類網狀血管病變與白色萎縮 (Livedoid Vasculopathy and Atrophie Blanche)
臨床特徵 (Clinical Features)
- 類網狀血管病變與白色萎縮 (livedoid vasculopathy and atrophie blanche)(亦稱 livedo vasculitis、livedoid vasculitis 與 segmental hyalinizing vasculitis)傳統上一直被交替使用。這是一種常見的皮膚病,通常發生於年輕至中年女性。
- 然而,有人主張:livedoid vasculopathy 一詞應用以描述該疾病本體,而 atrophie blanche 應作為某種臨床表現型態的描述,此型態雖常與 livedoid vasculopathy 相關,但並非必然相伴。
- 除了與屬於血栓性血管病變 (thrombotic vasculopathy) 的 livedoid vasculopathy 相關之外,atrophie blanche 的變化亦可見於慢性靜脈功能不全 (chronic venous insufficiency)。
- 在病程早期,病人可能表現為疼痛的紫斑性丘疹與斑塊,並進展為潰瘍。在其完全確立的狀態下,病灶可發展為 atrophie blanche,由一個或多個不規則、平滑、萎縮性斑塊組成,周圍被一圈色素過度沉著的邊緣與微血管擴張 (telangiectases) 所環繞(圖 16.110 與 16.111)。可能在其之前出現的潰瘍性病灶有兩型:
- 小型(直徑 1–5 mm)、極為疼痛的紅斑性紫斑區域,會潰瘍並緩慢癒合;
- 慢性的大面積潰瘍,直徑可達 5 cm,在經過一段長時間後,癒合形成廣泛的萎縮性斑塊區域。
- 此病呈季節性變化,典型上於夏季月份惡化。病灶以週期性間隔復發,主要位於小腿、踝部與足背表面。然而偶爾也可見於前臂、手指與手部周圍,甚至呈更廣泛的分布。Atrophie blanche 的臨床表現常與靜脈鬱滯 (venous stasis) 的徵象相關。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
-
Livedoid vasculopathy 的致病機轉尚未完全明瞭,但顯然是一種導致缺血的血栓性血管病變 (thrombotic vasculopathy)。鑑於其好發於下肢遠端,以及在某些病例中與靜脈功能不全的關聯,靜水壓 (hydrostatic pressure) 必然對其發生有所貢獻。
-
血管壁內存在免疫球蛋白(通常為 IgM,較少為 IgG 與 IgA)與補體 (complement),使某些病例存在免疫學致病機轉的可能性。本病曾被認為與組織纖溶酶原活化劑 (tissue plasminogen activator) 的局部缺陷有關。
-
病灶的位置提示外傷 (trauma) 在某些病灶的發生中可能也扮演某種角色。如前所述,許多病例與凝血障礙 (disorders of coagulation) 相關,提示其根本基礎為潛在的凝血病 (coagulopathy)。
-
脂蛋白(a) (lipoprotein(a)) 濃度升高與 livedoid vasculopathy 相關,並可能也對促血栓狀態 (prothrombotic state) 有所貢獻。
-
