Impetigo
Impetigo
The skin has a normal commensal population of bacteria in which Staphylococcus epidermidis predominates.1 Other resident Gram-positive bacteria include Micrococcus spp. and Corynebacterium spp.2 The free fatty acids and other lipids derived from the stratum corneum and sebum have an antibacterial role, yet 10% to 20% of the normal population are cutaneous carriers of S. aureus and approximately 10% are pharyngeal carriers of group A β-hemolytic streptococci (Streptococcus pyogenes).1,3 This ‘carrier’ state may precede infective lesions in the host or may be the origin of infections in others. S. aureus and S. pyogenes are the most common agents in superficial bacterial infections of the skin, but even organisms of low virulence, such as S. epidermidis, can become pathogenic with a sufficiently large inoculum or in an immunocompromised host.1 S. aureus toxin production is also responsible for bullous impetigo, the staphylococcal scalded skin syndrome (SSSS), and the toxic shock syndrome.4,5
Clinical features Impetigo is the most superficial pyogenic (pyoderma) bacterial skin infection and is highly infectious. It is exceedingly common and occurs most often in childhood, but may be seen in the elderly and in patients with immunodeficiency states. It is estimated that more than 162 million children worldwide suffer from this condition at any given time. The median childhood prevalence is around 12%. The highest disease burden, however, appears to be among underprivileged children from marginalized communities in high-income countries.6 Impetigo is typically subdivided into nonbullous (simple) impetigo and bullous impetigo and usually follows the contamination of minor skin abrasions and insect bites by S. aureus or S. pyogenes.7,8 Scabies is an important risk factor for impetigo, especially among children.6,9
In simple impetigo, the lesions present as small superficial vesicles, which rapidly burst and are replaced by a characteristic, adherent, thick yellowish dirty crust with a margin of erythema (Figs 18.92–18.94). The mouth, nose, and extremities are particularly affected. Regional lymphadenopathy
is sometimes present. Simple impetigo may occur in endemic or epidemic form and often spreads to involve siblings and schoolmates. It is seen more often in warm, humid conditions.10,11 Although S. aureus remains the more frequent cause in North America and S. pyogenes was the more important etiological agent of impetigo in developing countries in the past, S. aureus is now the most commonly isolated pathogen in many parts of the world.12,13 In some cases, however, the two bacteria appear to coexist. Streptococcal impetigo may occasionally progress to cellulitis or precede acute glomerulonephritis, erythema nodosum, or erythema multiforme.
859 Impetigo
is not marked. The lesions do not usually involve mucosae. There may be mild constitutional symptoms, and the lesions resolve in 2–3 weeks.
Ecthyma is probably a variant of impetigo and occurs predominantly on the lower limbs of children, but may occur in adults and at other sites (Figs 18.96 and 18.97).14,15 It presents with thick crusting, overlying punched-out ulceration, and resultant scarring. S. pyogenes is the usual cause. It is more common in tropical climates, where it occurs in all age groups. Minor trauma or scabies infestation may determine the site of the lesions. It is possible that vasculitis and necrosis induced by bacterial toxins determine the different presentation.
Bullous impetigo is primarily a staphylococcal-mediated disease exclusively due to phage group II S. aureus.10 Superficial blisters up to 2 cm across are the initial features (Fig. 18.95). The contents are at first clear, but rapidly become cloudy and then develop a thin seropurulent crust; erythema
Ecthyma gangrenosum is usually a complication of P. aeruginosa septicemia that occurs in immunodeficient patients, particularly those with a neutropenia.16,17 It has also been reported in association with
A
B
860 Infectious diseases of the skin
hypogammaglobulinemia.18 There have been rare reports of ecthyma gangrenosum occurring in the absence of neutropenia or septicemia.19–21 The condition has also been reported following toxic epidermal necrolysis (TEN).22 Lesions, which may be single or multiple, begin as painless erythematous macules that become indurated, bullous, or pustular.16 Annular lesions have been described.23 The lesions soon become gangrenous and covered by a characteristic gray-black eschar and erythematous halo. Lesions are especially seen on the gluteal and perineal regions and on the limbs.16 The mortality is high, particularly in those with multiple lesions. Organisms other than P. aeruginosa have been implicated in the evolution of the disease.24
attached to the traumatized area, binding strongly to fibronectin and possibly type IV collagen and laminin, which are abundant in the exudate.1,10 The innate virulence of the organisms and the host defense capability determine the subsequent progress of the infection, but this is facilitated if the bacteria produce coagulase, hyaluronidase, or lipases.1 The form of S. aureus responsible for bullous impetigo is of serotype II and mainly of phage type
Pathogenesis and histologic features The carrier state or inoculation by a contaminated object is a necessary precondition to superficial infection of the skin. The organisms become
A
B
861 Impetigo
A
B
71 and produces exfoliative toxins A and B; the latter are also involved in the SSSS (see below).4,5,25,26 During the past decade, community-acquired methicillin-resistant S. aureus (CA-MRSA) emerged as a major cause of impetigo.12,13,27–29
An early lesion of impetigo is characterized by a split in the epidermis just beneath the stratum granulosum (Fig. 18.98). The resultant vesicle becomes filled with neutrophils, Gram-positive cocci, and occasional acantholytic cells (Fig. 18.99). The underlying dermis contains a mixed neutrophil and lymphocyte infiltrate. Neutrophils may be seen in the spongiotic stratum spinosum beneath the vesicle in the process of migrating from the dermis as a chemotactic response to the causative bacteria. In conditions of impaired neutrophil function, impetigo may be common and more extensive.1
A
In echthyma, there is a sharply circumscribed area of ulceration with a heavy neutrophil infiltrate and overlying adherent crust (Fig. 18.100).
