Cutaneous anthrax
Cutaneous anthrax
Clinical features Anthrax is a zoonotic infection caused by Bacillus anthracis, an encapsulated, spore-forming, Gram-positive bacillus.1–3 Although the condition is relatively uncommon in humans, epidemic outbreaks still occur in tropical and subtropical regions of the world (including Africa and South America), southern Europe, Turkey, the Middle East, and India.2–8 Anthrax is very rarely seen in developed countries.9–11 Cutaneous anthrax accounts for more than 95% of cases; pulmonary and gastrointestinal forms generally account for the remainder, and are associated with a high mortality.2 Recent years, however, have seen the emergence of a fourth form of the disease – injection (injectional) anthrax. The latter occurs among users of intravenous drugs, notably heroin. All of the cases recorded thus far appear have occurred in Europe, and the infection is attributed to contamination of the heroin.12–16
Cutaneous anthrax occurs after inoculation of B. anthracis into abraded skin. An erythematous macule or papule develops after an incubation period of 2–3 weeks. This later evolves into a pruritic vesicle. A characteristic black eschar develops after breakdown of the blister (Figs 18.120 and 18.121).2,20,21 There is often pronounced edema and erythema of the surrounding skin, sometimes accompanied by the formation of bullae.2,20 The infection may present with periorbital involvement.22 Lymphadenitis is sometimes seen. Septicemia may arise in untreated cases; this carries a mortality of 10% to 20%.2,3 Toxemic shock and renal failure have also been reported.20,23 A rare form of the disease termed malignant edema presents with severe, rapidly spreading edema, lymphangitis, lymphadenitis, and systemic symptoms. Hemorrhagic and necrotic vesicles may evolve in these cases.2,20 Complications documented among patients with injection anthrax
871 Brucellosis
have included mulitorgan failure, compartment syndrome, NF, and lethal cervical cellulitis.12,13,15 Injection anthrax carries a mortality of up to 37%.16
Pathogenesis and histologic features B. anthracis is associated with potent virulence factors, namely, a poly-Dglutamic acid capsule with antiphagocytic properties, and a plasmid-encoded polypeptide protein exotoxin consisting of three components: edema factor (EF), protective antigenic factor (PA), and lethal factor (LF).1,3,24 Anthrax toxin receptor 2 (ANTXR2) and capillary morphogenesis protein 2 (CMG2) are the major receptors for anthrax toxins.1,25,26 Binding of PA to cellular receptors facilitates translocation of EF and LF into host cells, with subsequent alterations in cell signaling pathways.1 EF leads to increased vascular permeability via the production or release of inflammatory mediators, including neurokinins, prostanoids, and histamine.27
