地方性梅毒 (Endemic syphilis)
臨床特徵 (Clinical Features)
地方性梅毒 (endemic syphilis;又稱 Syrian bejel) 是一種非性病性梅毒螺旋體病 (nonvenereal treponematosis),由 Treponema pallidum subsp. endemicum 所引起,此菌與性病性梅毒 (venereal syphilis) 的病原 T. pallidum subsp. pallidum 幾乎完全相同。此病通常發生於生活在衛生條件不良環境中的兒童,並經由皮膚接種 (cutaneous inoculation) 傳播。其他地方性形式則與共用飲水器皿及其他受污染的家庭用具有關——當社群中某些成員具有口腔或唇部梅毒病灶時即可能發生。雖然 endemic syphilis 在二十世紀已大致從歐洲根除,但此病仍見於中東與非洲部分地區,尤其是鄉村沙漠地帶。
在 late yaws 的病灶出現之前,可能有一段 3–5 年的無症狀期。晚期病灶於約 10% 的患者中發生,為破壞性潰瘍與膠腫結節 (gummatous nodules),侵犯皮膚、骨骼(例如刀鞘狀脛骨 saber tibia)與關節(圖 18.141 與 18.142)。late yaws 的皮膚表現包括掌蹠角化過度 (palmar and plantar hyperkeratosis;crab yaws)、色素脫失 (pintoid yaws) 與膠腫 (gummata)。Pintoid yaws 包括角化過度、攣縮 (contractures)、關節旁結節 (juxta-articular nodules) 與骨病灶。膠腫特徵性地侵犯長骨、手足骨骼,並典型地導致顏面的嚴重破壞 (gangosa)。一般認為心血管與神經系統不受侵犯,但有部分歷史證據顯示在流行地區可能發生眼部病變與脊髓神經病變 (myeloneuropathies)。
與性病性梅毒不同,地方性梅毒中很少出現原發性下疳 (primary chancre);然而,哺餵受感染嬰兒的婦女可能於乳頭發生原發性感染。原發性病灶通常侵犯口咽部,但容易被忽略。早期次發性病灶表現為柔軟、卵圓形的黏膜斑塊 (mucous patches),好發於頰黏膜與唇黏膜,有時伴隨口角炎 (angular stomatitis)。黏膜斑塊也可能出現於肛周與生殖器部位,在該處有時呈疣狀外觀 (condylomatous)。可能發生骨膜骨炎 (osteoperiostitis),且全身性淋巴結腫大 (generalized lymphadenopathy) 常見。
晚期(第三期)表現於 5 至 15 年的潛伏期後發展。病灶可能於皮膚、鼻咽、骨骼演變,
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
引起 yaws 的螺旋體在形態學上與 T. pallidum subsp. pallidum 無法區分。全基因組定序 (whole genome sequencing) 顯示這些菌在基因組序列上的差異小於 0.2%。
879 Endemic (nonvenereal) treponematoses
早期病灶特徵為角化不全 (parakeratotic)、棘層肥厚 (acanthotic) 與乳頭瘤狀 (papillomatous)。它們顯示局灶性海綿水腫 (focal spongiosis) 與表皮內中性球並伴有微膿瘍形成 (microabscess formation)(圖 18.143)。真皮內有緻密的血管周圍浸潤,含有大量漿細胞 (plasma cells)。與梅毒相比,其血管變化通常不顯著。可於血管周圍、真皮乳頭尖端及表皮內見到螺旋體 (treponemes)(圖 18.144)。
A
掌蹠病灶的特徵為角化過度 (hyperkeratosis)、角化不全 (parakeratosis) 與棘層肥厚 (acanthosis)。淺層真皮可見輕度非特異性慢性發炎細胞浸潤。
膠腫顯示中央乾酪樣壞死 (caseation necrosis),周圍環繞淋巴細胞、漿細胞、組織球 (histiocytes)、上皮樣細胞 (epithelioid cells) 與巨細胞 (giant cells)。並伴有纖維化。

圖 18.139:早期 yaws:典型的覆盆子狀 (framboesiform)「母 yaw (mother yaw)」。注意黃色痂皮與周圍色素減退 (hypopigmentation)。By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.
Fig. 18.139 Early yaws: typical framboesiform ‘mother yaw’. Note the yellow crust and surrounding hypopigmentation. By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.

