皮膚炭疽 (Cutaneous Anthrax)
臨床特徵 (Clinical Features)
-
炭疽 (anthrax) 是由 Bacillus anthracis 引起的人畜共通感染 (zoonotic infection),此菌為一種具莢膜、會形成芽孢 (spore-forming) 的 Gram 陽性桿菌。
-
此病在人類相對少見,但在全世界的熱帶與亞熱帶地區(包括非洲與南美洲)、南歐、土耳其、中東及印度,仍會發生流行性爆發 (epidemic outbreaks)。在已開發國家則極為罕見。
-
皮膚炭疽 (cutaneous anthrax) 占全部病例的百分之九十五以上;肺型 (pulmonary) 與胃腸道型 (gastrointestinal) 一般占其餘部分,且死亡率高。
-
然而近年來出現了第四型疾病——注射型(注射性)炭疽 (injection [injectional] anthrax)。後者發生於靜脈注射藥物使用者,尤其是海洛因 (heroin) 使用者。迄今所記錄的所有病例似乎都發生於歐洲,感染歸因於海洛因受到污染。
-
皮膚炭疽發生於 B. anthracis 接種進入有擦傷的皮膚之後。經過 2–3 週的潛伏期後,會出現一個紅斑性斑疹 (erythematous macule) 或丘疹 (papule)。此後演變為一個搔癢性水疱 (pruritic vesicle)。在水疱破裂後,會形成具特徵性的黑色焦痂 (black eschar)(Figs 18.120 and 18.121)。
-
周圍皮膚常有明顯的水腫 (edema) 與紅斑 (erythema),有時伴隨大疱 (bullae) 形成。感染可能以眼周侵犯 (periorbital involvement) 表現。
-
有時可見淋巴結炎 (lymphadenitis)。未治療的病例可能發生敗血症 (septicemia);此情形的死亡率為百分之十至百分之二十。也曾報告毒血性休克 (toxemic shock) 與腎衰竭 (renal failure)。
-
一種罕見型的疾病稱為惡性水腫 (malignant edema),表現為嚴重、迅速擴散的水腫、淋巴管炎 (lymphangitis)、淋巴結炎 (lymphadenitis) 與全身性症狀。這些病例可能演變出出血性與壞死性水疱 (hemorrhagic and necrotic vesicles)。
-
在注射型炭疽 (injection anthrax) 病人中記錄到的併發症包括多重器官衰竭 (multiorgan failure)、腔室症候群 (compartment syndrome)、NF(壞死性筋膜炎)與致命性頸部蜂窩組織炎 (lethal cervical cellulitis)。注射型炭疽的死亡率高達百分之三十七。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
-
B. anthracis 帶有強效的毒力因子 (virulence factors),亦即具有抗吞噬 (antiphagocytic) 特性的 poly-D-glutamic acid 莢膜,以及一種由質體編碼 (plasmid-encoded) 的多胜肽蛋白外毒素 (polypeptide protein exotoxin),由三個成分組成:edema factor (EF)、protective antigenic factor (PA) 與 lethal factor (LF)。
-
Anthrax toxin receptor 2 (ANTXR2) 與 capillary morphogenesis protein 2 (CMG2) 是炭疽毒素的主要受體。PA 與細胞受體的結合促進 EF 與 LF 轉位 (translocation) 進入宿主細胞,繼而改變細胞訊息傳遞路徑 (cell signaling pathways)。EF 透過產生或釋放發炎介質——包括 neurokinins、prostanoids 與 histamine——而導致血管通透性 (vascular permeability) 增加。