Ecthyma gangrenosum is characterized by epidermal necrosis with hemorrhage and dermal infarction, usually accompanied by a mixed inflammatory cell infiltrate of lymphocytes, histiocytes, and neutrophils.16 Less commonly, a dearth of inflammatory cells is noted.16,30 Gram-negative bacilli may be seen in the dermis and involving the media and adventitia of venules.16 Vasculitis and thrombosis may be present.
Differential diagnosis The diagnosis is usually made on clinical grounds and supported by culture of the causative organisms. Rarely, a biopsy is necessary.
The lesion may be confused histologically with a superficial variant of pemphigus, particularly as the latter can become secondarily infected
B
862 Infectious diseases of the skin
and there may be a few acantholytic cells in impetigo. Antibodies in a pemphigus-like pattern may be demonstrated in bullous impetigo and distinction from pemphigus foliaceus may therefore be a problem.5,31,32 Generally, the presence of numerous neutrophils and the recognition of Gram-positive cocci is sufficiently characteristic to confirm impetigo, as acantholytic cells are very scanty. Distinction from subcorneal pustular dermatosis and pustular psoriasis may be considered histologically, but the lack of acanthosis, although not conclusive, should point toward impetigo.
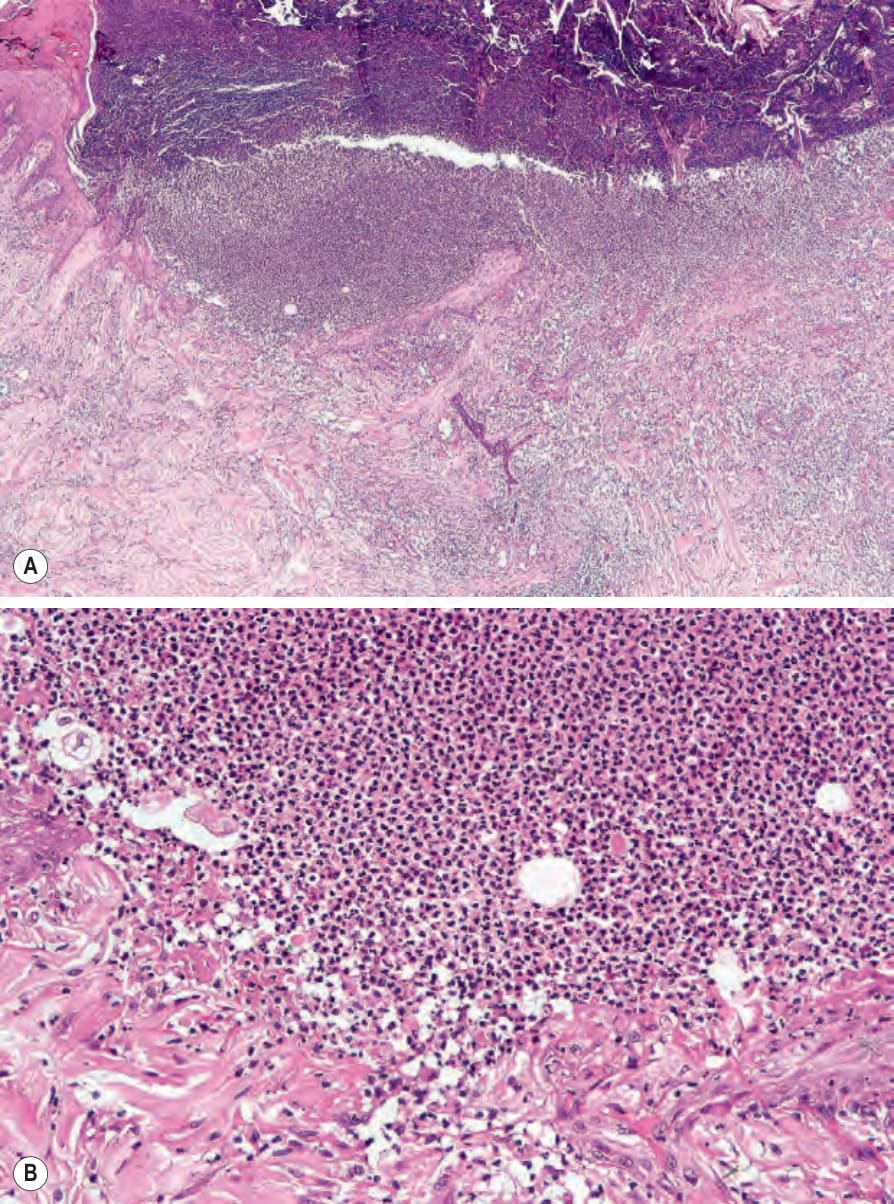
Fig. 18.100 (A, B) Ecthyma: there is a sharply delineated ulcer. Artifact is an important differential diagnosis.

