Endemic syphilis
Endemic syphilis
Clinical features Endemic syphilis (Syrian bejel) is a form of nonvenereal treponematosis caused by Treponema pallidum subsp. endemicum, an organism nearly identical to T. pallidum subsp. pallidum, the etiological agent of venereal syphilis.1–5 The condition usually occurs in children living in conditions of poor hygiene and is transmitted by cutaneous inoculation.1,3–7 Other endemic forms have been associated with shared drinking vessels and other contaminated domestic utensils when some members of the community have oral or labial syphilitic lesions.1,3–6 Although endemic syphilis was largely eradicated from Europe in the twentieth century, the disease still occurs in parts of the Middle East and Africa, especially in rural desert regions.1,3,4,8,9
There may be a symptom-free period of 3–5 years before the lesions of late yaws arise. The late lesions, which develop in about 10% of patients, are destructive ulcers and gummatous nodules which affect the skin, bones (e.g., saber tibia), and joints (Figs 18.141 and 18.142).3,6,18,19,22 Cutaneous manifestations of late yaws include palmar and plantar hyperkeratosis (crab yaws), loss of pigment (pintoid yaws), and gummata. Pintoid yaws includes hyperkeratosis, contractures, juxta-articular nodules, and bony lesions.6,19 Gummata characteristically involve the long bones, the bones of the hands and feet, and typically lead to gross destruction of the face (gangosa).24 The cardiovascular and nervous systems are said not to be involved, but there is some historical evidence to suggest that ophthalmic and myeloneuropathies might occur in endemic areas.18,20,25
Unlike venereal syphilis, a primary chancre seldom occurs in endemic syphilis; women suckling infected infants may, however, develop primary infections of the nipple.1,3 The primary lesions usually involve the oropharynx but are easily overlooked. Early secondary lesions manifest as soft, oval mucous patches with a predilection for the buccal and labial mucosae, sometimes accompanied by angular stomatitis. Mucous patches may also occur in the perianal and genital areas, where they sometimes appear condylomatous. Osteoperiostitis may occur, and generalized lymphadenopathy is common.1,3
Late (tertiary) manifestations develop following a latent period of between 5 and 15 years. The lesions may evolve in the skin, nasopharynx, bone,
Pathogenesis and histologic features The spirochete responsible for yaws is morphologically indistinguishable from T. pallidum subsp. pallidum. Whole genome sequencing has revealed that these organisms differ in less than 0.2% of the genomic sequence.22,26
879 Endemic (nonvenereal) treponematoses
Early lesions are characteristically parakeratotic, acanthotic, and papillomatous. They show focal spongiosis and intraepidermal neutrophils with microabscess formation (Fig. 18.143).22 There is a dense perivascular dermal infiltrate containing numerous plasma cells. The vascular changes in contrast to syphilis are usually insignificant. Treponemes can be seen around the blood vessels, in the tips of the dermal papillae, and within the epidermis (Fig. 18.144).1,3,23,27–29
A
The palmoplantar lesions are characterized by hyperkeratosis, parakeratosis, and acanthosis. A mild non-specific chronic inflammatory cell infiltrate is present in the superficial dermis.
The gummata show central caseation necrosis surrounded by a rim of lymphocytes, plasma cells, histiocytes, epithelioid cells, and giant cells.1,23 There is associated fibrosis.

Fig. 18.139 Early yaws: typical framboesiform ‘mother yaw’. Note the yellow crust and surrounding hypopigmentation. By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.

