臨床特徵 (Clinical Features)
-
Actinomyces israelii 是人類口腔內的共生菌 (commensal),與其他菌種共存,包括 Aggregatibacter(舊稱 Actinobacillus)actinomycetemcomitans。A. israelii 是常見的致病菌,但偶爾也牽涉其他菌種,包括 A. viscosus、A. naeslundii、A. odontolyticus、A. meyeri、A. turicensis、A. radingae 與 A. neuii。
-
最常見的表現是頸顏面放線菌病 (cervicofacial actinomycosis),但也可能發生較嚴重的肺部與腸道感染,並且罕見地出現純皮膚病灶。
-
頸顏面型常見於農場工作者,並與口腔衛生不良有關,通常起源於齲齒,發生於拔牙或口腔創傷之後。此病在兒童少見,最常見於年輕男性。
-
呼吸道侵犯表現為肺膿瘍 (lung abscess) 與瘻管 (fistulae),可能「穿出」胸壁 (Fig. 18.228)。腹部病灶包括闌尾與結腸放線菌病以及肝臟侵犯,並可能使子宮內避孕器 (intrauterine contraceptive devices) 的使用變得複雜,病灶可侵犯女性內生殖器。其後可能續發皮膚瘻管。
-
偶爾含有完整及部分被消化的細菌。有人推測巨噬細胞 (macrophages) 內的吞噬溶酶體 (phagolysosomes) 是對慢性細菌感染的反應而堆積的。此感染並非由單一特定微生物所致,但其病原通常為 E. coli。吞噬溶酶體傾向融合然後鈣化;這些變化的原因尚不清楚,雖然部分病例發生於與巨噬細胞功能可能受損相關的全身性疾病中。從 malakoplakia 病灶培養出的其他微生物包括革蘭氏陰性桿菌 (Gram-negative bacilli)(Klebsiella spp.、Enterobacter spp.、Proteus spp.、Pseudomonas spp.、Burkholderia cepacia complex)與革蘭氏陽性球菌 (Gram-positive cocci),包括 Staphylococcus aureus、Streptococcus spp. 與 enterococci。
-
頸顏面病灶表現為下顎的硬性腫脹,或偶爾表現為自上顎延伸至臉頰的斑塊樣浸潤 (plaquelike infiltration)(對照牛的「lumpy jaw」)。這些堅實增厚的區域傾向經由竇道 (sinuses) 排出,並伴隨疤痕形成與新結節的生成 (Fig. 18.229)。在排出的膿液中偶爾可見直徑達 2 mm 的黃色顆粒——即所謂的「硫磺顆粒」(sulfur granules)。部分上顎病灶的延伸可能到達眼眶與顱底。少見地,可能發展出大型臉部腫塊。
鑑別診斷 (Differential Diagnosis)
-
Malakoplakia 應與感染性肉芽腫 (infectious granulomata)、組織球增生症 (histiocytosis) 與顆粒細胞瘤 (granular cell tumor) 區別,並與 pseudomalakoplakia 區別,後者指的是先前手術部位中異常的組織球增生 (histiocytic proliferation)。雖然 pseudomalakoplakia 同樣由含胞質內鈣化物質的大型組織球 (histiocytes) 片狀聚集所構成,但此病可藉由顆粒缺乏同心圓狀層狀構造 (concentric lamination) 而與真正的 malakoplakia 區別。
-
