Onchocerciasis
Onchocerciasis
Clinical features
Onchocerciasis (river blindness) is endemic in some 37 countries, with an estimated 187 million people at risk of infection. Although the vast majority of these countries are in parts of tropical Africa (where 99% of the at-risk population live), the disease also occurs in the Yemen and has been recorded in six countries in Central and South America.1–7 Much success has been achieved toward disease control through the mass administration of the microfilaricide ivermectin in the Americas, including Guatemala, where the elimination of onchocerciasis was recently verified.7,8 Although a mass treatment program with ivermectin has been in place in some 16 sub-Saharan African countries since 1995, eradication of the disease has not yet been accomplished.2,9 More than 27 million people are thought to be infected.10 Recent estimates of the burden of the disease suggest that 1.1 million disability-adjusted life-years were lost in 2015 as a result of the disease’s major associated morbidities, namely, blindness, severe visual impairment, and cutaneous involvement in the form of troublesome pruritus and disfiguring skin lesions.2,6 Skin involvement now appears to be the major contributor to the disease burden, rather than ocular disease.9
Tunisia, Turkey, Iran, and the United States.13,14 The microfilariae migrate to the skin and other organs, causing itching and macules showing altered pigmentation.5,10 Scratching results in excoriation and sometimes secondary infection. Dermal thickening, edema, and wrinkling of the skin follow in severe cases. Scaling and depigmentation are termed lizard and leopard skin, respectively (Fig. 18.391). Lymph nodes often become involved, exacerbating the problems of edema. Adult worms exist in dermal nodules, often associated with scar tissue; these nodules are mobile and tender, and are usually seen over bony prominences.10,15
The clinical cutaneous manifestations have been classified into a number of categories including acute papular onchodermatitis, chronic papular onchodermatitis, lichenified onchodermatitis, atrophy, and depigmentation (Figs 18.392–18.395).10,11 Other recognized manifestations include palpable onchocercal nodules, lymphadenopathy, hanging groin, and lymphedema. In endemic areas, 30% or more of the population may have onchocercal skin lesions; this figure approaches 60% in some hyperendemic communities.4 The varying clinical features are believed to reflect variable host immune reactions to the presence of the microfilariae in the dermis.16 The migrating microfilariae can enter the eyes and cause river blindness. Ocular lesions, which are a cause of major morbidity, include punctate keratitis, sclerosing keratitis, iritis, chorioretinitis, and optic atrophy.17,18
Most symptoms of onchocerciasis are associated with the microfilarial stage of the filarial nematode Onchocerca volvulus. Onchocerciasis particularly affects individuals living close to fast-flowing rivers.11 Exceptionally, humans may be infected with zoonotic species of Onchocerca, and O. lupi in particular.12–14 Cases of the latter have been documented in Europe,
Pathogenesis and histologic features O. volvulus is transmitted in its larval form to man in rural areas by the bite of female black flies (Simulium).3,5,10,19 The larvae develop into adult worms in the deep dermis. Microfilariae are produced by gravid females and these can migrate throughout the host (Fig. 18.396). Most are present in
970 Infectious diseases of the skin
the superficial dermis, and may be identified by the histologic examination of ‘skin snips’.5,10 The adult female worm is up to 50 cm in length, with a diameter of up to 0.45 mm, and is found in complex coils in the fixed nodules. The microfilariae are 220–360 × 5–9 µm. The nodules (sometimes referred to as ‘onchocercomas’) contain several entwined worms within
surrounding inflammation, which may be suppurative or granulomatous (Figs 18.397 and 18.398).
There is extensive fibrosis, often calcification, and sometimes ossification. Microfilariae may be seen free within the dermis and also in lymphatics. The skin shows hyperkeratosis and parakeratosis, with acanthosis and melanophages in the dermis, but only a mild lymphocytic and eosinophilic inflammatory infiltrate. Fibrosis becomes prominent, resulting in hyalinization of the papillary dermis. Mucin is prominent between collagen bundles, and foci of fibrinoid change are occasionally seen. Degeneration of microfilariae is foreshadowed by an eosinophilic change with fragmentation of the nuclei; these changes are accompanied by an intense infiltrate of eosinophils.
971 Cutaneous larva migrans
novel therapeutic target, with drugs such as doxycycline earmarked for the potential treatment of onchocerciasis in the future.5,23,24

Fig. 18.391 Onchocerciasis: leopard skin. There are numerous depigmented macules. Rarely, these are pruritic. By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.

Fig. 18.392 Acute papular onchodermatitis: numerous small papules are present on the back and upper arm. Vesiculation and pustulation may sometimes be present. By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.

Fig. 18.393 Chronic papular onchodermatitis: numerous flat-topped macules and papules are present on the buttocks. By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.

Fig. 18.394 Lichenified onchodermatitis: this variant most often affects teenagers and young adults. There is marked hyperkeratosis associated with confluent plaques. Lymphadenopathy is often a feature. By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.