早期與潰瘍性病灶的特徵為:真皮血管數目增加,其管壁內含有纖維蛋白 (fibrin),此外管腔內並有纖維蛋白樣栓子 (fibrinoid plugs)(圖 16.112–16.114)。後者典型上具有抗澱粉酶 (diastase resistant) 與過碘酸希夫染色 (periodic acid-Schiff, PAS) 陽性的特性,亦可用磷鎢酸–蘇木精染色 (phosphotungstic acid–hematoxylin stain) 加以凸顯(圖 16.115)。
-
然而,血管的發炎性破壞並非本病的特徵,因此此疾病並非真正的血管炎 (vasculitis)。可見不同程度的紅血球外滲 (red cell extravasation),且常存在含鐵血黃素 (hemosiderin) 色素。通常可發現程度不一的血管周圍淋巴組織球浸潤 (perivascular lymphohistiocytic infiltrate),且真皮肥大細胞 (mast cells) 數目常增加。潰瘍性病灶顯示淺層真皮與表皮的梗塞 (infarction)。在完全確立的萎縮性斑塊中,除了血管變化外,表皮呈萎縮,真皮則顯示緻密的硬皮病樣瘢痕 (scleroderma-like scarring)。
-
約半數受累病人有凝血異常,包括 factor V Leiden 突變、protein C 或 protein S 活性降低、prothrombin G20210A 突變、anticardiolipin antibodies、homocysteinemia、lupus anticoagulant、cryoglobulinemia 與 methylenetetrahydrofolate reductase 突變。一項研究發現 17% 的 lupus 病人受到影響。該研究亦指出皮膚病灶的型態有些不尋常,侵犯膝部、肘部、手指、足底與背部。同一研究提示患有 atrophie blanche 的 lupus erythematosus 病人,發生 lupus 中樞神經系統 (CNS) 侵犯的風險增加。
鑑別診斷 (Differential Diagnosis)
- 在適當的臨床情境下,其組織學特徵即具診斷意義。凝血病 (coagulopathies) 與管腔內纖維蛋白樣栓子相關,但不伴有廣泛的血管壁纖維蛋白樣變化 (fibrinoid change)。
- 具有 atrophie blanche 臨床表現的病灶會顯示一些見於鬱滯性皮膚炎 (stasis dermatitis) 的特徵,例如淺層真皮的血管叢集;然而,單純未複雜化的鬱滯並不會顯示纖維蛋白樣變化。
膽固醇結晶栓塞與心房黏液瘤栓塞之皮膚表現 (Dermatological manifestations of cholesterol crystal embolism and embolism from atrial myxoma)
臨床特徵 (Clinical Features)
- 膽固醇結晶栓塞 (cholesterol crystal embolism) 是一種老年人的疾病,典型上發生於男性(4:1),從而反映出動脈粥樣硬化 (atherosclerosis) 的人口學特徵。膽固醇栓塞可自發發生,或併發於主動脈或其他大動脈的外傷。它可見於 warfarin 治療之後。
- 因梗塞所致的全身性症狀程度不一,並取決於發生栓塞的器官。曾有文獻描述在膽固醇結晶栓塞之後出現壞死性血管炎 (necrotizing vasculitis)。多系統侵犯有時會導致最初被診斷為血管炎。