罕見地,皮膚的直接接種 (direct inoculation) 可能產生類似的慢性排膿膿瘍 (chronically discharging abscess),並伴隨鄰近疤痕 (Fig. 18.230)。或者,可能發展出足菌腫 (mycetoma) 或具多個竇道的慢性排膿膿瘍腫塊。此原發型皮膚放線菌病罕見。發生部位包括大腿、股臀區 (femorogluteal region)、手臂、陰莖、乳房、頸部、鼻部與前額。多數病例是外部創傷與局部缺血 (local ischemia) 的結果,但並非總是如此。有些感染是經由注射傷口取得,包括一則報告:一名靜脈注射古柯鹼 (cocaine) 的使用者承認在注射前舔舐其皮下注射針頭,因而發展出 A. odontolyticus 相關的皮下膿瘍。極罕見地,原發性皮膚放線菌病可能是潛在 HIV 感染的表現徵象。另有一則單獨報告:一名罹患普通變異型免疫缺乏 (common variable immunodeficiency) 的病人,A. bovis 感染侵犯其指甲。
910 Infectious diseases of the skin
- 此病有一種不常見的型態,是在缺乏可證實的皮膚外感染情況下,出現播散性皮膚病灶;此情形曾在一名急性白血病 (acute leukemia) 病人身上被報告。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- 放線菌病所牽涉的微生物混合並非純屬偶然,而是具有協同作用 (synergistic)。A. israelii 是一種革蘭氏陽性 (Gram-positive)、非抗酸性 (nonacid-fast)、微需氧 (microaerophilic) 的細菌,具有絲狀分枝 (filamentous branching) 的形態。A. actinomycetemcomitans 是一種革蘭氏陰性的球桿菌 (coccobacillus),會抑制纖維母細胞 (fibroblasts) 與角質細胞 (keratinocytes) 的生長。據推測,這一點連同其對抗生素的不同感受性,有助於維持放線菌病灶。
- 組織學上,病灶具有慢性膿瘍與竇道的特徵,含有膿液並被纖維化 (fibrosis) 與混合性發炎浸潤 (mixed inflammatory infiltrate) 所包圍 (Fig. 18.231)。可見由肉芽組織 (granulation tissue) 分隔的小腔室 (locules)。可見由交織細菌構成的硫磺顆粒 (sulfur granules)、放射狀的菌絲絲狀體 (radiating mycelial filaments),其末端常帶有不透明的棒狀構造 (opaque clubs) (Figs 18.232 及 18.233)。這些顆粒可能與 Splendore-Hoeppli 現象 (Splendore-Hoeppli phenomenon) 有關。
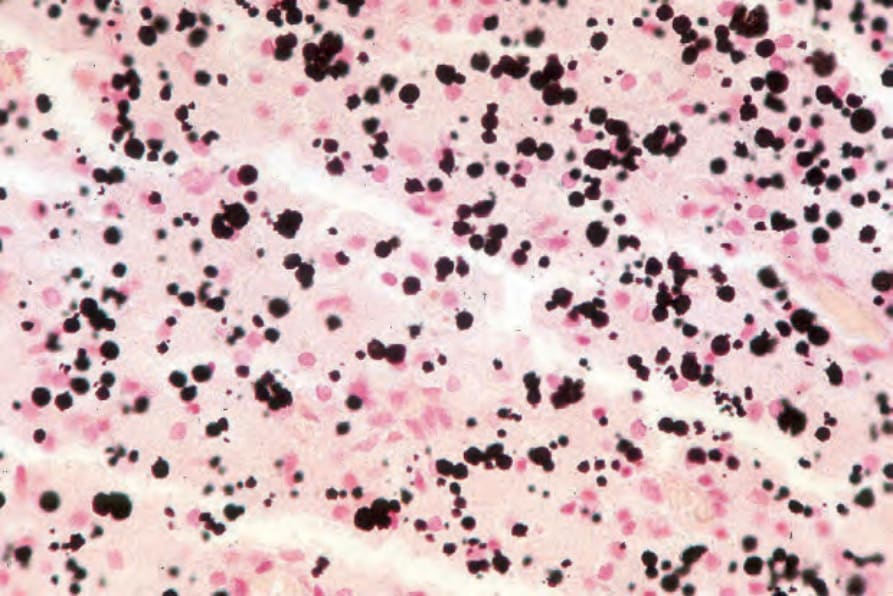
圖 18-227:Malakoplakia:使用 von Kossa 反應 (von Kossa reaction) 可使 Michaelis-Gutmann bodies 更為明顯,並顯示其數量遠較 hematoxylin and eosin 染色所見更為眾多。
Fig. 18.227 Malakoplakia: use of the von Kossa reaction renders the Michaelis-Gutmann bodies more conspicuous and reveals that they are much more numerous than was apparent in the hematoxylin and eosin stain.

