Actinomycosis
Actinomycosis
Clinical features Actinomyces israelii is a commensal in the human mouth, along with other organisms including Aggregatibacter (formerly Actinobacillus) actinomycetemcomitans.1 A. israelii is the usual pathogen but occasionally other species including A. viscosus, A. naeslundii, A. odontolyticus, A. meyeri, A. turicensis, A. radingae, and A. neuii are implicated.2–7 The most common manifestation is cervicofacial actinomycosis, but more grave pulmonary and intestinal infections can occur and, rarely, purely cutaneous lesions.1,8–12 The cervicofacial form is common in farm workers and is associated with poor oral hygiene, usually starting from carious teeth and following dental extractions or oral trauma. The condition is infrequent in children and most common in young men. Respiratory involvement as lung abscess and fistulae may ‘point’ through the thoracic wall (Fig. 18.228).13 Abdominal lesions include appendiceal and colonic actinomycosis and hepatic involvement, and it may complicate the use of intrauterine contraceptive devices, with lesions affecting the internal female genitalia. Cutaneous fistulae may subsequently develop.14,15
that occasionally contain intact and partly digested bacteria. It has been suggested that phagolysosomes in macrophages accumulate in response to chronic bacterial infection. The infection is not by one specific organism, but the agent is usually E. coli.4 The phagolysosomes tend to fuse and then calcify; the reason for these changes is not clear, although some cases occur in systemic disease associated with a probable impairment of macrophage function.1,5 Other organisms that have been cultured from lesions of malakoplakia include Gram-negative bacilli (Klebsiella spp., Enterobacter spp., Proteus spp., Pseudomonas spp., Burkholderia cepacia complex) and Gram-positive cocci, including Staphylococcus aureus, Streptococcus spp., and enterococci.4,5,12,15
The cervicofacial lesion presents as a hard swelling on the lower jaw or, occasionally, as a plaquelike infiltration of the cheek from the upper jaw (cf. bovine lumpy jaw). These firm thickened areas tend to discharge through sinuses and are associated with scarring and the formation of new nodules (Fig. 18.229). Yellow granules measuring up to 2 mm in diameter – the so-called ‘sulfur granules’ – are occasionally found in the discharging pus. Extensions of some maxillary lesions may reach the orbit and base of the skull. Uncommonly, a large facial mass may develop.5,16
Differential diagnosis Malakoplakia should be distinguished from infectious granulomata, histiocytosis, and granular cell tumor, and from pseudomalakoplakia,4,15,16 which refers to an abnormal histiocytic proliferation in a previous surgical site. Although pseudomalakoplakia also comprises sheets of large histiocytes with intracytoplasmic calcific material, this condition is distinguished from true malakoplakia by the lack of concentric lamination of the granules.15,16
Rarely, direct inoculation of skin may produce a similar chronically discharging abscess with adjacent scarring (Fig. 18.230). Alternatively, a mycetoma or chronic discharging abscess mass with multiple sinuses may develop. This primary form of cutaneous actinomycosis is rare. Sites have included the thigh, the femorogluteal region, the arm, the penis, the breast, the neck, the nose, and the forehead.7,17–25 Most cases are the result of external trauma and local ischemia, but this is not always the case.17,21,22,25–27 Some infections have been acquired through injection wounds, including one report where an A. odontolyticus-associated subcutaneous abscess evolved in an intravenous cocaine user who admitted to licking his hypodermic needle prior to injection.17,28 Very rarely, primary cutaneous actinomycosis may be a presenting manifestation of underlying HIV infection.6 There is an isolated report of A. bovis infection affecting the fingernails of a patient with common variable immunodeficiency.29
910 Infectious diseases of the skin
An uncommon form of the disease is the presence of disseminated cutaneous lesions in the absence of demonstrable extracutaneous infection; this has been reported in a patient with acute leukemia.30
Pathogenesis and histologic features The mixture of organisms involved in actinomycosis is not purely accidental but is synergistic. A. israelii is a Gram-positive, nonacid-fast, microaerophilic bacterium with filamentous branching organisms. A. actinomycetemcomitans is a Gram-negative coccobacillus which inhibits growth of fibroblasts and keratinocytes. It is speculated that this, together with its different susceptibility to antibiotics, helps to maintain the actinomycotic lesion.