Fig. 18.101 Staphylococcal scalded skin syndrome: note the very extensive blistering. By courtesy of A. du Vivier, MD, King’s College Hospital, London, UK.

Fig. 18.102 Staphylococcal scalded skin syndrome: note the widespread denuded areas at the edge of which the epithelium is being shed. This case developed in a patient following wound infection after a coronary artery bypass. By courtesy of S. Parker, MD, West Middlesex Hospital, London, UK.
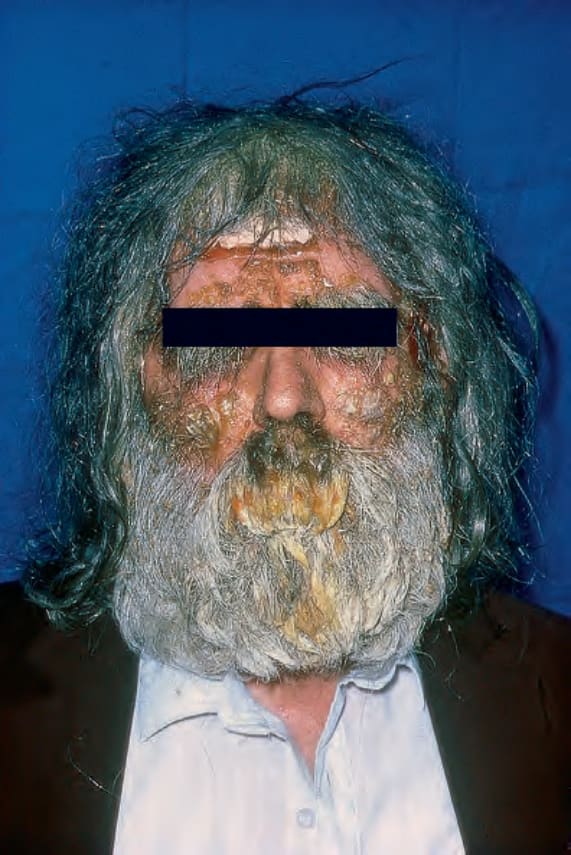
Fig. 18.92 Impetigo: note the crusted lesions on this patient’s forehead and cheeks. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 18.93 (A, B) Impetigo: note that the vesicles are covered by a golden crust. These perioral lesions are at a characteristic site. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 18.94 Impetigo: in this patient numerous vesicles are evident. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 18.95 Bullous impetigo: there is a large raw erosion and a healed lesion distally. By courtesy of the Institute of Dermatology, London, UK.

Fig. 18.96 Ecthyma: (A) characteristic lesions in varying stages of evolution; (B) a punched-out ulcer is shown in close-up. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.

Fig. 18.97 Ecthyma: multiple lesions are present. By courtesy of N.C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa.