Fig. 18.395 Chronic onchocerciasis: the presence of redundant folds of skin in the inguinal region is a late manifestation (late hanging groin). By courtesy of M.E. Murdoch, MD, Watford Hospital, Watford, UK.
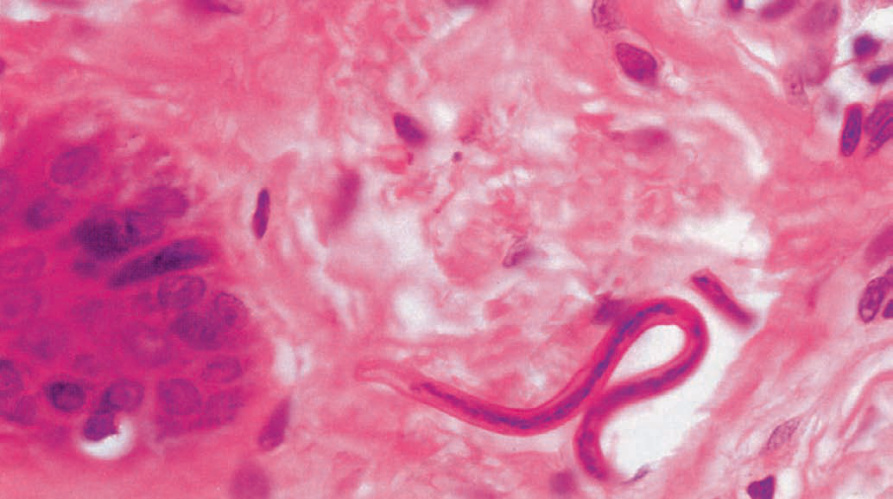
Fig. 18.396 Onchocerciasis: microfilariae in the dermis may elicit a lymphohistiocytic infiltrate and eosinophils may be conspicuous. By courtesy of S. Lucas, MD, St Thomas’ Hospital, London, UK.
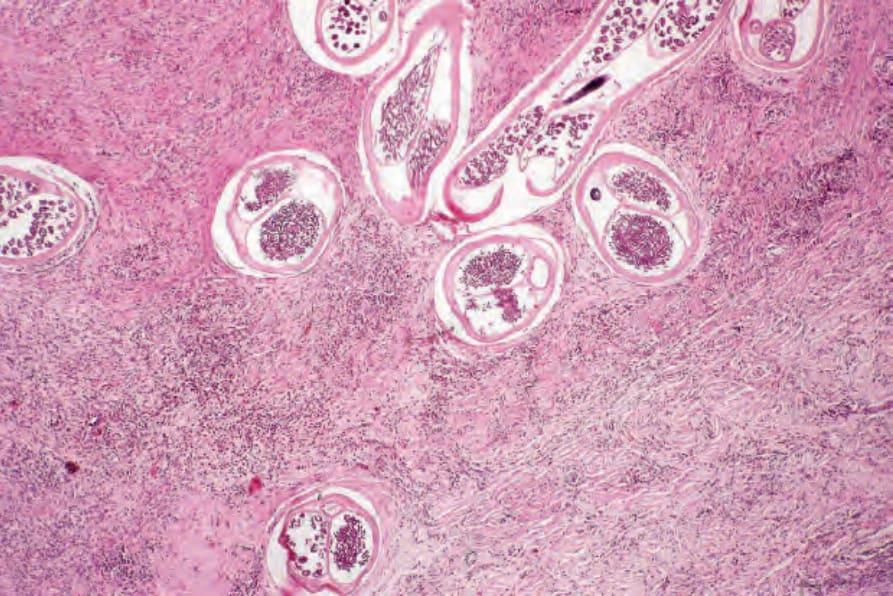
Fig. 18.397 Onchocerciasis: multiple sections of adult worm are evident.
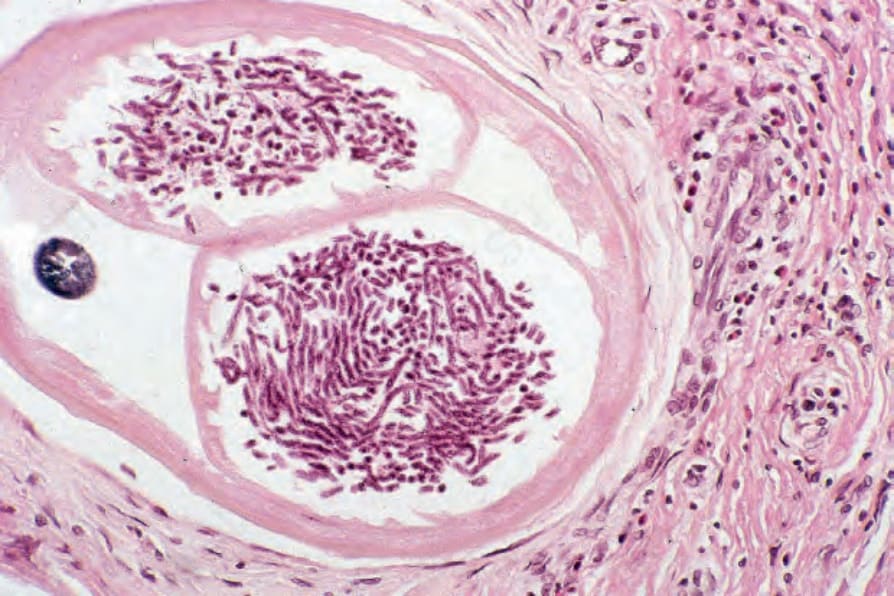
Fig. 18.398 Onchocerciasis: numerous developing microfilariae are evident.