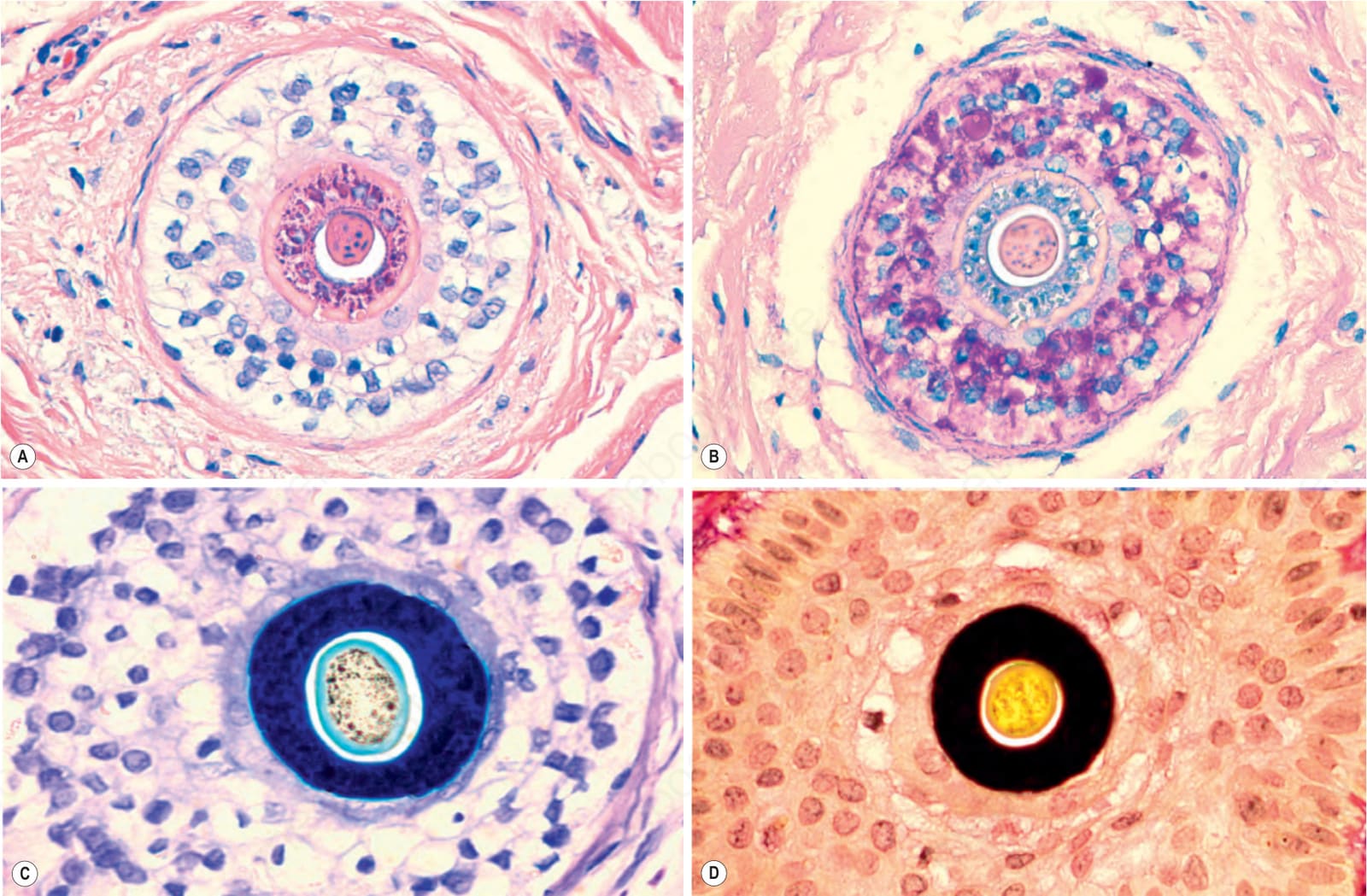
Fig. 22.15 Vellus hair, horizontal section: note the caliber of the hair shaft compared to the inner root sheath in: (A) pink, hematoxylin and eosin; (B) gray, PAS; (C) blue, toluidine blue; and (D) black, elastic tissue stain.
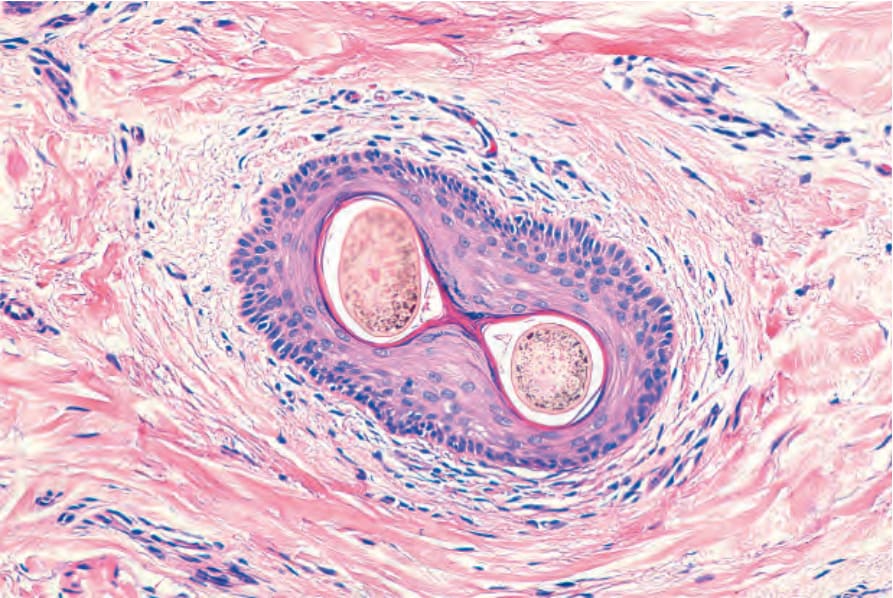
Fig. 22.17 Infundibulum. Horizontal section. The wall is made up of squamous stratified keratinized epithelium. The surrounding dermis is infiltrated by some lymphocytes. There are two hair shafts emerging from a single ostium.