Histologically, the lesions have the features of chronic abscesses and sinuses, containing pus and surrounded by fibrosis and a mixed inflammatory infiltrate (Fig. 18.231). Locules separated by granulation tissue are present. Sulfur granules of intertwined bacteria are seen, radiating mycelial filaments, often with opaque clubs at their tips (Figs 18.232 and 18.233).31 These granules may be associated with the Splendore-Hoeppli phenomenon.
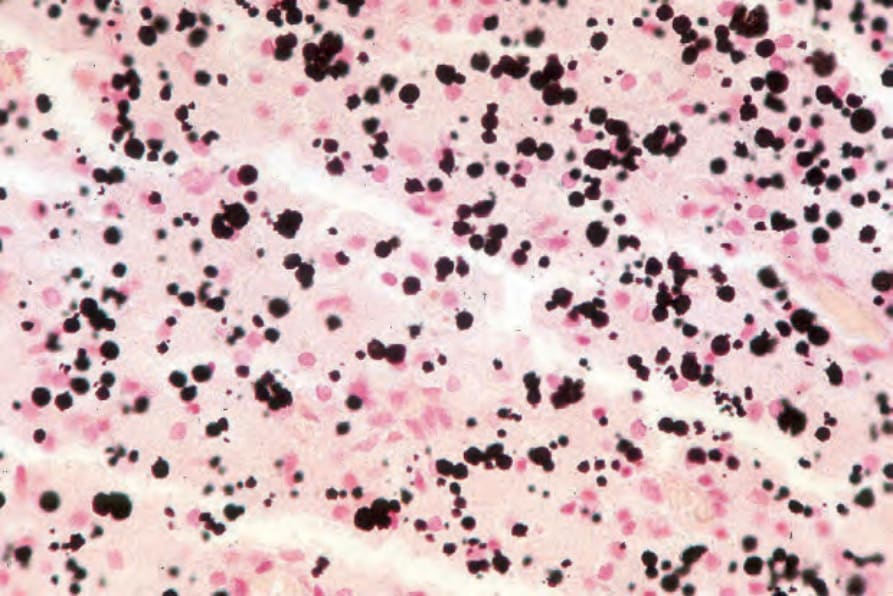
Fig. 18.227 Malakoplakia: use of the von Kossa reaction renders the Michaelis-Gutmann bodies more conspicuous and reveals that they are much more numerous than was apparent in the hematoxylin and eosin stain.

Fig. 18.228 Actinomycosis: extensive intrathoracic disease has resulted in involvement of the anterior chest wall. Numerous sinuses are evident. By courtesy of P. Duhra, MD, Coventry and Warwickshire Hospital, Coventry, UK.

Fig. 18.229 Actinomycosis: infection of the cervicofacial region; note the scarring and dimple at the site of the draining sinus. By courtesy of T.F. Sellers, MD, and H.P. Lambert, MD, St George’s Hospital, London, UK.

Fig. 18.230 Actinomycosis: multiple sinuses are present about the lateral malleolus. By courtesy of R. Hay, Institute of Dermatology, London, UK.
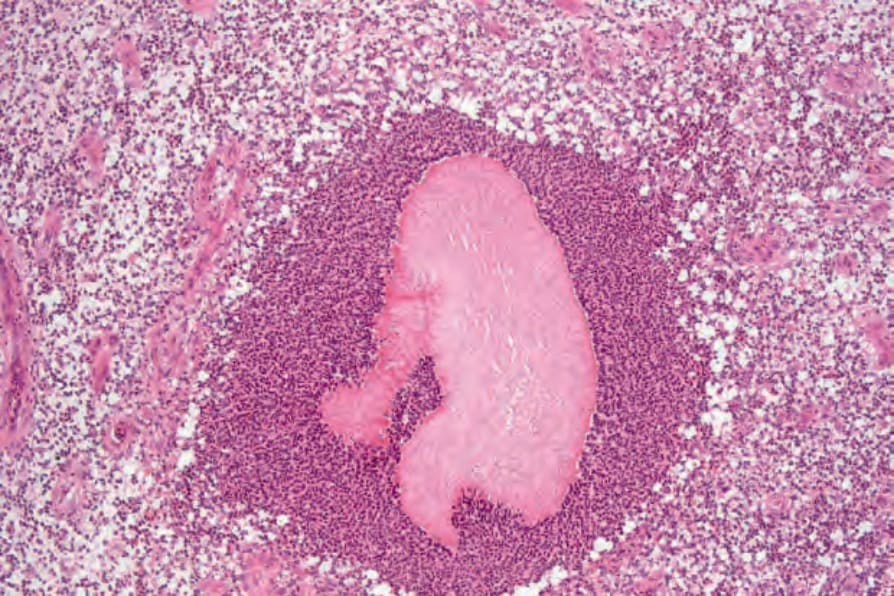
Fig. 18.231 Actinomycosis: a bacterial colony lies in the center of an abscess.