The histologic picture is dominated by massive subepidermal edema (Fig. 18.122).9,28 Intraepidermal edema results in coalescent intercellular vacuoles.2 The epidermis is often attenuated. The dermis is expanded by a dense inflammatory infiltrate consisting of large numbers of polymorphonuclear leukocytes, admixed with lymphocytes and histiocytes. The process often extends into subcutaneous fat.9 Vasodilatation may be prominent. Hemorrhage and fibrin deposition occur in the deep dermis and subcutis (Fig. 18.123). Thrombotic vascular occlusion and fibrinoid necrosis of blood vessel walls may be encountered in the deep dermis and subcutaneous fat (Fig. 18.124). A Gram stain will reveal considerable numbers of large Gram-positive bacilli predominantly in the superficial dermis (Fig. 18.125).9 The diagnosis is confirmed by culture. Serological investigations are also available. Immunohistochemical methods of detection may be used on tissue specimens.3
from Turkey and the Middle East.4–6 The mortality is low and most patients recover within 3 months.3
Cutaneous manifestations occur in approximately 6% or less of cases; however, this figure approached 14% in a series from Turkey.5,7–9 A number of cutaneous manifestations have been recorded, including a disseminated papulonodular eruption, a diffuse maculopapular rash, erythema nodosum-like subcutaneous nodules, purpura, leukocytoclastic vasculitis, erythema multiforme, urticaria-like papules and plaques, multiple abscesses, cutaneous ulcers, ecchymoses and (rarely) livedo reticularis, palmar erythema, or an even large mass mimicking a soft tissue tumor.3,5,7,8,10–17 Vasculitic skin lesions may form part of an infection-induced systemic thrombotic microangiopathy mimicking Henoch-Schönlein purpura.18,19 There is a single case report of Brucella-associated Stevens-Johnson syndrome.20 Contact brucellosis manifests with erythema or pruritus, usually on the forearm or hand. In some cases, this may progress to a follicular, vesicular, or pustular eruption.3 A rare case of contiguous skin involvement secondary to underlying Brucella chronic osteomyelitis has been recorded.21 A factitious case of brucellosis caused by autoinoculation has also been reported; the patient developed bacteremia and ulcerating cutaneous abscesses.22
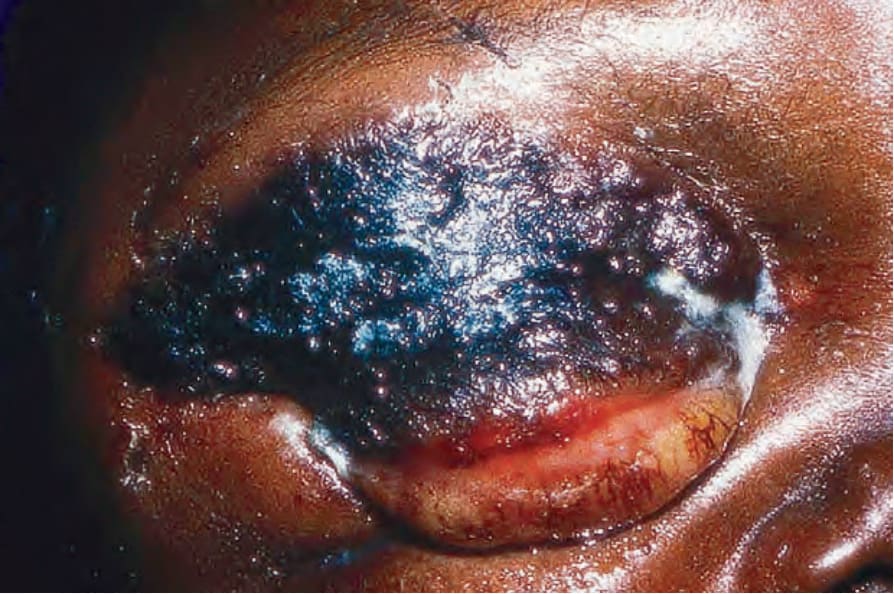
Fig. 18.120 Anthrax: cutaneous disease is the commonest manifestation in humans. This black crusted lesion is typical. By courtesy of J. Frean, MD, and the late M. Isaäcson, MD, University of Witwatersrand, Johannesburg, South Africa.
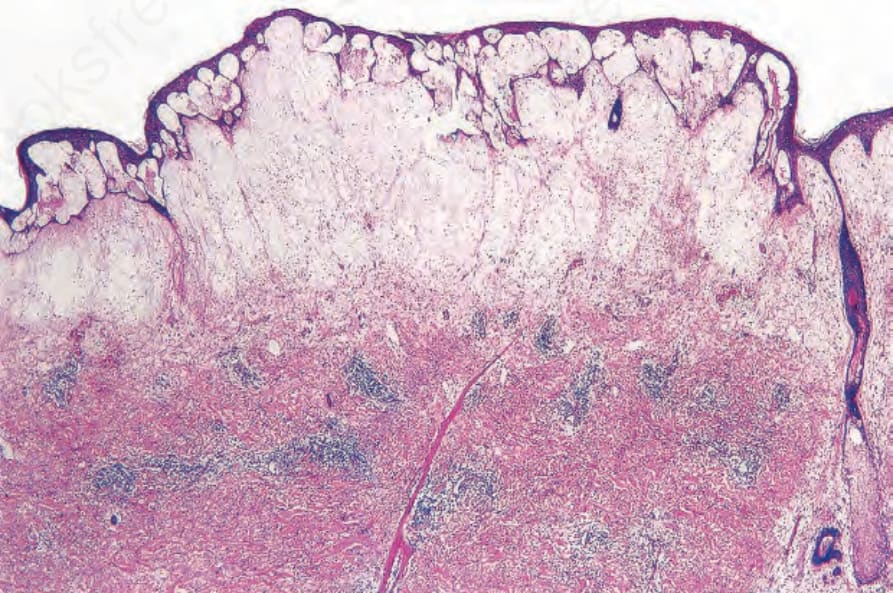
Fig. 18.122 Anthrax: there is massive subepidermal edema with subepidermal vesiculation. Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.
