臨床特徵 (Clinical Features)
- 蟠尾絲蟲病 (onchocerciasis,又稱河盲症 river blindness) 流行於約 37 個國家,估計有 1 億 8,700 萬人面臨感染風險。雖然這些國家絕大多數位於熱帶非洲部分地區(99% 的高風險族群居住於此),本病亦發生於葉門 (Yemen),並曾在中美洲與南美洲的六個國家有過記錄。雖然透過大規模投予微絲蟲殺蟲劑 (microfilaricide) ivermectin,已在美洲地區(包括瓜地馬拉 Guatemala,當地近期已證實消除蟠尾絲蟲病)達成相當的疾病防治成果,但儘管自 1995 年起已在約 16 個撒哈拉以南非洲國家施行 ivermectin 的大規模治療計畫,本病的根除仍尚未達成。據認超過 2,700 萬人遭受感染。對疾病負擔的近期估計顯示,2015 年因本病主要相關的併發症(即失明、嚴重視力障礙,以及表現為惱人搔癢與毀容性皮膚病灶的皮膚侵犯)而損失了 110 萬個失能調整生命年 (disability-adjusted life-years)。目前皮膚侵犯似乎已成為疾病負擔的主要貢獻來源,而非眼部疾病。
- 蟠尾絲蟲病大多數症狀與絲蟲性線蟲 (filarial nematode) Onchocerca volvulus 的微絲蟲 (microfilarial) 期相關。蟠尾絲蟲病特別好發於居住在水流湍急河川附近的個體。在罕見情況下,人類可能感染人畜共通 (zoonotic) 的 Onchocerca 物種,尤其是 O. lupi。後者的病例曾在歐洲、突尼西亞 (Tunisia)、土耳其 (Turkey)、伊朗 (Iran) 與美國有過記錄。微絲蟲會遷移至皮膚與其他器官,引起搔癢以及呈現色素變化的斑疹 (macules)。搔抓會導致表皮剝脫 (excoriation),有時造成續發性感染。在嚴重病例中,隨後會出現真皮增厚、水腫與皮膚皺褶。鱗屑與脫色 (depigmentation) 分別稱為蜥蜴皮 (lizard skin) 與豹皮 (leopard skin) (Fig. 18.391)。淋巴結常受侵犯,加劇水腫的問題。成蟲存在於真皮結節 (dermal nodules) 中,常與疤痕組織相關;這些結節可移動且有壓痛,通常見於骨性突起 (bony prominences) 上方。
- 皮膚的臨床表現已被分類為數個類別,包括急性丘疹型蟠尾皮膚炎 (acute papular onchodermatitis)、慢性丘疹型蟠尾皮膚炎 (chronic papular onchodermatitis)、苔癬化蟠尾皮膚炎 (lichenified onchodermatitis)、萎縮 (atrophy) 與脫色 (depigmentation) (Figs 18.392–18.395)。其他公認的表現包括可觸及的蟠尾絲蟲結節 (palpable onchocercal nodules)、淋巴結病變 (lymphadenopathy)、垂腹股溝 (hanging groin) 與淋巴水腫 (lymphedema)。在流行地區,30% 或更多的人口可能有蟠尾絲蟲性皮膚病灶;在某些超高度流行 (hyperendemic) 的社區,此數字接近 60%。多變的臨床特徵被認為反映了宿主對真皮中微絲蟲存在所產生的不同免疫反應。遷移的微絲蟲可進入眼睛並造成河盲症。眼部病灶為主要的併發症來源,包括點狀角膜炎 (punctate keratitis)、硬化性角膜炎 (sclerosing keratitis)、虹膜炎 (iritis)、脈絡膜視網膜炎 (chorioretinitis) 與視神經萎縮 (optic atrophy)。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- O. volvulus 在鄉村地區藉由雌性黑蠅 (black flies, Simulium) 的叮咬,以其幼蟲 (larval) 型態傳播給人類。幼蟲在深部真皮中發育為成蟲。微絲蟲由妊娠中的雌蟲產出,並可遷移遍布整個宿主 (Fig. 18.396)。大多數微絲蟲存在於淺層真皮,並可藉由「皮膚切片 (skin snips)」的組織學檢查加以辨識。成熟雌蟲長度可達 50 cm,直徑可達 0.45 mm,並以複雜的盤繞型態存在於固定結節中。微絲蟲為 220–360 × 5–9 µm。這些結節(有時被稱為「蟠尾絲蟲瘤 onchocercomas」)內含數條交纏的蟲體,周圍伴隨可能為化膿性 (suppurative) 或肉芽腫性 (granulomatous) 的發炎 (Figs 18.397 and 18.398)。
- 可見廣泛的纖維化 (fibrosis),常有鈣化 (calcification),有時甚至骨化 (ossification)。微絲蟲可見游離於真皮內,亦見於淋巴管中。皮膚顯示過度角化 (hyperkeratosis) 與角化不全 (parakeratosis),伴隨棘層肥厚 (acanthosis) 與真皮中的噬黑素細胞 (melanophages),但僅有輕度的淋巴球與嗜酸性球發炎浸潤。纖維化變得顯著,導致乳頭層真皮的玻璃樣變 (hyalinization)。黏液 (mucin) 在膠原束之間相當明顯,偶可見類纖維蛋白變化 (fibrinoid change) 的病灶。微絲蟲的退化以嗜酸性變化 (eosinophilic change) 伴隨細胞核碎裂為前兆;這些變化伴隨大量嗜酸性球的浸潤。
- Wolbachia 已被視為一個新穎的治療標靶,諸如 doxycycline 等藥物已被選定為未來治療蟠尾絲蟲病的潛在用藥。