Fig. 22.35 Male androgenetic alopecia: this patient shows well-established male pattern baldness with bifrontal hair line recession and hair loss on the scalp vertex. In the dermoscopic image on the right, note the difference in caliber between hair follicles. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
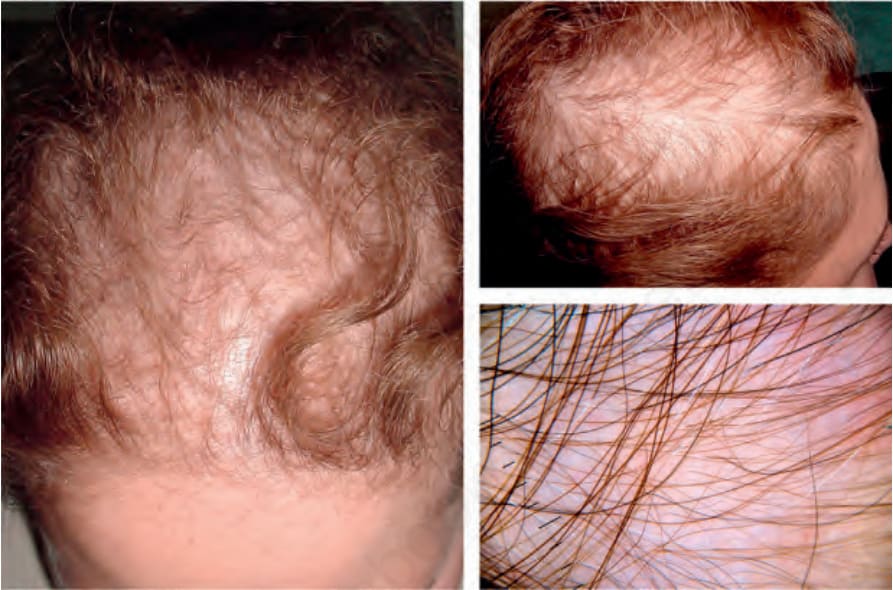
Fig. 22.36 Female pattern hair loss: this example shows a typical example with parietal and posterior frontal hair loss. Note the sparing of the frontal hairline. In the dermoscopic image on the right lower panel, note the hair loss due to extensive miniaturization on a noninflammatory background. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.

Fig. 22.37 Female pattern hair loss in a girl: early hair loss is observed with widening of the interparietal line. In the dermoscopic image on the right lower panel, note a tendency to miniaturization with hair follicles of different calibers. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.
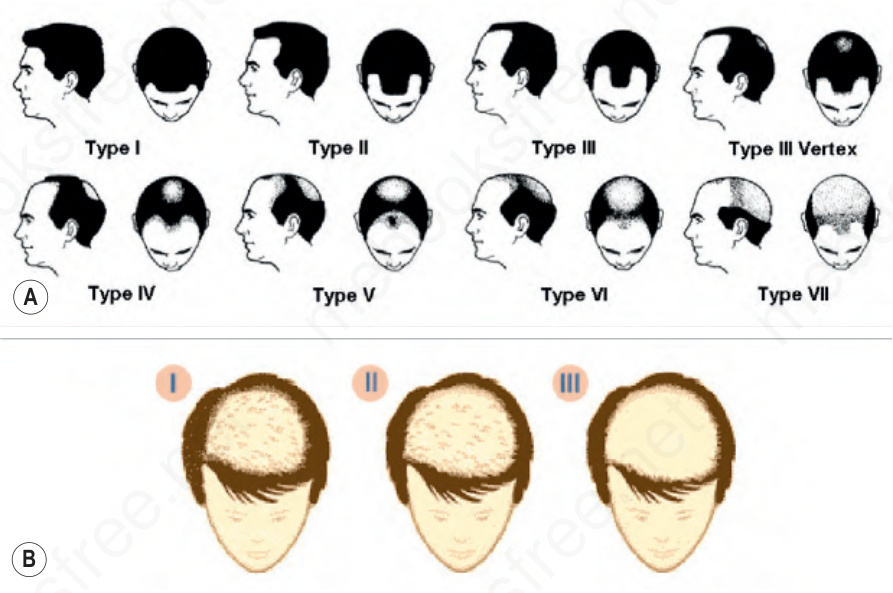
Fig. 22.38 (A) Hamilton-Norwood classification of male pattern androgenetic alopecia (top). Reproduced with permission from Norwood, O.T. (1984) Hair transplant surgery. Springfield: Charles C. Thomas, p 6. (B) Ludwig patterns of female pattern hair loss (bottom). Reproduced with permission from Ludwig, E. (1977) Classification of the types of androgenetic alopecia occurring in the female sex. British Journal of Dermatology, 97;247–254.