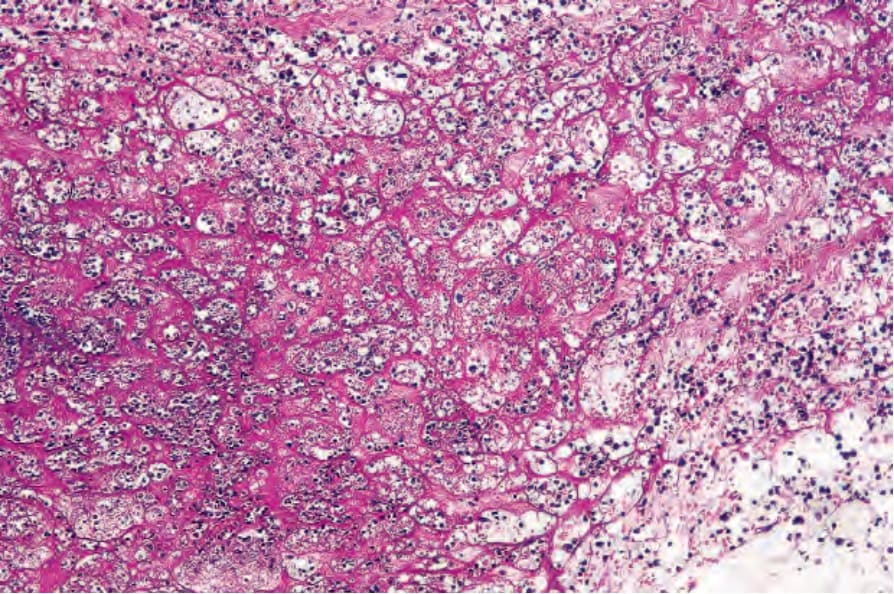
Fig. 18.123 Anthrax: marked fibrin deposition is evident. Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.
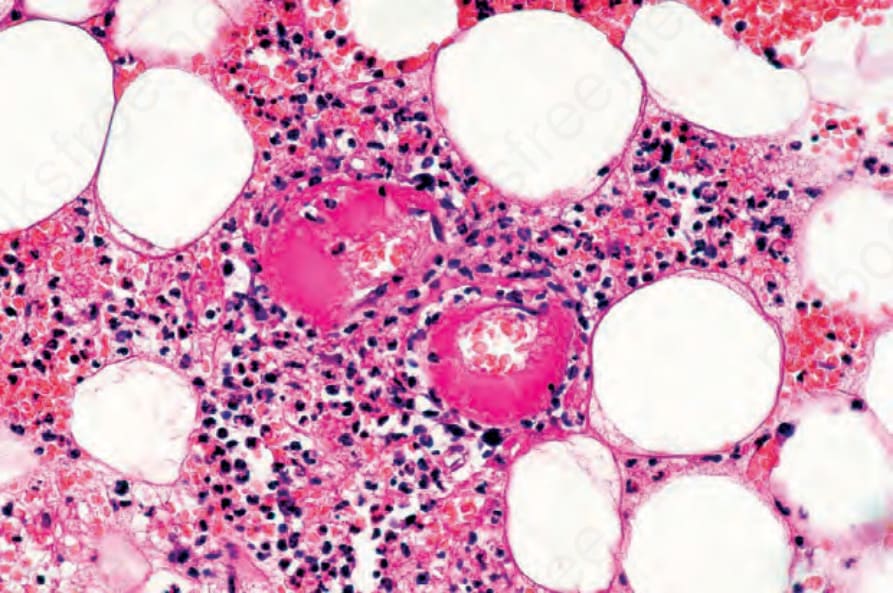
Fig. 18.124 Anthrax: thrombosed vessels are present. Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.
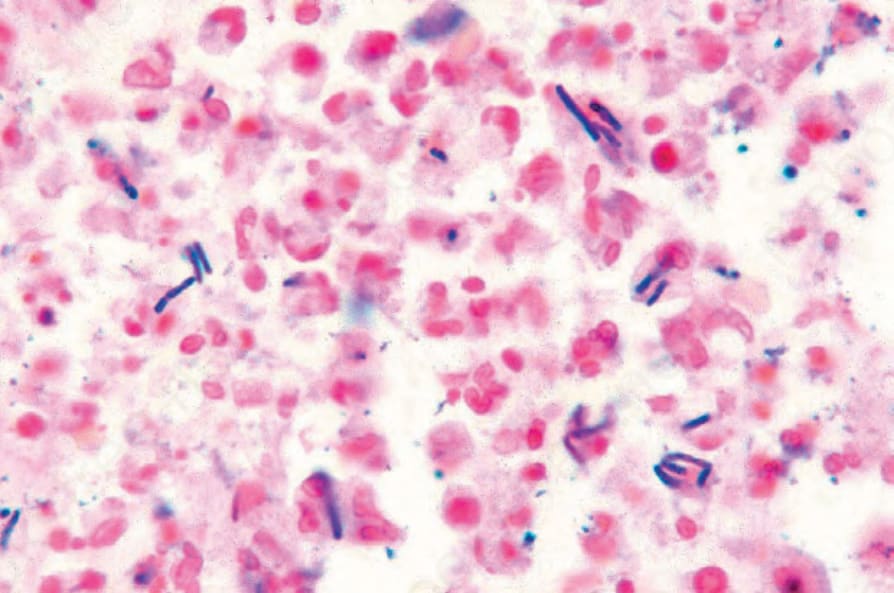
Fig. 18.125 Anthrax: numerous elongated Gram-positive bacilli are present. Reproduced with permission from Mallon E, McKee PH. Extraordinary case report: cutaneous anthrax. American Journal of Dermatopathology. 1997; 19: 79–82.