圖 18-391:蟠尾絲蟲病 (onchocerciasis):豹皮 (leopard skin)。可見眾多脫色斑疹 (depigmented macules)。罕見情況下,這些斑疹會搔癢。By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.
Fig. 18.391 Onchocerciasis: leopard skin. There are numerous depigmented macules. Rarely, these are pruritic. By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.

圖 18-392:急性丘疹型蟠尾皮膚炎 (acute papular onchodermatitis):背部與上臂可見眾多小丘疹。有時可能出現水疱化 (vesiculation) 與膿疱化 (pustulation)。By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.
Fig. 18.392 Acute papular onchodermatitis: numerous small papules are present on the back and upper arm. Vesiculation and pustulation may sometimes be present. By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.

圖 18-393:慢性丘疹型蟠尾皮膚炎 (chronic papular onchodermatitis):臀部可見眾多扁平頂的斑疹與丘疹 (flat-topped macules and papules)。By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.
Fig. 18.393 Chronic papular onchodermatitis: numerous flat-topped macules and papules are present on the buttocks. By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.

圖 18-394:苔癬化蟠尾皮膚炎 (lichenified onchodermatitis):此變異型最常侵犯青少年與年輕成人。可見顯著的過度角化 (hyperkeratosis) 伴隨融合性斑塊。淋巴結病變 (lymphadenopathy) 常為其特徵。By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.
Fig. 18.394 Lichenified onchodermatitis: this variant most often affects teenagers and young adults. There is marked hyperkeratosis associated with confluent plaques. Lymphadenopathy is often a feature. By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.