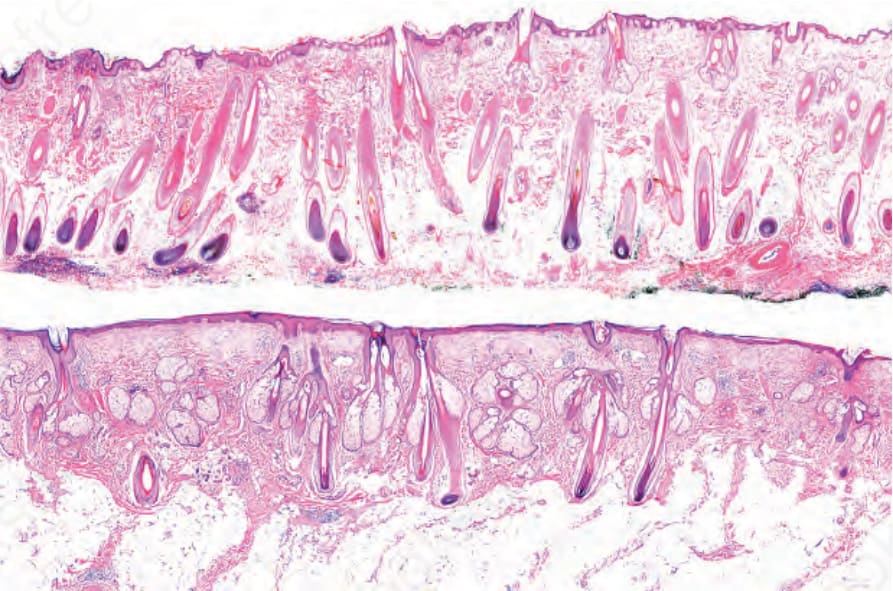
Fig. 22.39 Androgenetic alopecia. Vertical sections. In the top panel normal scalp with numerous terminal hair follicles extending into the deep subcutaneous fat. In the lower panel, note a scalp biopsy from a patient with advanced androgenic alopecia. Barely visible, are a few thin follicles which only just reach the limit between the dermis and the subcutaneous tissue.
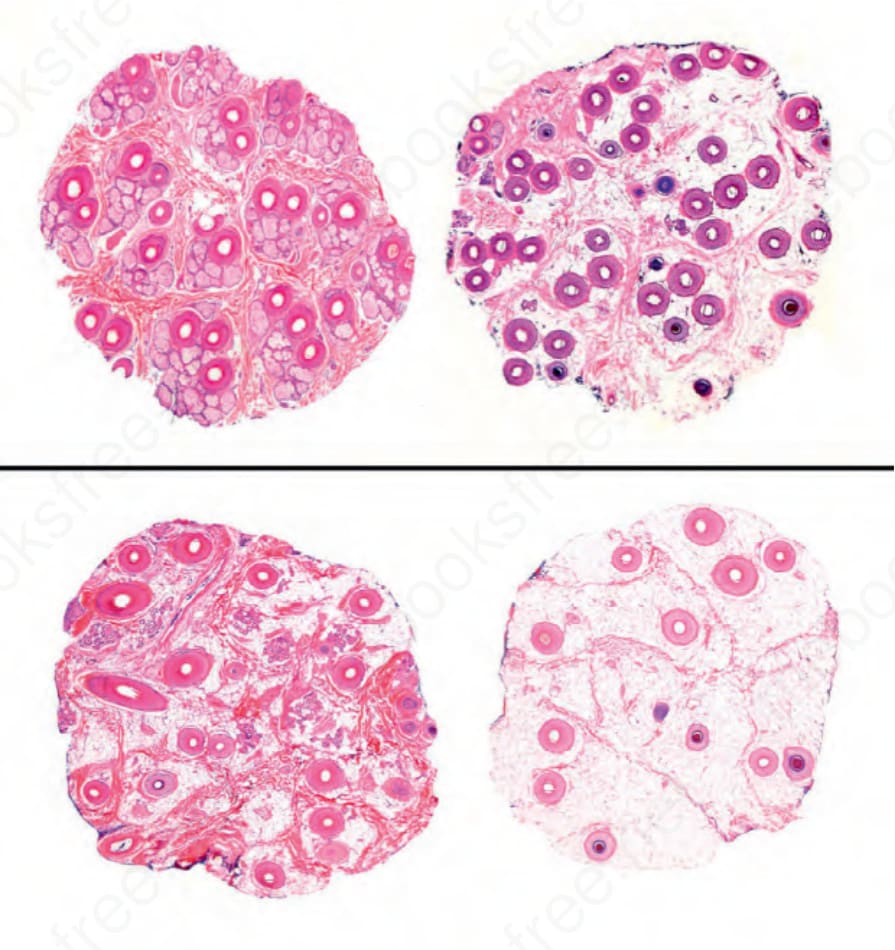
Fig. 22.40 Androgenetic alopecia, horizontal sections: in the upper panel, a biopsy of normal scalp taken from the occipital area. There are numerous follicular units formed by follicles of uniform size. Below are sections from an area of frontal alopecia with more than half of the follicles miniaturized (vellus) or in the process of miniaturization. The follicular units have disappeared and in the subcutaneous fat there are numerous stellae.
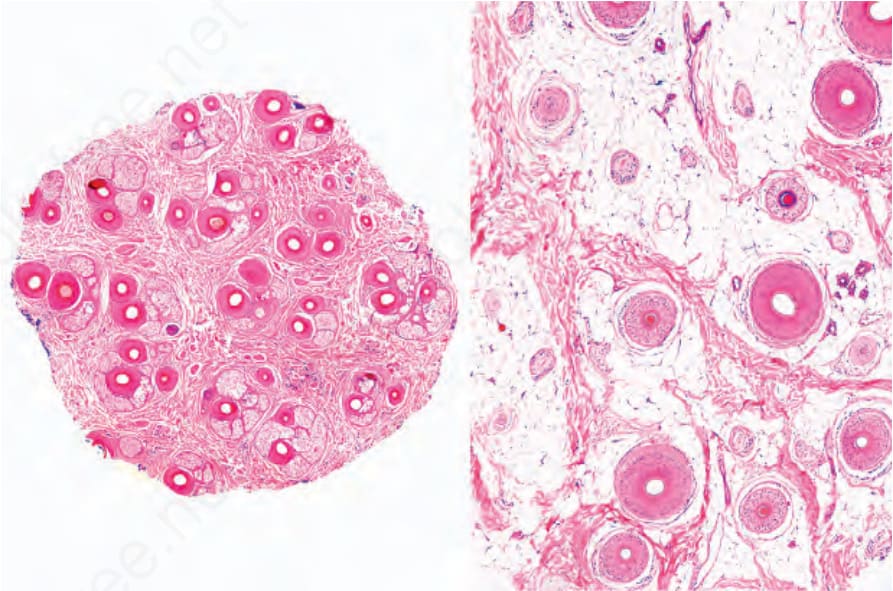
Fig. 22.41 Androgenetic alopecia, horizontal sections. This image highlights how the miniaturization phenomenon is not uniform but affects focal areas leaving normal areas in between. A section at a deeper level is shown in the right panel.