圖 18-228:Actinomycosis:廣泛的胸腔內疾病 (intrathoracic disease) 已導致前胸壁受侵犯。可見眾多竇道 (sinuses)。By courtesy of P. Duhra, MD, Coventry and Warwickshire Hospital, Coventry, UK。
Fig. 18.228 Actinomycosis: extensive intrathoracic disease has resulted in involvement of the anterior chest wall. Numerous sinuses are evident. By courtesy of P. Duhra, MD, Coventry and Warwickshire Hospital, Coventry, UK.

圖 18-229:Actinomycosis:頸顏面區域 (cervicofacial region) 的感染;注意排膿竇道 (draining sinus) 部位的疤痕與凹陷。By courtesy of T.F. Sellers, MD, and H.P. Lambert, MD, St George’s Hospital, London, UK。
Fig. 18.229 Actinomycosis: infection of the cervicofacial region; note the scarring and dimple at the site of the draining sinus. By courtesy of T.F. Sellers, MD, and H.P. Lambert, MD, St George’s Hospital, London, UK.

圖 18-230:Actinomycosis:外踝 (lateral malleolus) 周圍出現多個竇道 (sinuses)。By courtesy of R. Hay, Institute of Dermatology, London, UK。
Fig. 18.230 Actinomycosis: multiple sinuses are present about the lateral malleolus. By courtesy of R. Hay, Institute of Dermatology, London, UK.
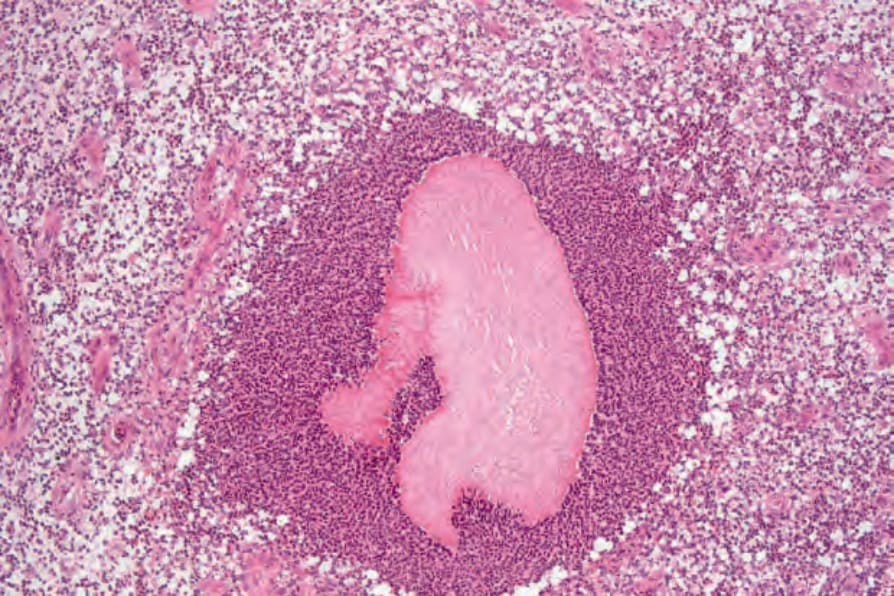
圖 18-231:Actinomycosis:一個細菌菌落 (bacterial colony) 位於膿瘍 (abscess) 中央。
Fig. 18.231 Actinomycosis: a bacterial colony lies in the center of an abscess.