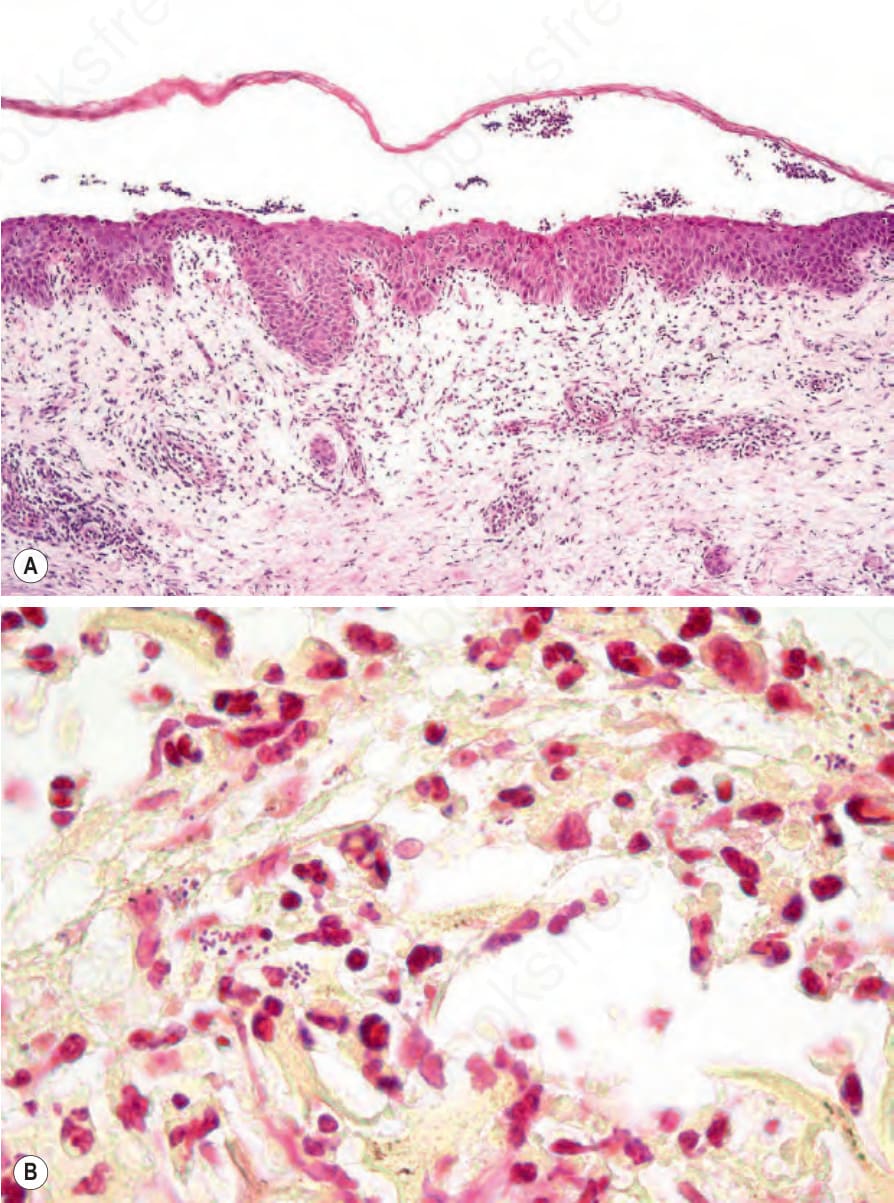
Fig. 18.98 Bullous impetigo: (A) the site of cleavage is immediately below the granular cell layer; (B) Gram-positive cocci are present.
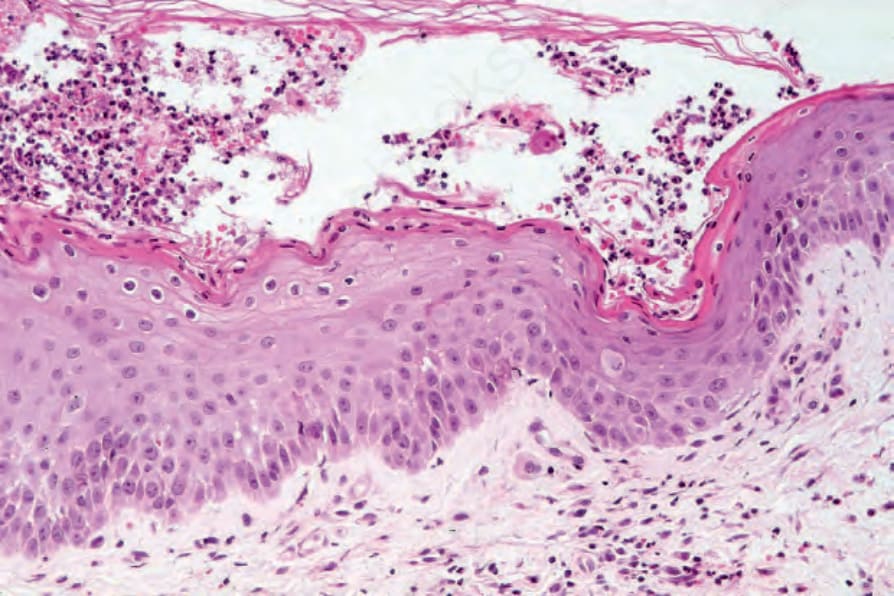
Fig. 18.99 Bullous impetigo: in addition to neutrophils, occasional acantholytic cells may be present causing diagnostic confusion with pemphigus foliaceus.