-
組織學圖像以大量的表皮下水腫 (massive subepidermal edema) 為主(Fig. 18.122)。表皮內水腫 (intraepidermal edema) 造成融合性的細胞間空泡 (coalescent intercellular vacuoles)。表皮常被拉薄 (attenuated)。
-
真皮被一個緻密的發炎浸潤所擴張,此浸潤由大量的多形核白血球 (polymorphonuclear leukocytes) 組成,混雜有淋巴球 (lymphocytes) 與組織球 (histiocytes)。此過程常延伸至皮下脂肪。血管擴張 (vasodilatation) 可能很明顯。
-
出血 (hemorrhage) 與纖維蛋白沈積 (fibrin deposition) 發生於深層真皮與皮下組織(Fig. 18.123)。在深層真皮與皮下脂肪中,可能遇到血栓性血管阻塞 (thrombotic vascular occlusion) 與血管壁的類纖維蛋白壞死 (fibrinoid necrosis)(Fig. 18.124)。Gram 染色將顯示為數可觀的大型 Gram 陽性桿菌,主要分布於淺層真皮(Fig. 18.125)。
-
診斷由培養 (culture) 確認。血清學檢查 (serological investigations) 亦可使用。免疫組織化學 (immunohistochemical) 偵測方法可用於組織檢體。
來自土耳其與中東。死亡率低,大多數病人在 3 個月內康復。
皮膚表現發生於約百分之六或更少的病例中;然而此數字在來自土耳其的一個系列中接近百分之十四。已記錄到許多種皮膚表現,包括瀰漫性丘疹結節性疹 (disseminated papulonodular eruption)、瀰漫性斑丘疹 (diffuse maculopapular rash)、類似結節性紅斑的皮下結節 (erythema nodosum-like subcutaneous nodules)、紫斑 (purpura)、白血球碎裂性血管炎 (leukocytoclastic vasculitis)、多形性紅斑 (erythema multiforme)、類似蕁麻疹的丘疹與斑塊 (urticaria-like papules and plaques)、多發性膿瘍 (multiple abscesses)、皮膚潰瘍 (cutaneous ulcers)、瘀斑 (ecchymoses),以及(罕見地)網狀青斑 (livedo reticularis)、掌部紅斑 (palmar erythema),或甚至一個模仿軟組織腫瘤的大型腫塊。血管炎性皮膚病灶可能構成感染誘發的全身性血栓性微血管病變 (systemic thrombotic microangiopathy) 的一部分,類似 Henoch-Schönlein purpura。有一例 Brucella 相關 Stevens-Johnson syndrome 的單一病例報告。接觸性 brucellosis 表現為紅斑或搔癢,通常在前臂或手部。在某些病例中,這可能進展為毛囊性、水疱性或膿疱性疹。曾記錄到一例罕見的、繼發於潛在 Brucella 慢性骨髓炎 (chronic osteomyelitis) 的鄰接皮膚侵犯病例。亦曾報告一例由自體接種 (autoinoculation) 引起的人為性 (factitious) brucellosis 病例;該病人發生菌血症 (bacteremia) 與潰瘍性皮膚膿瘍 (ulcerating cutaneous abscesses)。
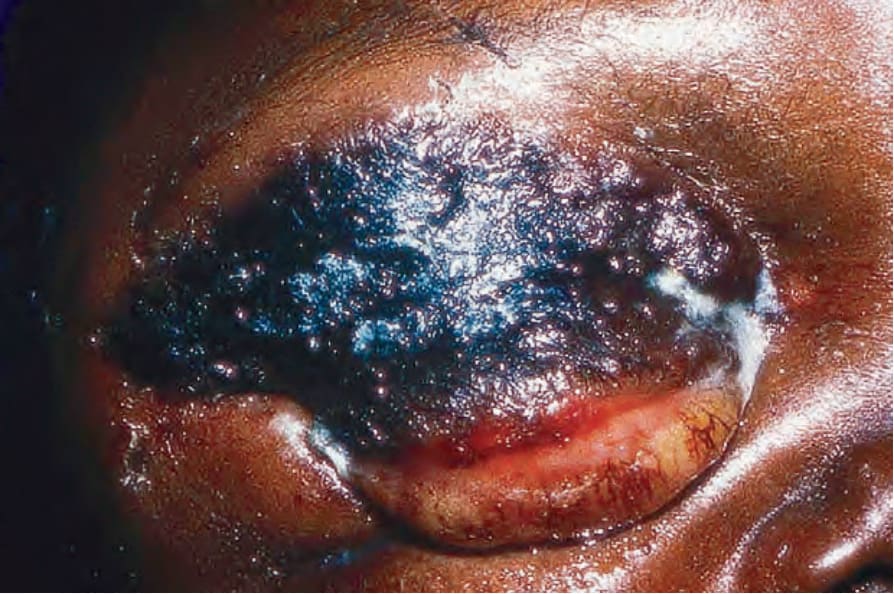
圖 18-120:炭疽 (anthrax):皮膚型疾病是人類最常見的表現。此黑色結痂病灶 (black crusted lesion) 為典型表現。By courtesy of J. Frean, MD, and the late M. Isaäcson, MD, University of Witwatersrand, Johannesburg, South Africa.