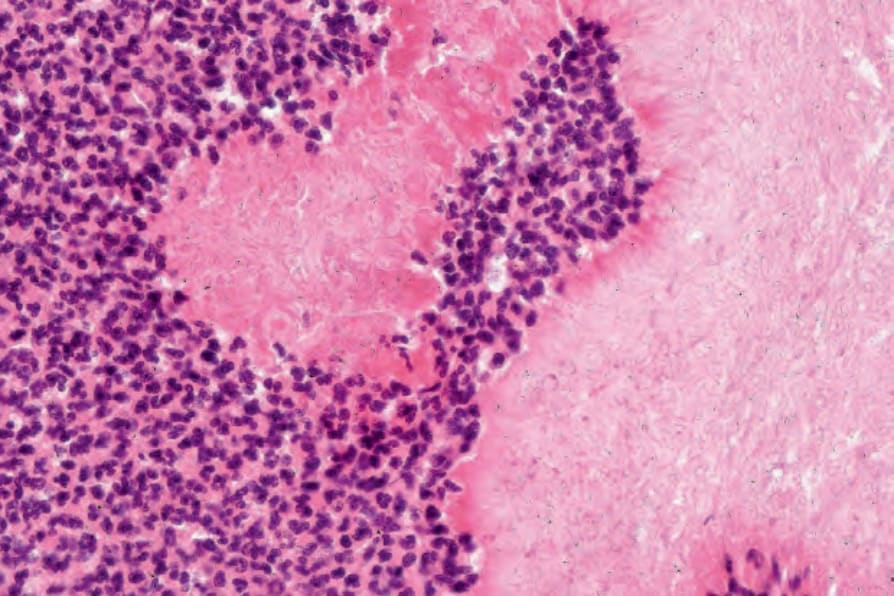
圖 18-232:Actinomycosis:高倍視野 (high-power view)。
Fig. 18.232 Actinomycosis: high-power view.
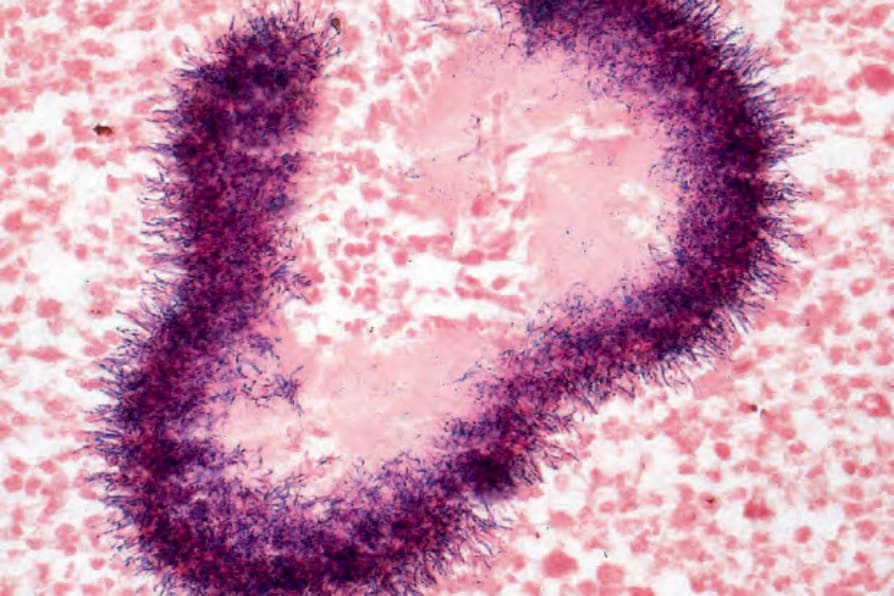
圖 18-233:Actinomycosis:顆粒邊緣可見帶有棒狀末端 (club-shaped ends) 的革蘭氏陽性細菌 (Gram-positive bacteria)。
Fig. 18.233 Actinomycosis: Gram-positive bacteria with club-shaped ends are present at the periphery of the granule.