疾病定義與分類
皮膚有一群正常的共生菌 (commensal bacteria),其中以 Staphylococcus epidermidis 為主。其他常駐的革蘭氏陽性菌包括 Micrococcus spp. 與 Corynebacterium spp.。源自角質層 (stratum corneum) 與皮脂 (sebum) 的游離脂肪酸 (free fatty acids) 及其他脂質具有抗菌作用,然而正常人群中仍有 10% 至 20% 為 S. aureus 的皮膚帶菌者 (cutaneous carriers),約 10% 為 A 群 β 溶血性鏈球菌 (group A β-hemolytic streptococci, Streptococcus pyogenes) 的咽部帶菌者 (pharyngeal carriers)。此「帶菌 (carrier)」狀態可能先於宿主出現感染性病灶,或成為他人感染的來源。S. aureus 與 S. pyogenes 是皮膚淺層細菌感染最常見的致病菌,但即使是低毒力的微生物,如 S. epidermidis,在接種量 (inoculum) 足夠大或宿主免疫功能低下 (immunocompromised) 的情況下亦可致病。S. aureus 的毒素產生也是大疱性膿痂疹 (bullous impetigo)、葡萄球菌燙傷樣皮膚症候群 (staphylococcal scalded skin syndrome, SSSS) 與毒性休克症候群 (toxic shock syndrome) 的成因。
臨床特徵 (Clinical Features)
膿痂疹 (impetigo) 是最淺層的化膿性 (pyogenic, pyoderma) 細菌性皮膚感染,且傳染性極強。它極為常見,最常發生於兒童期,但也可見於老年人及免疫缺乏 (immunodeficiency) 狀態的病人。據估計,全球任一時間點有超過 1 億 6,200 萬名兒童罹患此病。兒童期的中位盛行率約為 12%。然而,疾病負擔最高者似乎是高收入國家中弱勢及邊緣化社群的兒童。膿痂疹一般可細分為非大疱性 (單純性) 膿痂疹 (nonbullous (simple) impetigo) 與大疱性膿痂疹 (bullous impetigo),通常繼發於 S. aureus 或 S. pyogenes 對輕微皮膚擦傷及昆蟲叮咬的污染。疥瘡 (scabies) 是膿痂疹的重要危險因子,尤其在兒童中。
在單純性膿痂疹 (simple impetigo) 中,病灶表現為小的淺層水疱 (vesicles),水疱迅速破裂,並被一種特徵性、附著緊密、厚而髒污的黃色痂皮所取代,周圍有紅斑邊緣 (Figs 18.92–18.94)。口、鼻及四肢特別容易受累。有時會出現局部淋巴結腫大 (regional lymphadenopathy)。單純性膿痂疹可呈地方流行性 (endemic) 或流行性 (epidemic),並常擴散至同住的手足及同學。它在溫暖、潮濕的環境中較常見。雖然 S. aureus 在北美仍是較常見的病因,而 S. pyogenes 過去在開發中國家是膿痂疹較重要的病原體,但 S. aureus 現已成為世界許多地區最常分離到的病原體。然而在某些病例中,兩種細菌似乎共存。鏈球菌性膿痂疹 (streptococcal impetigo) 偶可進展為蜂窩性組織炎 (cellulitis),或先於急性絲球體腎炎 (acute glomerulonephritis)、結節性紅斑 (erythema nodosum) 或多形性紅斑 (erythema multiforme) 出現。
大疱性膿痂疹 (bullous impetigo) 主要是葡萄球菌媒介的疾病,專一由 phage group II 的 S. aureus 引起。初期表現為直徑可達 2 cm 的淺層水疱 (Fig. 18.95)。水疱內容物起初清澈,但迅速變混濁,繼而形成一層薄的漿液膿性 (seropurulent) 痂皮;紅斑不明顯。病灶通常不侵犯黏膜。可能有輕微的全身性症狀,病灶於 2–3 週內消退。