Fig. 18.120 Anthrax: cutaneous disease is the commonest manifestation in humans. This black crusted lesion is typical. By courtesy of J. Frean, MD, and the late M. Isaäcson, MD, University of Witwatersrand, Johannesburg, South Africa.
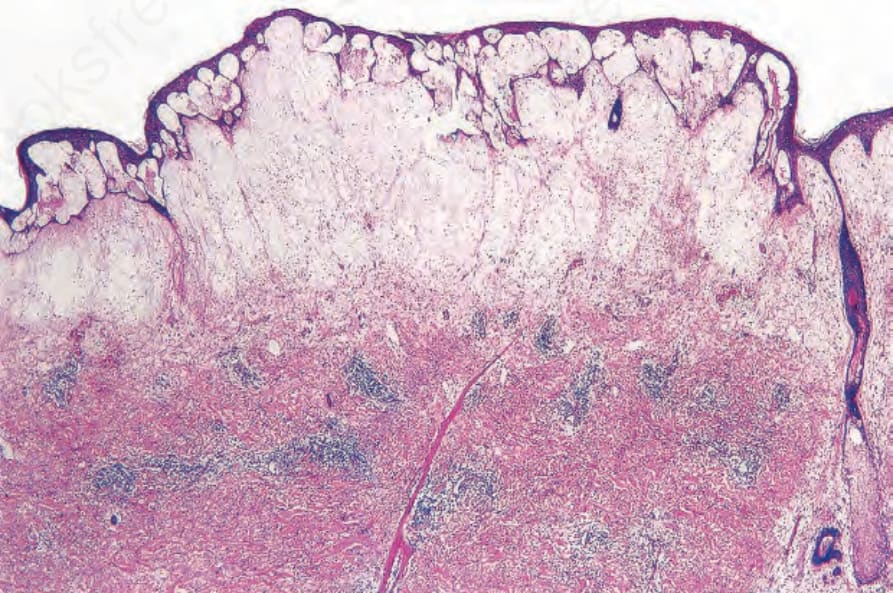
圖 18-122:炭疽 (anthrax):可見大量的表皮下水腫 (massive subepidermal edema) 伴隨表皮下水疱形成 (subepidermal vesiculation)。Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.
Fig. 18.122 Anthrax: there is massive subepidermal edema with subepidermal vesiculation. Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.
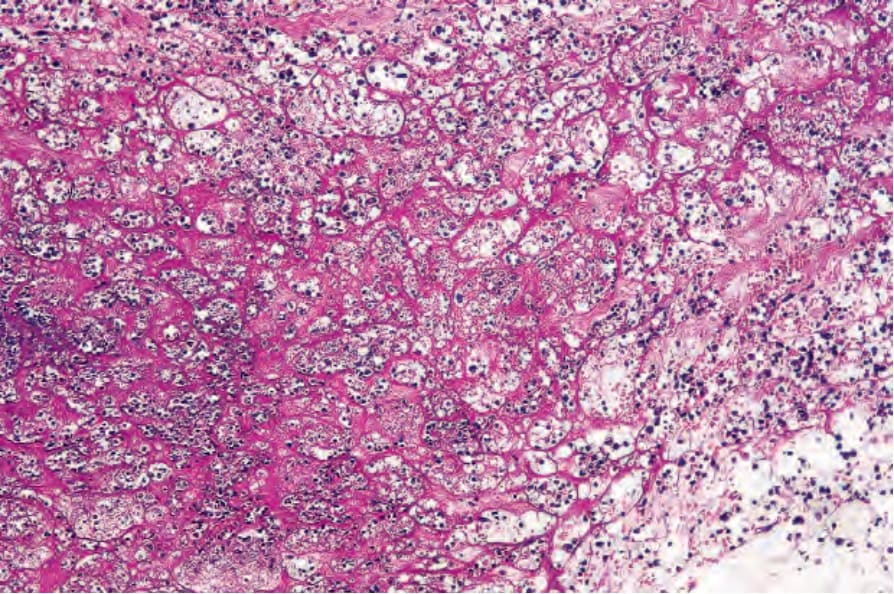
圖 18-123:炭疽 (anthrax):可見明顯的纖維蛋白沈積 (fibrin deposition)。Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.