- 病人常表現為發熱 (pyrexia)、肌痛 (myalgia)、突然發作的全身性高血壓,以及腎衰竭與皮膚病灶。紅血球沉降速率 (ESR) 上升、血液嗜酸性球增多 (eosinophilia) 與血清肌酸酐 (creatinine) 升高為附加特徵。皮膚表現常見,包括:
- 網狀青斑 (livedo reticularis),常為雙側性,侵犯足部與腿部,有時向上延伸侵犯軀幹;
- 腳趾壞疽 (gangrene)(圖 16.116);
- 發紺 (cyanosis);
- 腳趾呈紫色變色;
- 皮膚潰瘍;
- 腿部、大腿、足部與腳趾的結節;
- 腿部與足部的紫斑性病灶。
- 因此,膽固醇結晶栓塞的皮膚病灶會模擬許多其他血管性病灶,切片檢查 (biopsy) 對診斷而言至關重要。由於心臟與中樞神經系統 (CNS) 的侵犯,死亡率非常高。
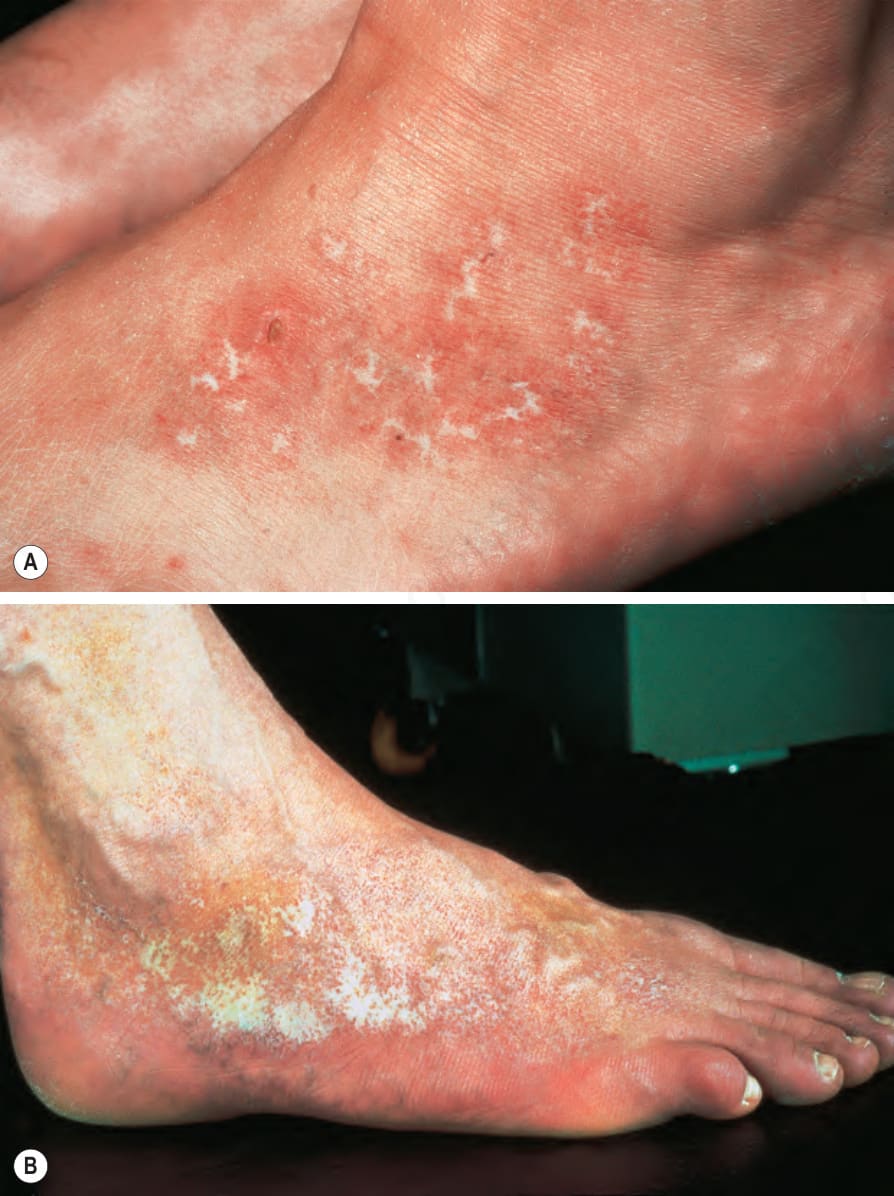
圖 16-110:Livedoid vasculopathy:(A) 出現伴有紅斑與脫屑的潰瘍;(B) 此例顯示踝部周圍明顯的色素過度沉著伴瘢痕與萎縮,並延伸至足背。By courtesy of the Institute of Dermatology, London, UK.
Fig. 16.110 Livedoid vasculopathy: (A) there is ulceration with erythema and scaling; (B) this example shows marked hyperpigmentation with scarring and atrophy around the ankle and extending onto the dorsum of the foot. By courtesy of the Institute of Dermatology, London, UK.

圖 16-111:Livedoid vasculopathy/atrophie blanche:一片廣泛的象牙白色瘢痕區覆蓋於內踝 (medial malleolus) 之上。By courtesy of R.A. Marsden, St George’s Hospital, London, UK.
Fig. 16.111 Livedoid vasculopathy/atrophie blanche: an extensive ivory-white area of scarring overlies the medial malleolus. By courtesy of R.A. Marsden, St George’s Hospital, London, UK.
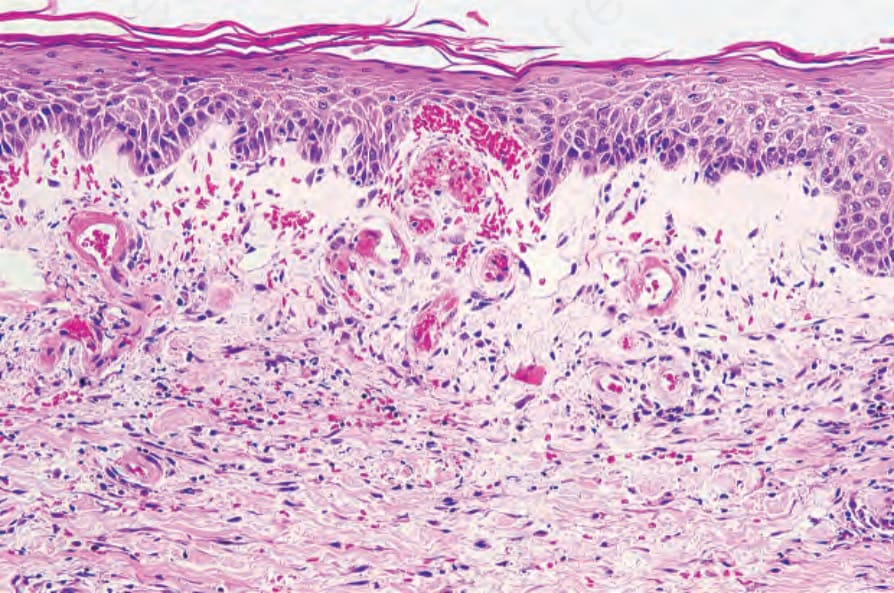
圖 16-112:Livedoid vasculopathy:真皮乳頭層的血管數目增加,並顯示管壁纖維蛋白沉積 (mural fibrin deposition)。其下方有瘢痕形成。
Fig. 16.112 Livedoid vasculopathy: the vessels in the papillary dermis are increased in number and show mural fibrin deposition. There is underlying scarring.