膿瘡疹 (ecthyma) 可能是膿痂疹的一種變異型,主要發生於兒童的下肢,但也可發生於成人及其他部位 (Figs 18.96 and 18.97)。它表現為厚痂、其下為穿鑿狀潰瘍 (punched-out ulceration),並導致結痂 (scarring)。S. pyogenes 是常見病因。它在熱帶氣候較常見,於各年齡層皆可發生。輕微創傷或疥瘡 (scabies) 感染可能決定病灶的位置。細菌毒素引起的血管炎 (vasculitis) 與壞死 (necrosis) 可能決定了其不同的表現。
壞疽性膿瘡疹 (ecthyma gangrenosum) 通常是 P. aeruginosa 敗血症 (septicemia) 的併發症,發生於免疫缺乏的病人,尤其是有嗜中性球減少症 (neutropenia) 者。它也曾被報告與低丙種球蛋白血症 (hypogammaglobulinemia) 相關。亦有少數壞疽性膿瘡疹在無嗜中性球減少症或敗血症情況下發生的報告。此病也曾被報告發生於毒性表皮壞死溶解 (toxic epidermal necrolysis, TEN) 之後。病灶可為單發或多發,起初為無痛的紅斑性斑疹 (erythematous macules),後變為硬結 (indurated)、大疱性 (bullous) 或膿疱性 (pustular)。也曾描述有環形 (annular) 病灶。病灶很快變為壞疽性,並覆以特徵性的灰黑色焦痂 (eschar) 及紅斑性暈環 (erythematous halo)。病灶尤其見於臀部及會陰部以及四肢。死亡率高,特別是病灶多發者。除 P. aeruginosa 外,其他微生物也被認為與此病的演變有關。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
帶菌狀態或經由污染物體的接種,是皮膚淺層感染的必要先決條件。微生物附著於受創區域,與大量存在於滲出液中的 fibronectin、可能還有 type IV collagen 及 laminin 強力結合。微生物的先天毒力 (innate virulence) 與宿主防禦能力決定了感染後續的進展,但若細菌產生 coagulase、hyaluronidase 或 lipases,則會促進感染。引起大疱性膿痂疹的 S. aureus 屬於 serotype II,主要為 phage type 71,並產生 exfoliative toxins A 與 B;後者也參與 SSSS (見下文)。在過去十年間,社區型抗 methicillin S. aureus (community-acquired methicillin-resistant S. aureus, CA-MRSA) 已成為膿痂疹的主要病因。
膿痂疹的早期病灶以表皮在顆粒層 (stratum granulosum) 正下方出現裂隙 (split) 為特徵 (Fig. 18.98)。所形成的水疱內充滿嗜中性球 (neutrophils)、革蘭氏陽性球菌 (Gram-positive cocci),偶見棘層鬆解細胞 (acantholytic cells) (Fig. 18.99)。其下的真皮含有嗜中性球與淋巴球的混合浸潤。在水疱下方海綿狀水腫的棘層 (spongiotic stratum spinosum) 中,可見嗜中性球正自真皮遷移,作為對致病細菌的趨化反應 (chemotactic response)。在嗜中性球功能受損的情況下,膿痂疹可能更為常見且範圍更廣。
在膿瘡疹 (ecthyma) 中,可見界線清楚的潰瘍區域,伴有大量嗜中性球浸潤及其上附著的痂皮 (Fig. 18.100)。
