Livedoid vasculopathy and atrophie blanche
Livedoid vasculopathy and atrophie blanche
Clinical features Livedoid vasculopathy and atrophie blanche (also referred to as livedo vasculitis, livedoid vasculitis, and segmental hyalinizing vasculitis) have traditionally been used interchangeably. It is a common dermatosis that usually occurs in young to middle-aged women.1–5 However, it has been argued that the term livedoid vasculopathy be used to describe the disease entity, and that atrophie blanche be used as a description of a certain pattern of clinical manifestation that is often, though not invariably, associated with livedoid vasculopathy.5 In addition to the association with the thrombotic vasculopathy that is livedoid vasculopathy, the changes of atrophie blanche may be seen in chronic venous insufficiency.5 Early in the course the patients may present with painful purpuric papules and plaques that progress to ulcers.5 In its fully established state, the lesions may develop into atrophie blanche consisting of one or more irregular, smooth, atrophic plaques surrounded
758 Vascular diseases
A
B
Pathogenesis and histologic features
The pathogenesis of livedoid vasculopathy is not entirely understood but is clearly a thrombotic vasculopathy resulting in ischemia. Hydrostatic pressure certainly contributes to the development, given the predilection for the distal lower extremities and the association with venous insufficiency in some cases. Both immunoglobulin (usually IgM, less often IgG and IgA) and complement within the blood vessel walls raise the possibility of an immunological pathogenesis in some cases.20 It has been associated with a localized defect of tissue plasminogen activator.3,21 The location of the lesions suggests that trauma may also play some role in development of some lesions. As previously mentioned, many cases are associated with disorders of coagulation, suggesting an underlying coagulopathy is the basis of disorder.4,5,10–18 Elevated levels of lipoprotein(a) are associated with livedoid vasculopathy and may also contribute to a prothrombotic state.22
by a hyperpigmented border and telangiectases (Figs 16.110 and 16.111). Ulcerative lesions of two types may precede it:
• small (1–5 mm diameter), very painful erythematous purpuric areas that ulcerate and heal slowly,
• chronic large areas of ulceration up to 5 cm in diameter, which, after a long period of time, heal to form extensive areas of atrophic plaque. The condition shows seasonal variation, typically worsening in the summer months. Lesions recur at periodic intervals and are predominantly located on the lower legs, ankles, and the dorsal surfaces of the feet. Occasionally, however, they are found around the forearms, fingers, and hands or even in a more widespread distribution.3,6,7 The clinical manifestation of atrophie blanche is often associated with signs of venous stasis.8,9
Early and ulcerative lesions are characterized by the presence of increased numbers of dermal vessels containing fibrin within their walls in addition to intraluminal fibrinoid plugs (Figs 16.112–16.114). The latter are typically diastase resistant and periodic acid-Schiff (PAS) positive, and can also be highlighted by use of the phosphotungstic acid–hematoxylin stain (Fig. 16.115). Inflammatory destruction of blood vessels is, however, not a feature and therefore this disorder is not a true vasculitis. Variable degrees of red cell extravasation are evident, and hemosiderin pigment is often present. A perivascular lymphohistiocytic infiltrate of varying intensity is usually found, and dermal mast cells are often increased in number. Ulcerative lesions show infarction of the superficial dermis and epidermis. In the fully established atrophic plaque, in addition to the vascular changes, the epidermis is atrophic and the dermis shows dense scleroderma-like scarring.