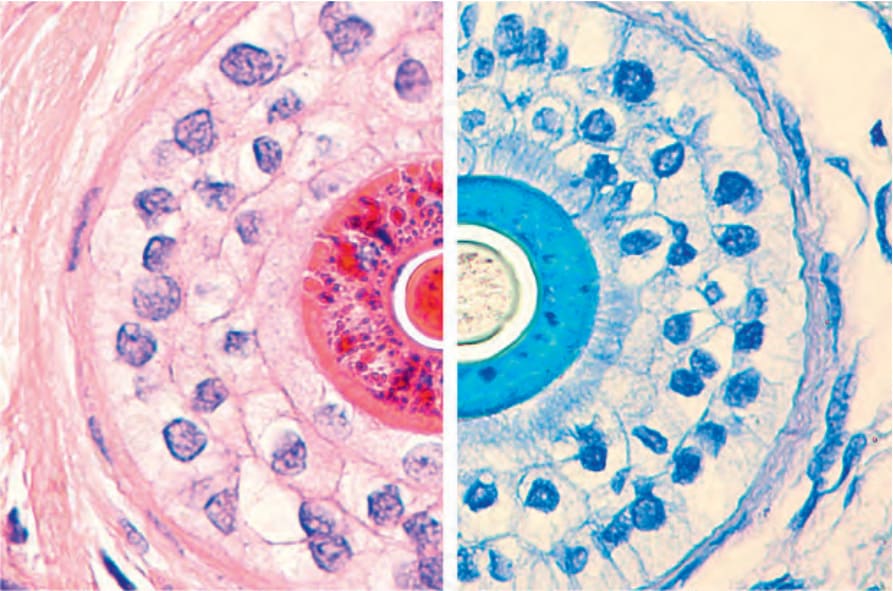
Fig. 22.42 Miniaturized hair follicle. Compare the staining of the inner root sheath on the left (red with hematoxylin and eosin) with the one on the right (blue with toluidine blue).
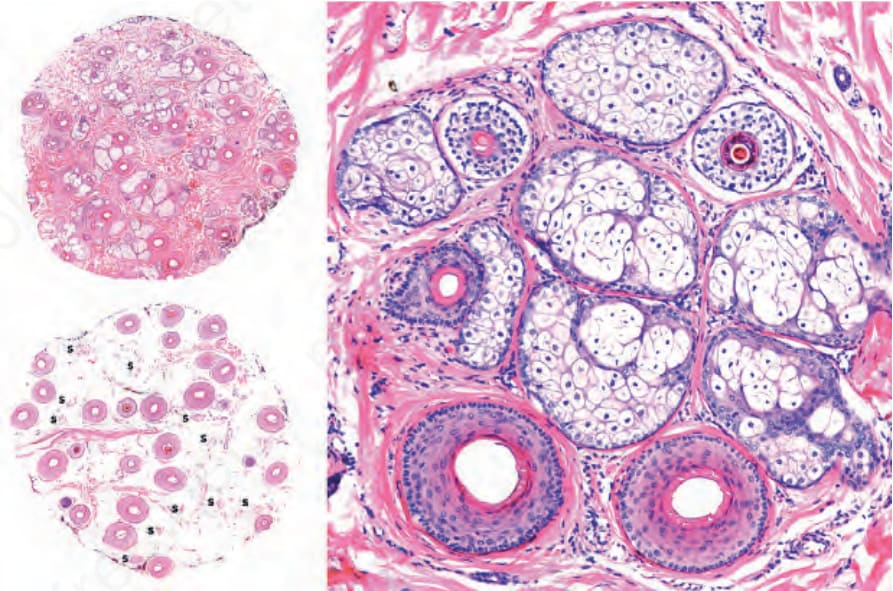
Fig. 22.43 Androgenetic alopecia, horizontal sections: (left) this is a scalp biopsy taken from the interparietal area. In the superficial section (top), there are numerous miniaturized hair follicles. In the section at the level of the subcutaneous tissue (bottom), many of the follicles have been replaced by follicular stellae (S); (right) follicular units with two terminal follicles at the bottom and three miniaturized follicles at the top.