壞疽性膿瘡疹 (ecthyma gangrenosum) 以表皮壞死 (epidermal necrosis) 伴出血及真皮梗塞 (dermal infarction) 為特徵,通常伴有由淋巴球、組織球 (histiocytes) 及嗜中性球組成的混合性發炎細胞浸潤。較少見的情況下,會發現發炎細胞稀少。革蘭氏陰性桿菌 (Gram-negative bacilli) 可見於真皮中,並侵犯小靜脈 (venules) 的中層 (media) 與外膜 (adventitia)。可能存在血管炎 (vasculitis) 與血栓 (thrombosis)。
鑑別診斷 (Differential Diagnosis)
診斷通常依臨床表現做出,並以致病微生物的培養加以佐證。少數情況下需要切片。
組織學上,本病灶可能與天疱瘡 (pemphigus) 的淺層變異型混淆,特別是因為後者可能繼發感染,且膿痂疹中也可能有少數棘層鬆解細胞 (acantholytic cells)。大疱性膿痂疹中可能呈現類似天疱瘡 (pemphigus-like) 形態的抗體,因此與落葉型天疱瘡 (pemphigus foliaceus) 的區分可能會有困難。一般而言,大量嗜中性球的存在及革蘭氏陽性球菌的辨識,已足夠特徵性以確認膿痂疹,因為棘層鬆解細胞非常稀少。組織學上也可考慮與角質下膿疱性皮膚病 (subcorneal pustular dermatosis) 及膿疱性乾癬 (pustular psoriasis) 的區分,雖然缺乏棘層肥厚 (acanthosis) 並非結論性,但應指向膿痂疹。
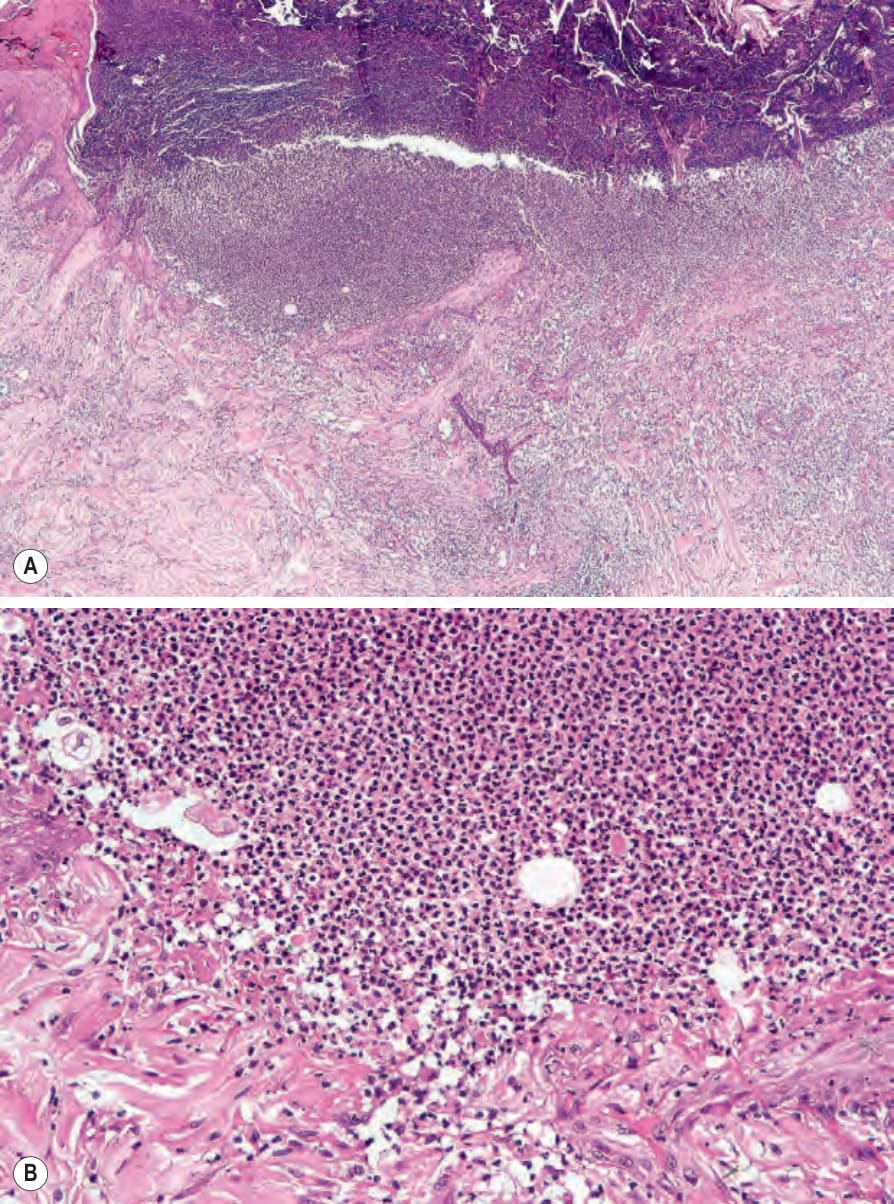
圖 18-100 (A, B):膿瘡疹 (ecthyma):可見界線清楚的潰瘍。人為假象 (artifact) 是重要的鑑別診斷。
Fig. 18.100 (A, B) Ecthyma: there is a sharply delineated ulcer. Artifact is an important differential diagnosis.

圖 18-101:葡萄球菌燙傷樣皮膚症候群 (staphylococcal scalded skin syndrome):注意極為廣泛的水疱形成。By courtesy of A. du Vivier, MD, King’s College Hospital, London, UK.
Fig. 18.101 Staphylococcal scalded skin syndrome: note the very extensive blistering. By courtesy of A. du Vivier, MD, King’s College Hospital, London, UK.

圖 18-102:葡萄球菌燙傷樣皮膚症候群 (staphylococcal scalded skin syndrome):注意廣泛的剝脫區域,其邊緣的上皮正在脫落。本病例發生於一名冠狀動脈繞道手術後傷口感染的病人。By courtesy of S. Parker, MD, West Middlesex Hospital, London, UK.
Fig. 18.102 Staphylococcal scalded skin syndrome: note the widespread denuded areas at the edge of which the epithelium is being shed. This case developed in a patient following wound infection after a coronary artery bypass. By courtesy of S. Parker, MD, West Middlesex Hospital, London, UK.