Approximately half of patients involved have coagulation abnormalities, including factor V Leiden mutation, decreased protein C or protein S activity, prothrombin G20210A mutation, anticardiolipin antibodies, homocysteinemia, lupus anticoagulant, cryoglobulinemia, and methylenetetrahydrofolate reductase mutation.4,5,10–18 One study found 17% of lupus patients were affected.19 This study also noted that the pattern of cutaneous lesions was somewhat unusual, with involvement of the knees, elbows, fingers, soles, and the back.19 The same study suggested that patients with lupus erythematosus who have atrophie blanche are at an increased risk of developing lupus CNS involvement.19
Differential diagnosis The histologic features in the appropriate clinical setting are diagnostic. Coagulopathies are associated with intraluminal fibrinoid plugs but not extensive fibrinoid change of the vessel wall. Lesions with the clinical manifestation of atrophie blanche show some of the features seen in stasis
759 Dermatological manifestations of cholesterol crystal embolism and embolism from atrial myxoma
dermatitis, such as clustering of vessels in the superficial dermis; however, uncomplicated stasis does not show fibrinoid change.
Dermatological manifestations of cholesterol crystal embolism and embolism from atrial myxoma
Clinical features Cholesterol crystal embolism is a disease of the elderly and typically occurs in males (4 : 1), thereby reflecting the demographics of atherosclerosis.1,2 Cholesterol embolism may occur spontaneously or complicate trauma to the aorta or other large arteries.1,3 It can be seen following warfarin therapy.4 Systemic symptoms due to infarction are variable and depend upon the