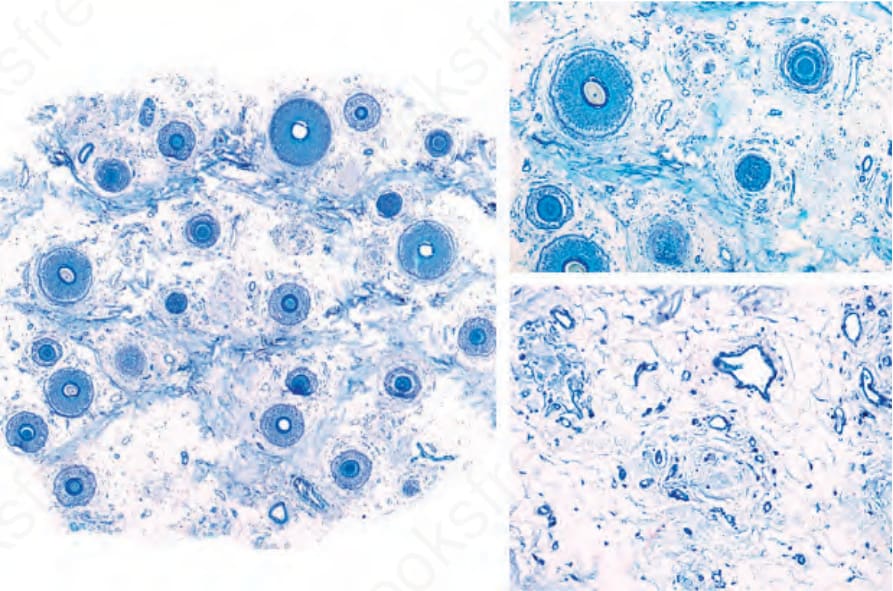
Fig. 22.44 Androgenetic alopecia: in this more advanced example, the follicular density is greatly reduced with many miniaturized hair follicles (left) and numerous stellae (right). Toluidine blue stain.
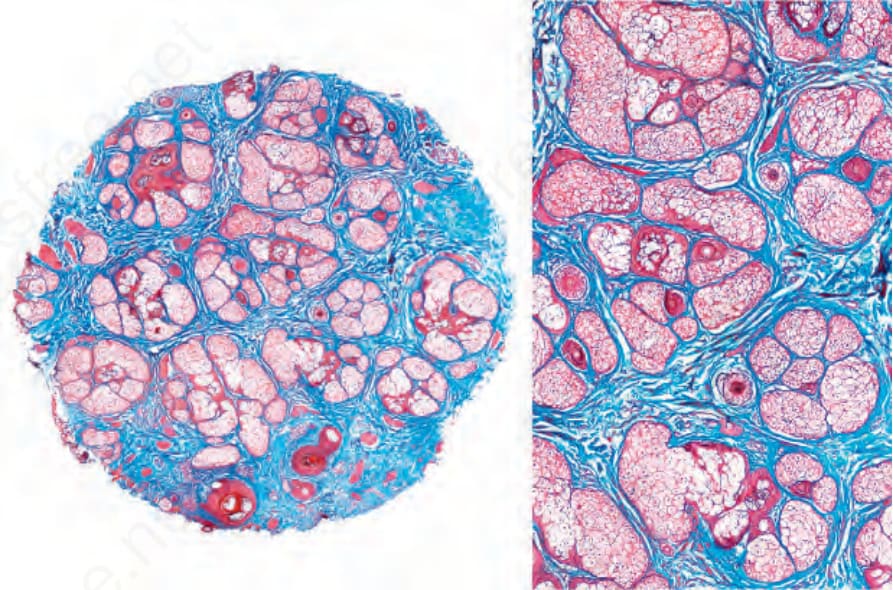
Fig. 22.45 Androgenetic alopecia: almost all hair follicles are miniaturized and the sebaceous glands appear prominent. The hair shafts are barely visible. Masson trichrome stain.
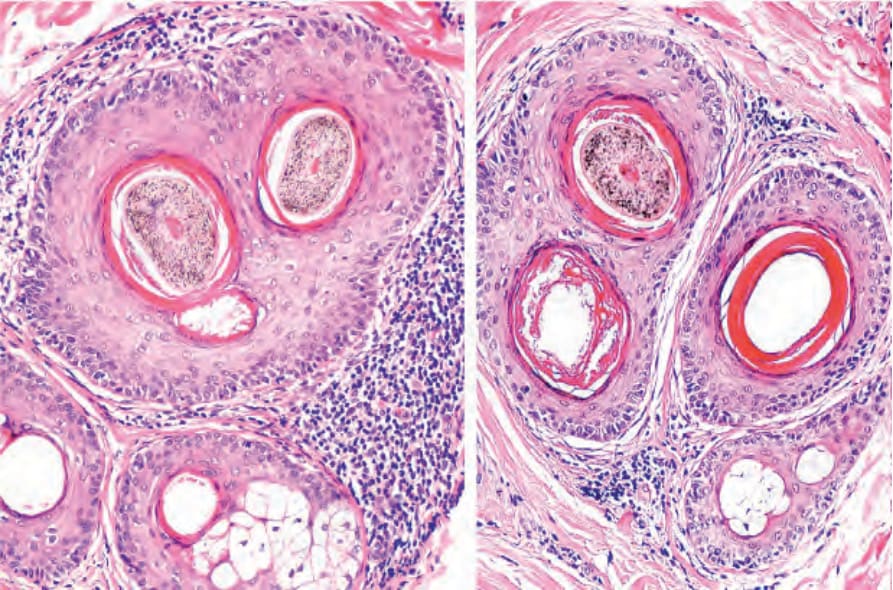
Fig. 22.46 Compound hair infundibulum surrounded by a lymphocytic infiltrate and mild concentric fibrosis in a patient with androgenetic alopecia.