Fig. 18.123 Anthrax: marked fibrin deposition is evident. Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.
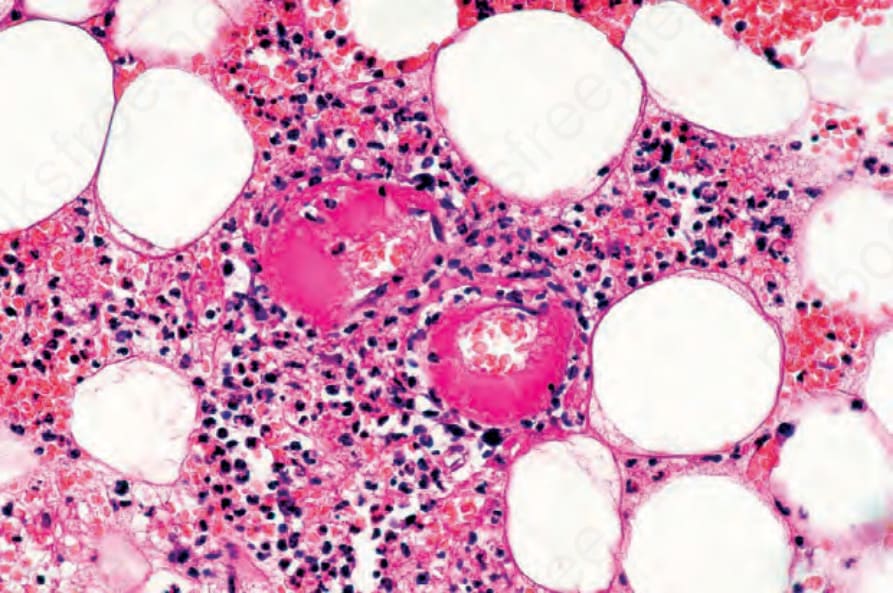
圖 18-124:炭疽 (anthrax):可見血栓化的血管 (thrombosed vessels)。Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.
Fig. 18.124 Anthrax: thrombosed vessels are present. Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.
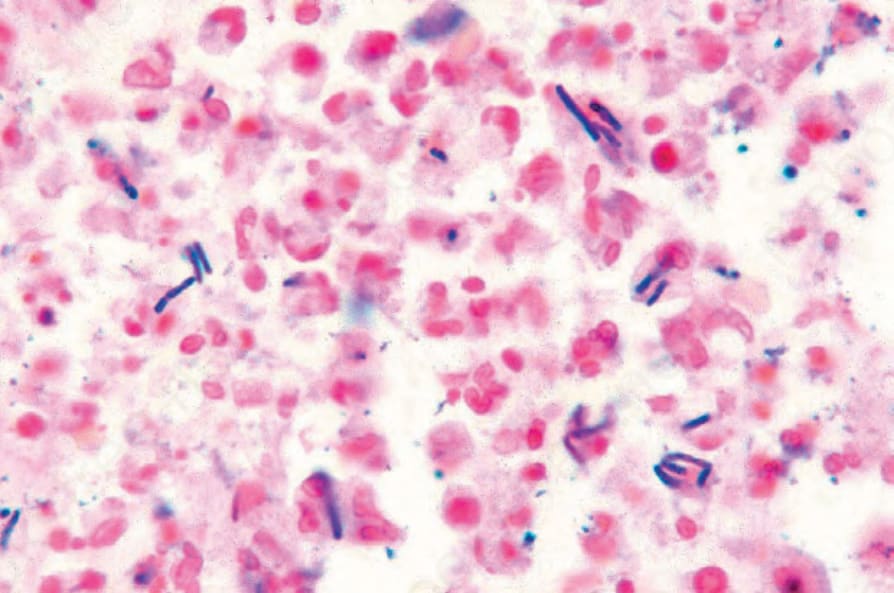
圖 18-125:炭疽 (anthrax):可見許多細長的 Gram 陽性桿菌 (Gram-positive bacilli)。Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.
Fig. 18.125 Anthrax: numerous elongated Gram-positive bacilli are present. Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.