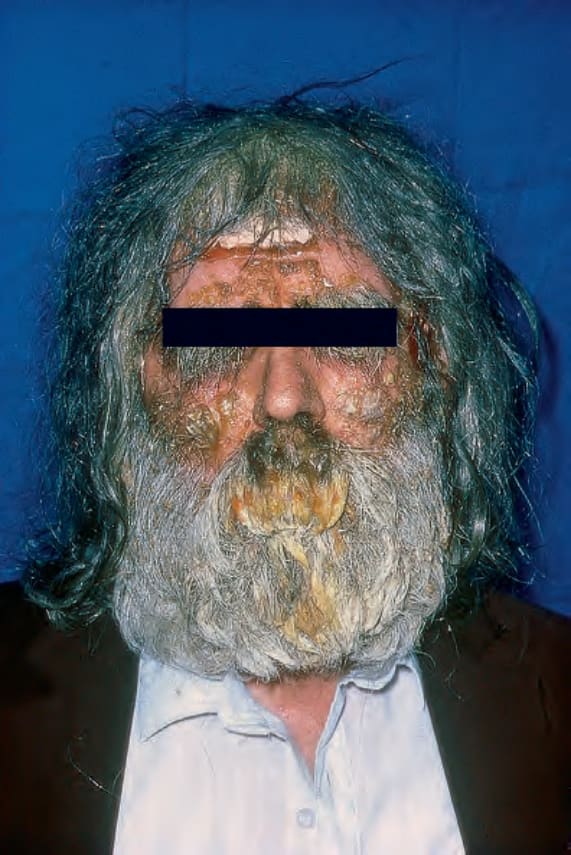
圖 18-92:膿痂疹 (impetigo):注意此病人前額與雙頰上的結痂病灶。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 18.92 Impetigo: note the crusted lesions on this patient’s forehead and cheeks. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 18-93 (A, B):膿痂疹 (impetigo):注意水疱被金黃色痂皮覆蓋。這些口周 (perioral) 病灶位於特徵性的部位。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 18.93 (A, B) Impetigo: note that the vesicles are covered by a golden crust. These perioral lesions are at a characteristic site. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 18-94:膿痂疹 (impetigo):此病人可見許多水疱。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 18.94 Impetigo: in this patient numerous vesicles are evident. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 18-95:大疱性膿痂疹 (bullous impetigo):可見一大片裸露的糜爛 (raw erosion) 及遠端一處已癒合的病灶。By courtesy of the Institute of Dermatology, London, UK.
Fig. 18.95 Bullous impetigo: there is a large raw erosion and a healed lesion distally. By courtesy of the Institute of Dermatology, London, UK.