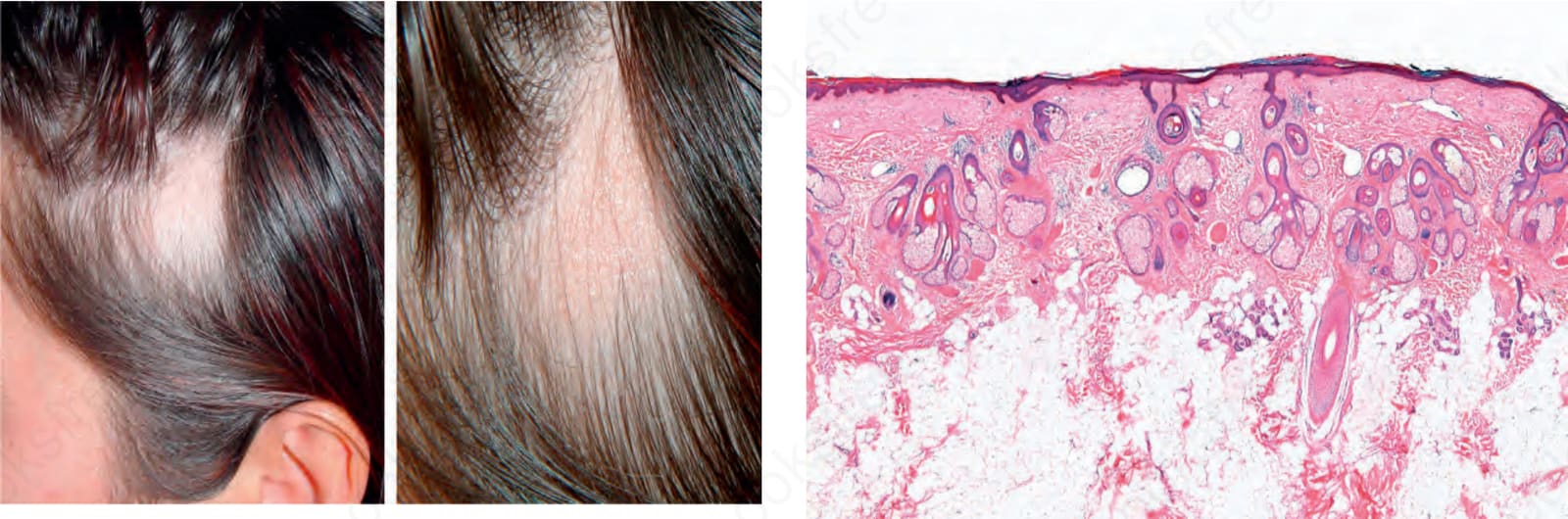
Fig. 22.52 Triangular alopecia: note the characteristic triangular patch of alopecia. In the right panel, a close-up view shows absence of inflammatory changes. Courtesy of A.M. Aristizábal, MD, CES, Medellín, Colombia.
the process.50 The sebaceous glands remain normal, but in androgenetic alopecias of long evolution hyperplasia of the eccrine glands may be observed and sometimes form syringoma-like structures (Fig. 22.47).51,52
In deeper sections, hair bulbs are present at different depths, and they may be completely absent focally, with only follicular stellae remaining. These stellae are seen in a variety of conditions and reflect either miniaturized
1068 Diseases of the hair
follicles or else follicles that have entered catagen or telogen stage (Fig. 22.48). As the stellae mature, they become less vascularized, presenting as fibrous scars with a blue-gray hue, which corresponds to condensations of elastic tissue known as Arao-Perkins bodies (Fig. 22.49).53,54 In late androgenic alopecia, the stellae become abnormally thick and could impede the growth of the follicle.
The terminal/vellus hair ratio (7 : 1) is much reduced and varies from 1 : 1 or even 1 : 2. Although initially the number of hair follicles is normal, in longstanding disease there can be a real reduction. A biopsy may therefore show a decrease in hair follicle density in addition to diminution in size of the individual hair follicles. Sometimes the appearances may be more suggestive of a scarring alopecia (Fig. 22.50).
Differential diagnosis The most important differential diagnosis is with diseases which present with diffuse nonscarring alopecia including chronic telogen effluvium,
1069 Nonscarring alopecias
alopecia areata, and fibrosing alopecia in a pattern distribution. In such cases, a biopsy is crucial to reach an accurate diagnosis.
Although androgenetic alopecia may show increased numbers of telogen hairs, telogen effluvium is clinically more diffuse and there are no miniaturized hair follicles. The biopsy from the occipital region is of great value in order to record whether or not the follicular involvement is diffuse. It is important, however, to note that both diseases may present simultaneously and that chronic telogen effluvium may uncover occult androgenetic alopecia.
Alopecia areata may show miniaturized hair follicles, particularly in its diffuse form and in very chronic cases. Characteristically, however, there is a prominent increase in the number of hair follicles in catagen and telogen, and usually a sparse peribulbar lymphocytic infiltrate is present, sometimes accompanied by eosinophils. Without adequate clinical information, however, distinction may be impossible.
In fibrosing alopecia in pattern distribution (Fig. 22.51) the lymphocytic inflammatory cell infiltrate affects the infundibulum and the follicular isthmus and there is epithelial and bulge cell destruction. Additionally,
1070 Diseases of the hair
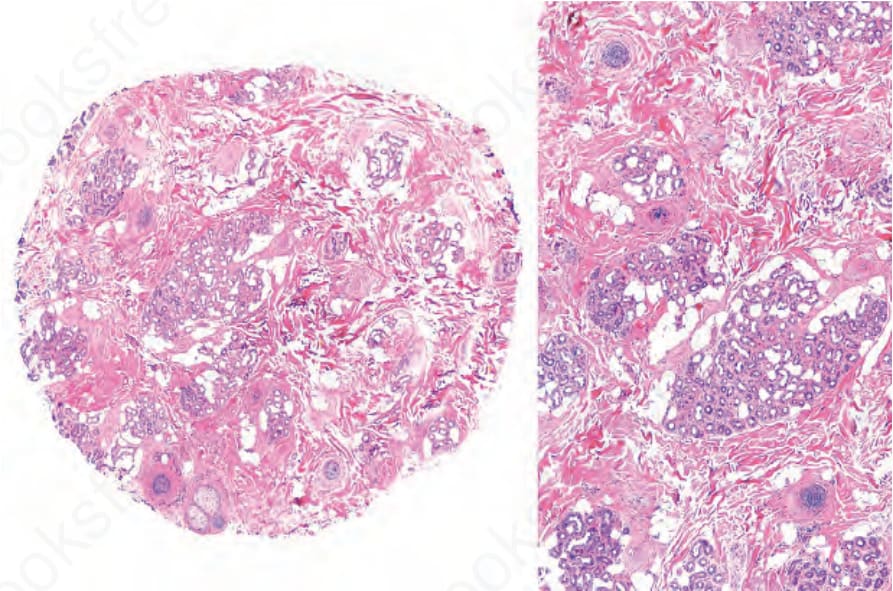
Fig. 22.47 Sweat gland duct proliferation. Case of advanced androgenetic alopecia with follicular structures replaced by lobules of hyperplastic sweat glands and ducts.