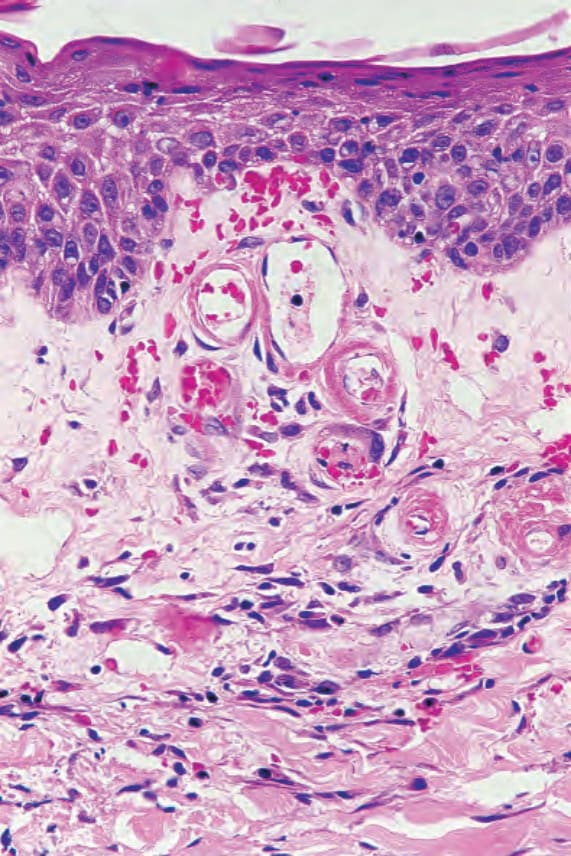
圖 16-113:Livedoid vasculopathy:血管的高倍視野。
Fig. 16.113 Livedoid vasculopathy: high-power view of vessels.
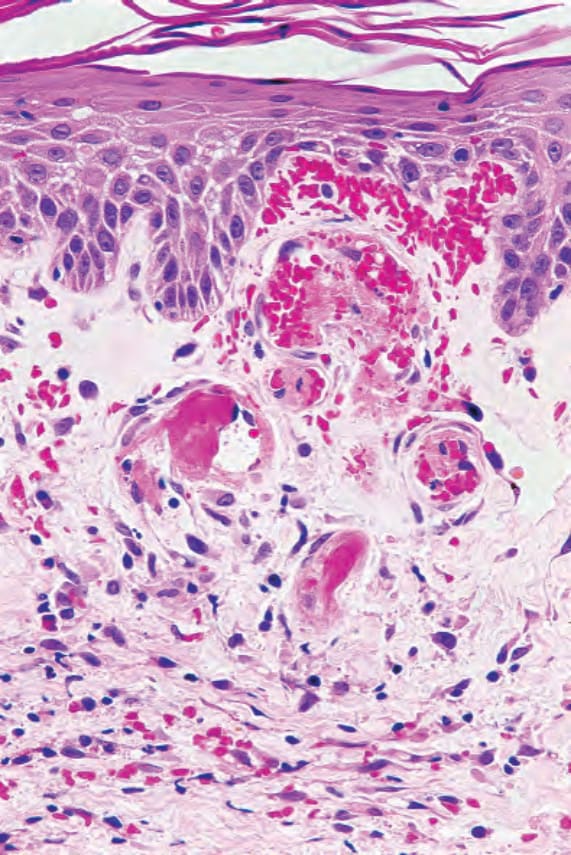
圖 16-114:Livedoid vasculopathy:可見阻塞的血管 (occluded vessels)。有明顯的紅血球外滲 (red blood cell extravasation)。
Fig. 16.114 Livedoid vasculopathy: occluded vessels are present. There is marked red blood cell extravasation.