Fig. 18.141 Late yaws: note the bowing of the lower leg with cutaneous ulcerated and crusted lesions in this late stage. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
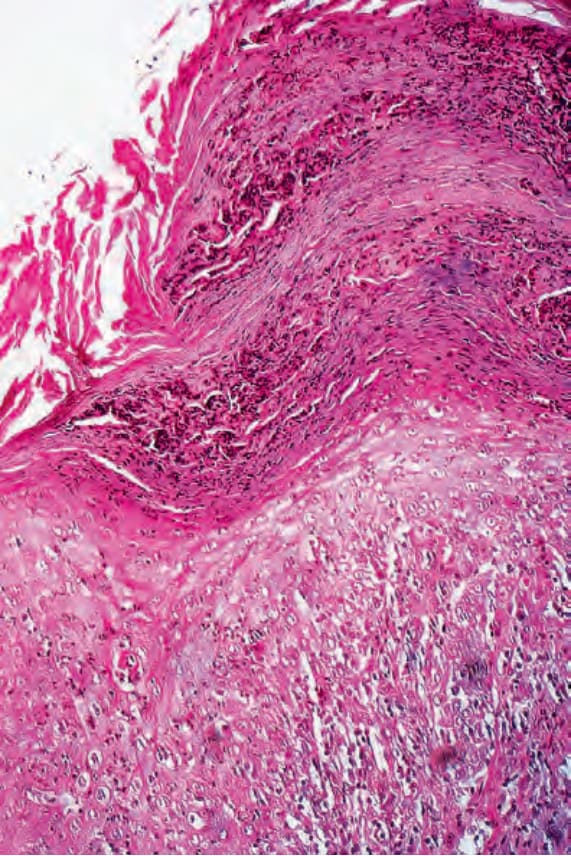
Fig. 18.143 Early yaws: biopsy through an evolving papilloma. There is very marked parakeratosis associated with abundant neutrophil debris. The epidermis shows intense acute inflammation. By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.
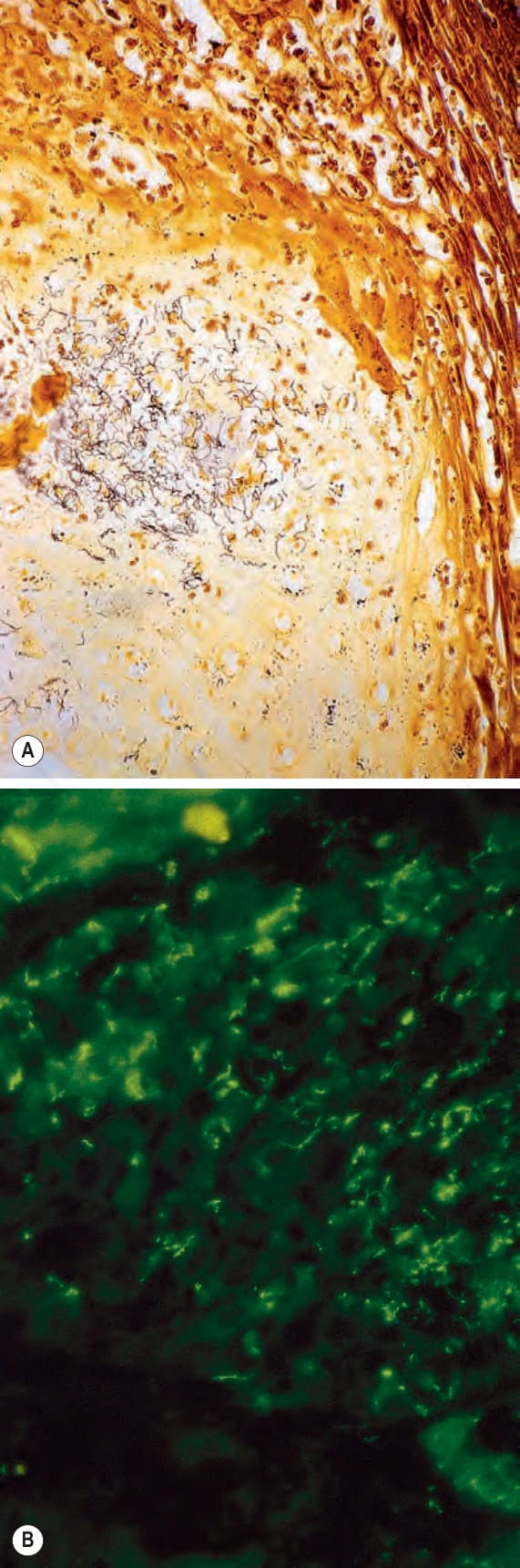
Fig. 18.144 (A, B) Early yaws: same specimen as that shown in Fig. 18.140. Note the presence of numerous spirochetes. (A) Warthin-Starry; (B) immunofluorescence. By courtesy of H.J.H. Engelkens, MD, and E. Stolz, MD, University Hospital, Rotterdam-Dijkzigt and Erasmus University, Rotterdam, The Netherlands.