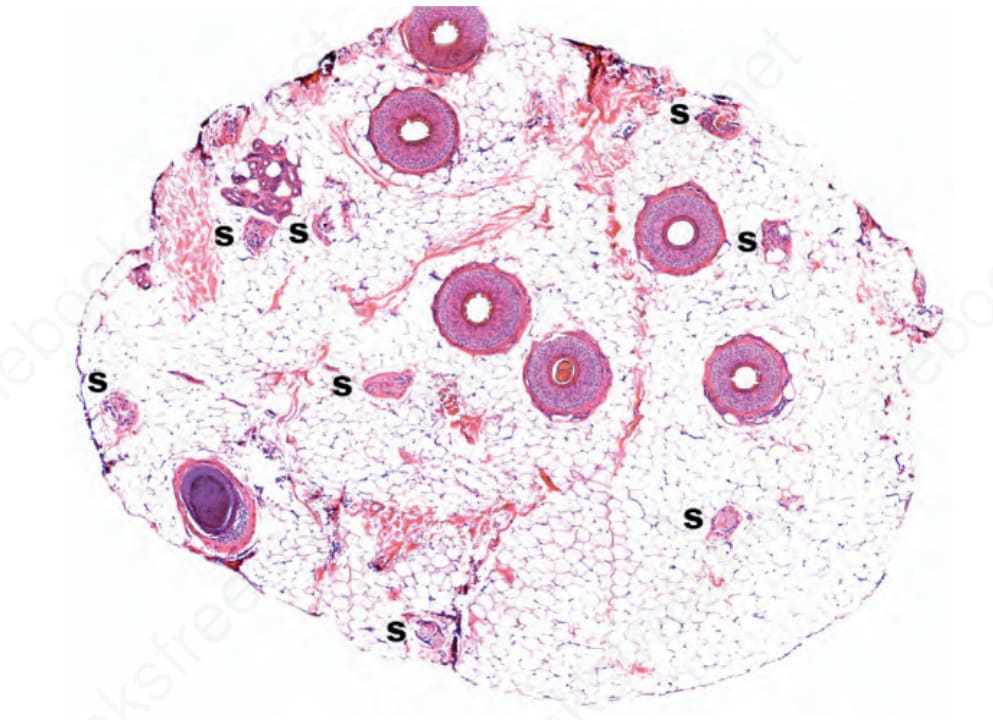
Fig. 22.48 Androgenetic alopecia, follicular stellae; as the follicles undergo miniaturization they leave behind numerous follicular stellae (S).
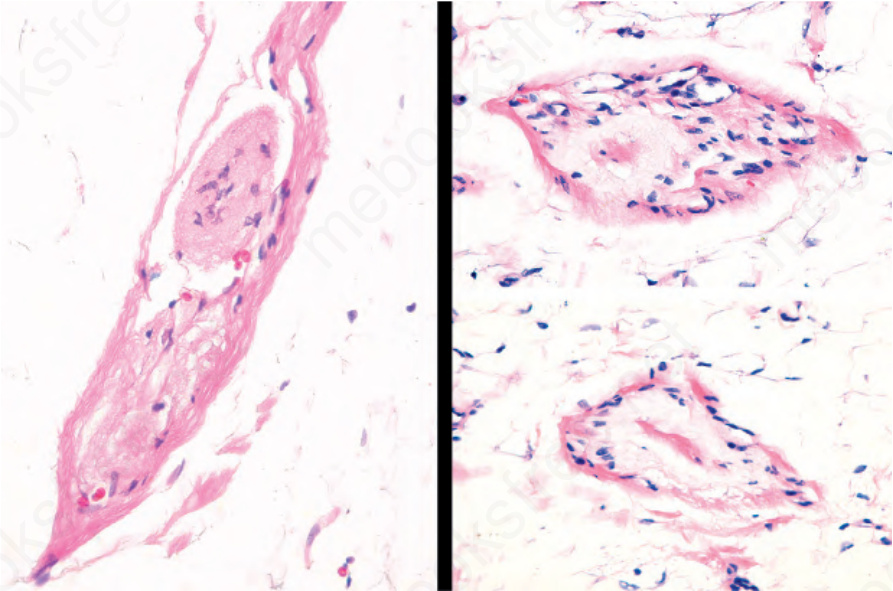
Fig. 22.49 Arao-Perkins bodies, in vertical (left) and horizontal (right) sections. Note the collagenous and elastotic material deposited in the center of the follicular stellae.