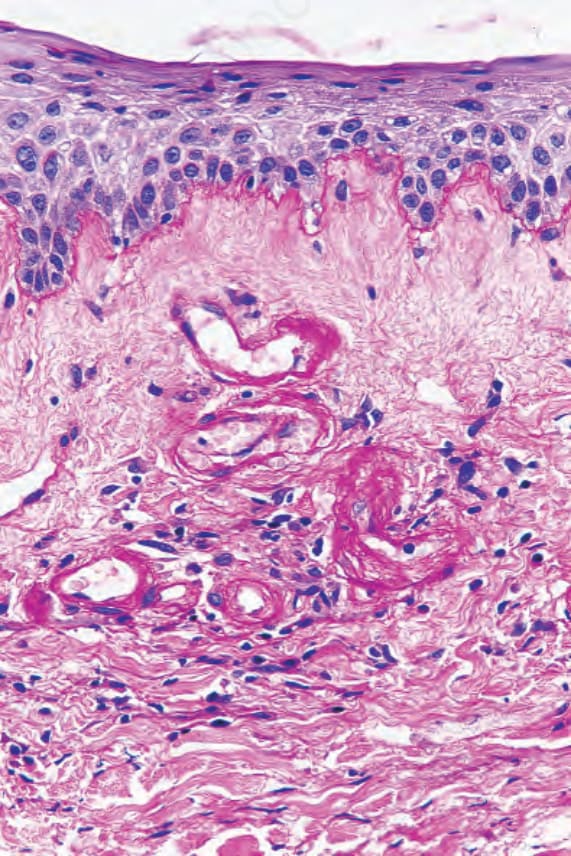
圖 16-115:Livedoid vasculopathy:血管壁呈強烈 PAS 陽性、抗澱粉酶 (diastase resistant)。
Fig. 16.115 Livedoid vasculopathy: the vessel walls are strongly PAS positive, diastase resistant.

圖 16-116:Cholesterol embolism:此老年男性病人的腳趾出現廣泛的梗塞 (infarction)。
Fig. 16.116 Cholesterol embolism: there is extensive infarction of the toes of this elderly male patient.
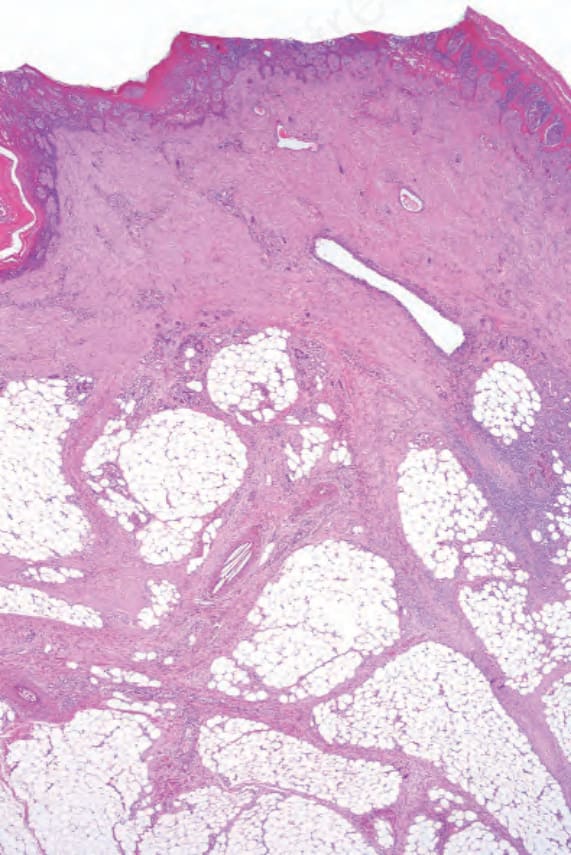
圖 16-117:Cholesterol emboli:出現潰瘍,且真皮瘢痕組織延伸進入皮下脂肪的隔膜 (septa)。視野中央一條動脈的管腔內可見針狀結晶 (needle-shaped crystals)。
Fig. 16.117 Cholesterol emboli: there is ulceration and dermal scar tissue extending into the septa of the subcutaneous fat. Needle-shaped crystals are present in the lumen of an artery in the middle of the field.