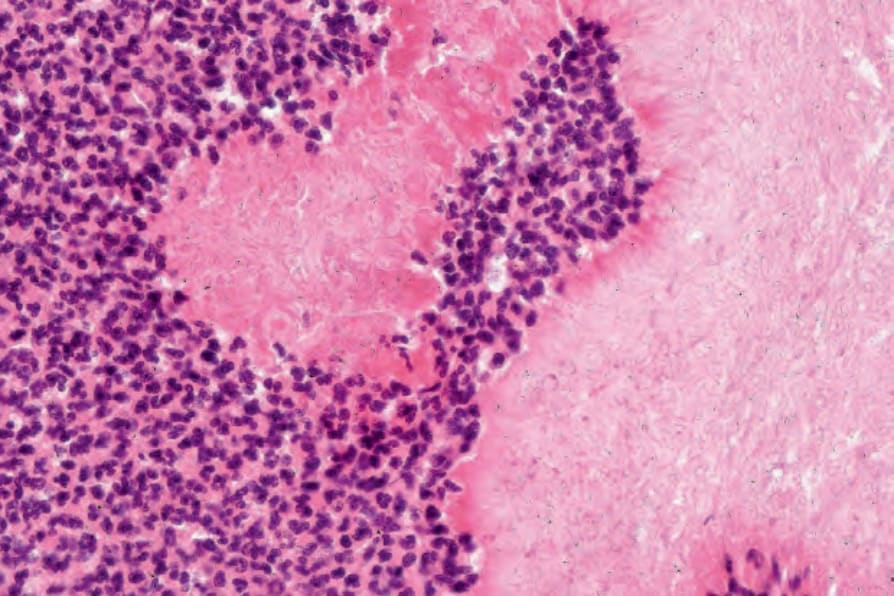
Fig. 18.232 Actinomycosis: high-power view.
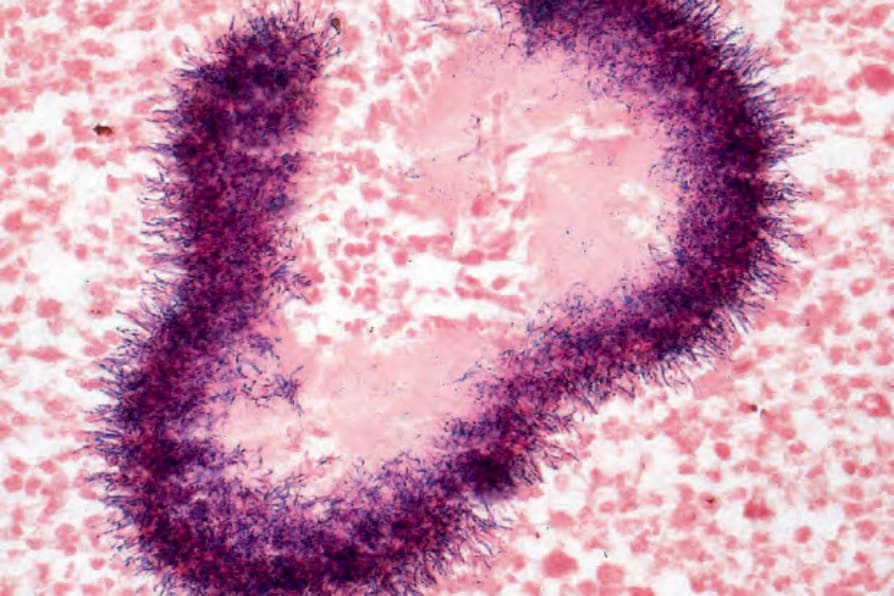
Fig. 18.233 Actinomycosis: Gram-positive bacteria with club-shaped ends are present at the periphery of the granule.