圖 18.141:晚期 yaws:注意此晚期階段小腿的彎曲,伴有皮膚潰瘍與結痂病灶。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 18.141 Late yaws: note the bowing of the lower leg with cutaneous ulcerated and crusted lesions in this late stage. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
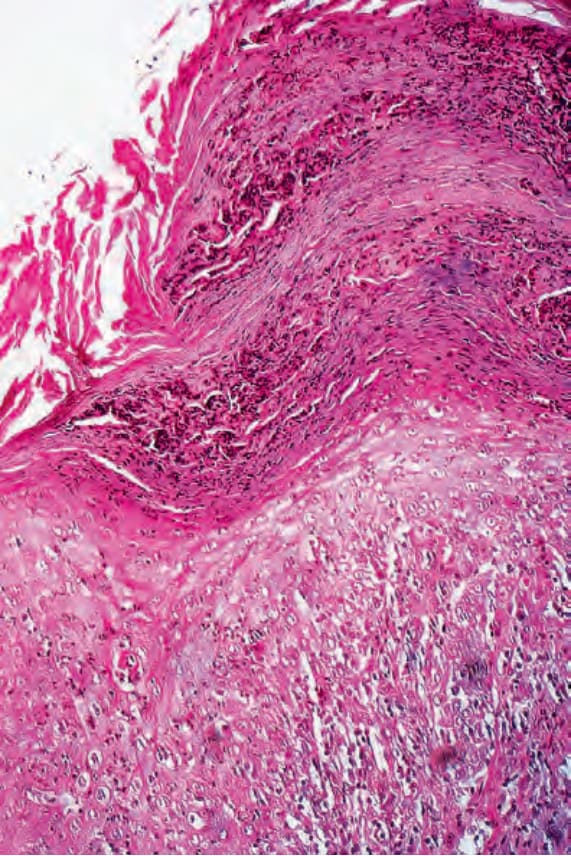
圖 18.143:早期 yaws:通過一處演變中乳頭瘤的切片。可見非常顯著的角化不全 (parakeratosis),並伴有大量中性球碎屑。表皮顯示強烈的急性發炎。By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.
Fig. 18.143 Early yaws: biopsy through an evolving papilloma. There is very marked parakeratosis associated with abundant neutrophil debris. The epidermis shows intense acute inflammation. By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.
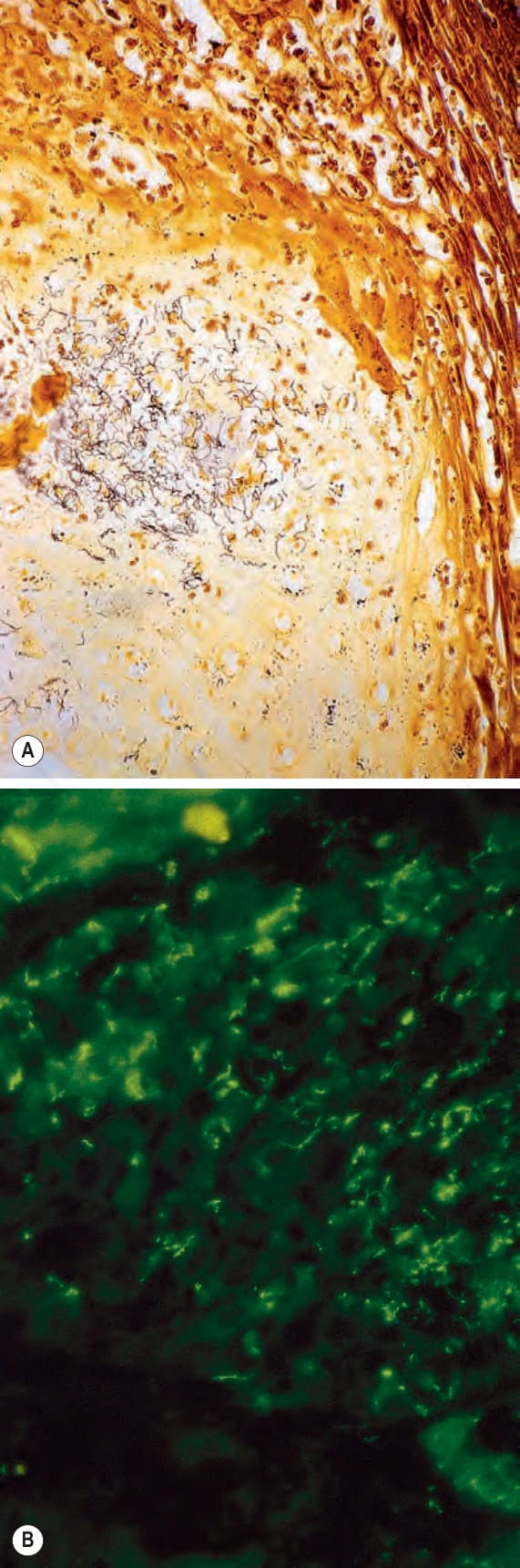
圖 18.144:(A, B) 早期 yaws:與圖 18.140 所示為同一檢體。注意大量螺旋體 (spirochetes) 的存在。(A) Warthin-Starry 染色;(B) 免疫螢光 (immunofluorescence)。By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.
Fig. 18.144 (A, B) Early yaws: same specimen as that shown in Fig. 18.140. Note the presence of numerous spirochetes. (A) Warthin-Starry; (B) immunofluorescence. By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.