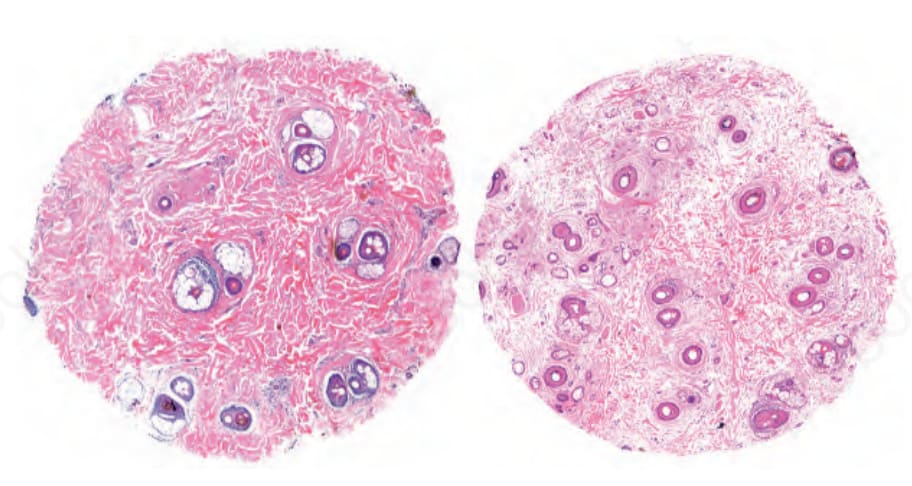
Fig. 22.50 Androgenetic alopecia, final stage: follicular units and miniaturized hair follicles are rare. In this advanced stage, connective tissue has almost completely replaced follicular structures and the appearance resembles a scarring alopecia. In the section on the right, upper part, a syringoma-like proliferation of sweat ducts is observed.
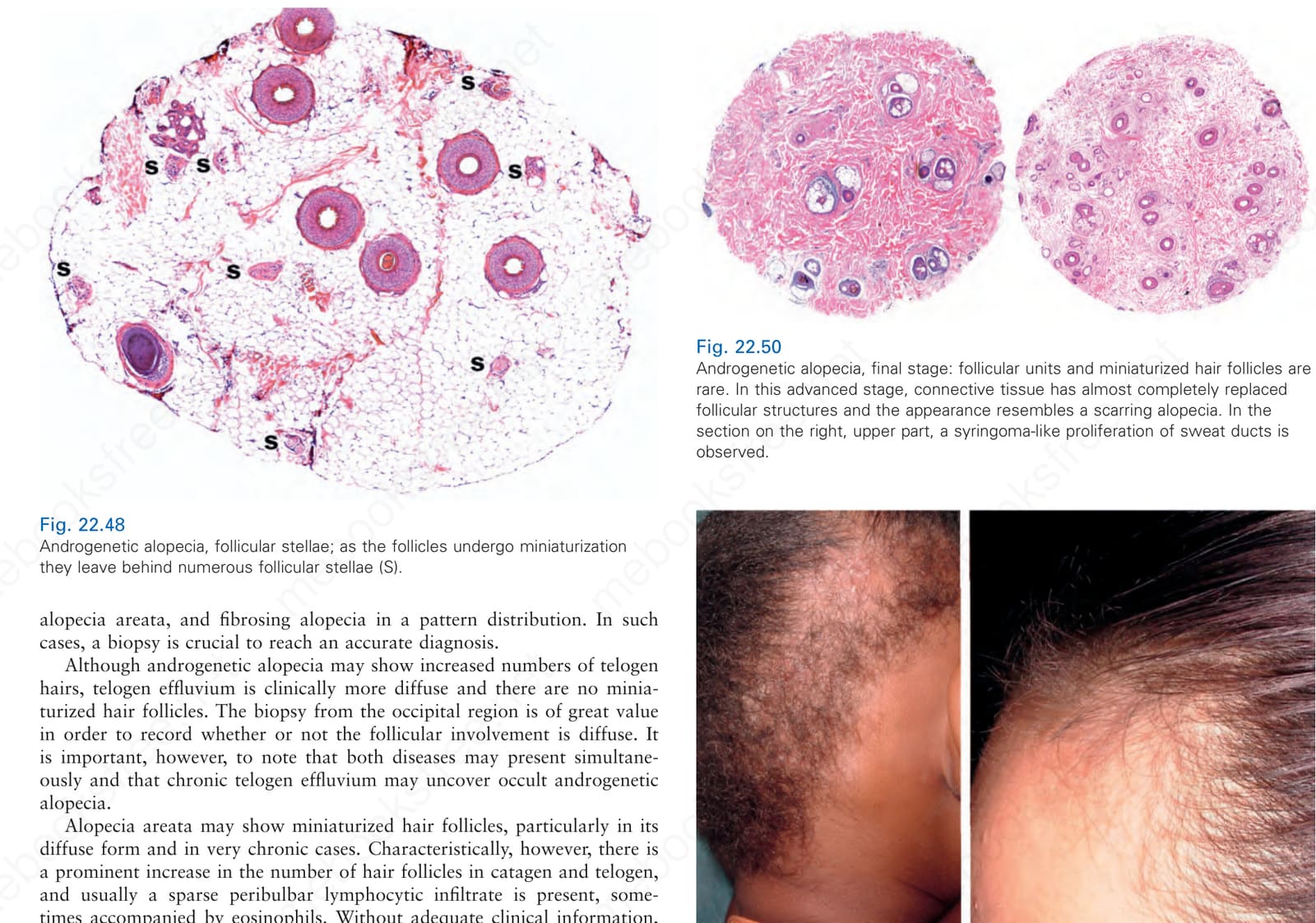
Fig. 22.51 Traction alopecia, ophiasis and frontal fibrosing alopecia pattern of hair loss. The patient on the left with the ophiasis pattern also has a superimposed tinea. Courtesy of L.M. Gómez, MD, UPB, Medellín, Colombia.