圖 18-96:膿瘡疹 (ecthyma):(A) 處於不同演變階段的特徵性病灶;(B) 特寫顯示一處穿鑿狀潰瘍 (punched-out ulcer)。By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.
Fig. 18.96 Ecthyma: (A) characteristic lesions in varying stages of evolution; (B) a punched-out ulcer is shown in close-up. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.

圖 18-97:膿瘡疹 (ecthyma):可見多發病灶。By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
Fig. 18.97 Ecthyma: multiple lesions are present. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
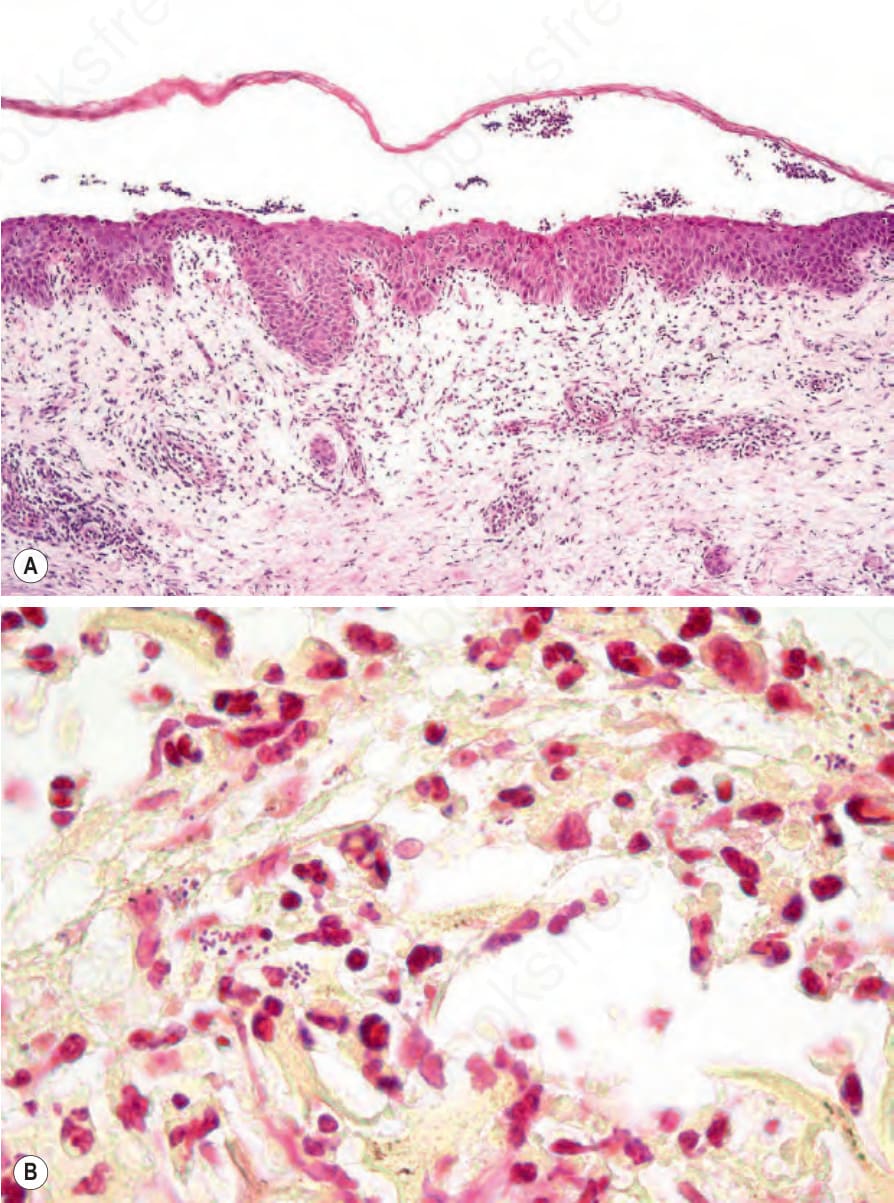
圖 18-98:大疱性膿痂疹 (bullous impetigo):(A) 裂隙部位緊位於顆粒細胞層 (granular cell layer) 正下方;(B) 可見革蘭氏陽性球菌 (Gram-positive cocci)。
Fig. 18.98 Bullous impetigo: (A) the site of cleavage is immediately below the granular cell layer; (B) Gram-positive cocci are present.
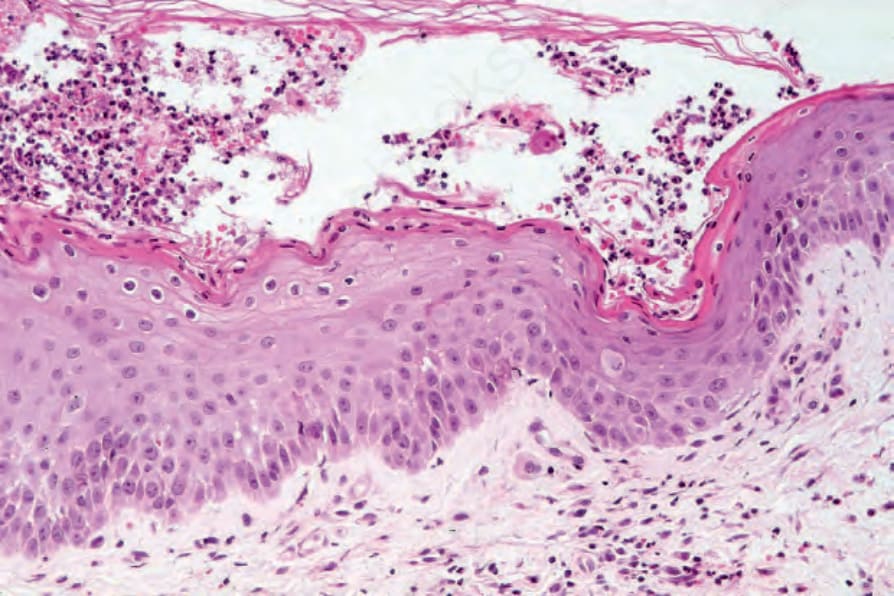
圖 18-99:大疱性膿痂疹 (bullous impetigo):除嗜中性球 (neutrophils) 外,偶可見棘層鬆解細胞 (acantholytic cells),造成與落葉型天疱瘡 (pemphigus foliaceus) 的診斷混淆。
Fig. 18.99 Bullous impetigo: in addition to neutrophils, occasional acantholytic cells may be present causing diagnostic confusion with pemphigus foliaceus.