圖 18-395:慢性蟠尾絲蟲病 (chronic onchocerciasis):腹股溝區域出現多餘的皮膚皺褶是一種晚期表現(晚期垂腹股溝 late hanging groin)。By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.
Fig. 18.395 Chronic onchocerciasis: the presence of redundant folds of skin in the inguinal region is a late manifestation (late hanging groin). By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.
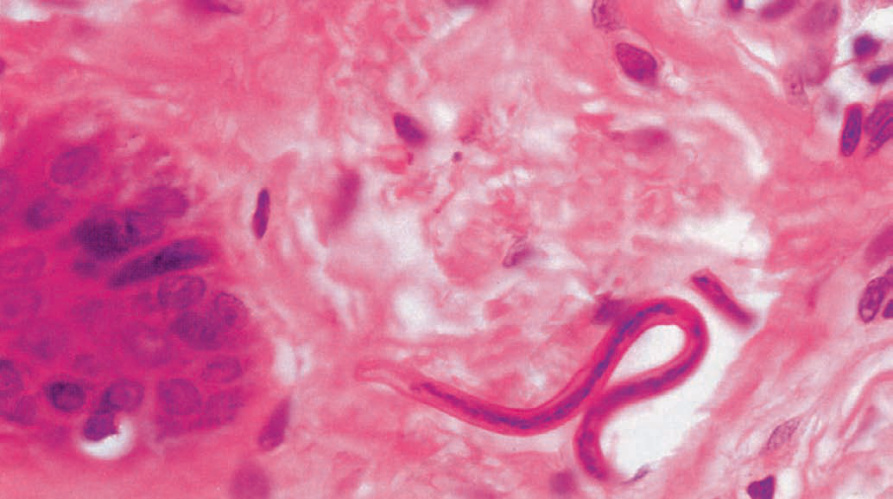
圖 18-396:蟠尾絲蟲病 (onchocerciasis):真皮中的微絲蟲 (microfilariae) 可引發淋巴組織球性浸潤 (lymphohistiocytic infiltrate),嗜酸性球 (eosinophils) 可能相當顯著。By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
Fig. 18.396 Onchocerciasis: microfilariae in the dermis may elicit a lymphohistiocytic infiltrate and eosinophils may be conspicuous. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
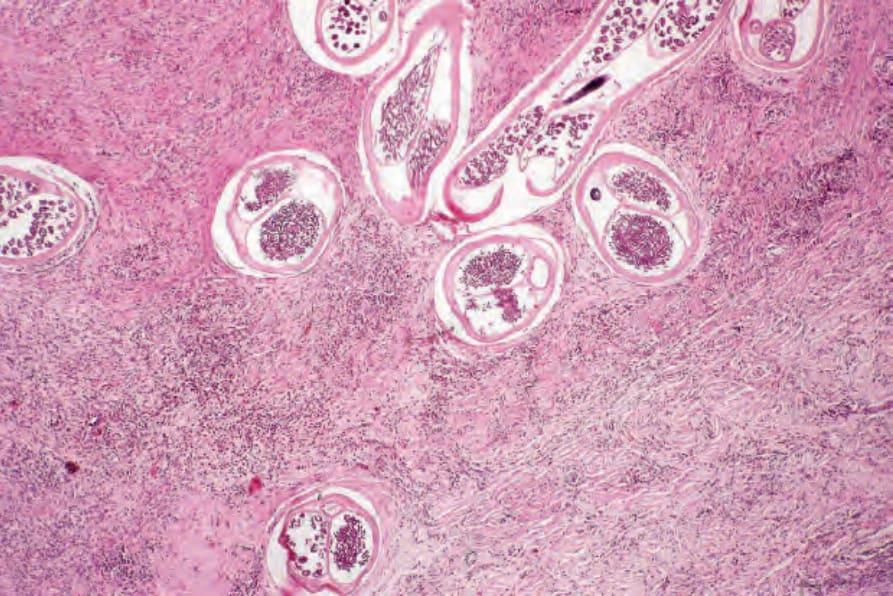
圖 18-397:蟠尾絲蟲病 (onchocerciasis):可見成蟲 (adult worm) 的多個切面。
Fig. 18.397 Onchocerciasis: multiple sections of adult worm are evident.
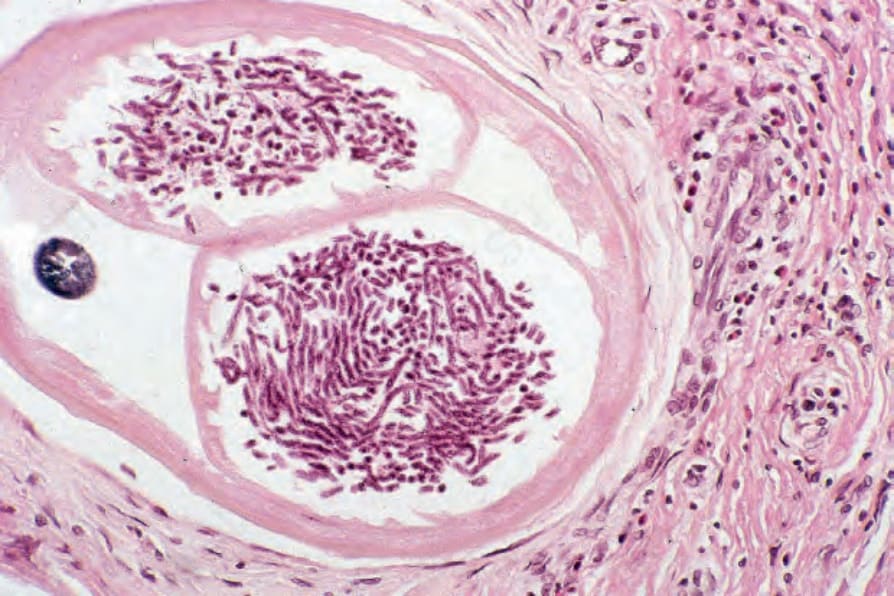
圖 18-398:蟠尾絲蟲病 (onchocerciasis):可見眾多發育中的微絲蟲 (developing microfilariae)。
Fig. 18.398 Onchocerciasis: numerous developing microfilariae are evident.