organ embolized. Necrotizing vasculitis has been described following cholesterol crystal embolization.5 Multisystem involvement sometimes results in an initial diagnosis of vasculitis.
Patients commonly manifest pyrexia, myalgia, and a sudden onset of systemic hypertension as well as renal failure and cutaneous lesions.6 An
760 Vascular diseases
increased ESR, blood eosinophilia, and raised serum creatinine are additional features. Cutaneous manifestations are common and include:
• livedo reticularis, often bilateral, affecting the feet and legs and sometimes extending up to involve the trunk,7
• gangrene of the toes (Fig. 16.116),
• cyanosis,
• purple discoloration of the toes,
• cutaneous ulceration,
• nodules on the legs, thighs, feet, and toes,
• purpuric lesions on the legs and feet. The cutaneous lesions of cholesterol crystal embolism therefore mimic many other vascular lesions, and biopsy is essential for diagnosis. Mortality is very high due to cardiac and CNS involvement.
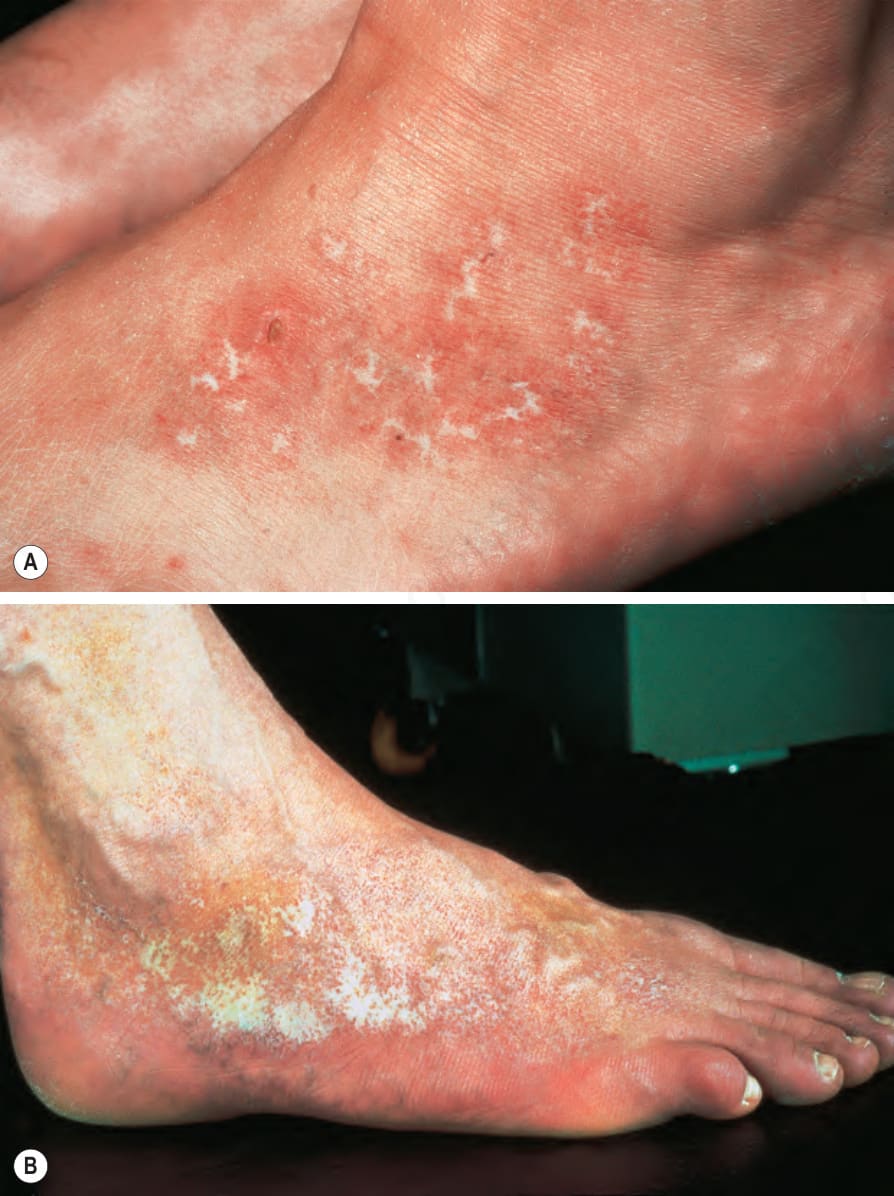
Fig. 16.110 Livedoid vasculopathy: (A) there is ulceration with erythema and scaling; (B) this example shows marked hyperpigmentation with scarring and atrophy around the ankle and extending onto the dorsum of the foot. By courtesy of the Institute of Dermatology, London, UK.

Fig. 16.111 Livedoid vasculopathy/atrophie blanche: an extensive ivory-white area of scarring overlies the medial malleolus. By courtesy of R.A. Marsden, St George’s Hospital, London, UK.
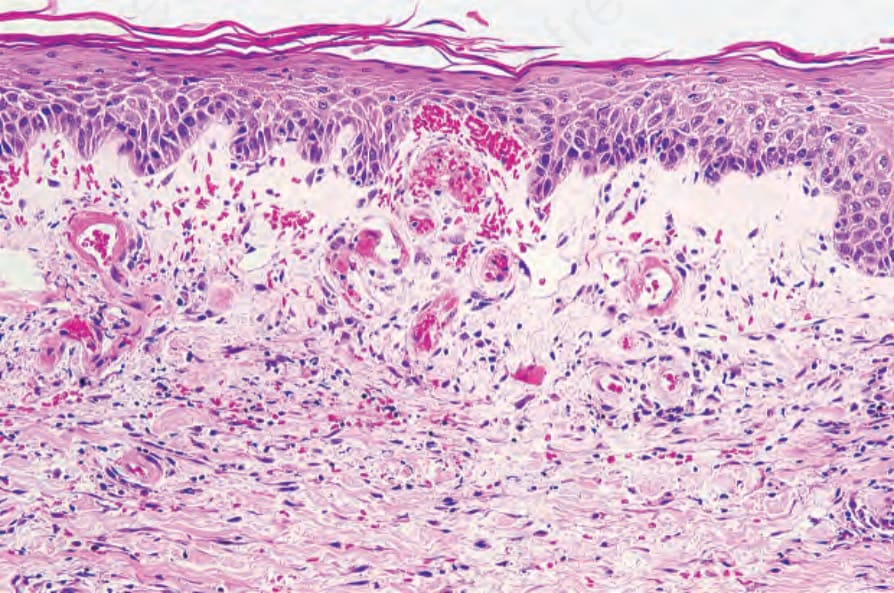
Fig. 16.112 Livedoid vasculopathy: the vessels in the papillary dermis are increased in number and show mural fibrin deposition. There is underlying scarring.
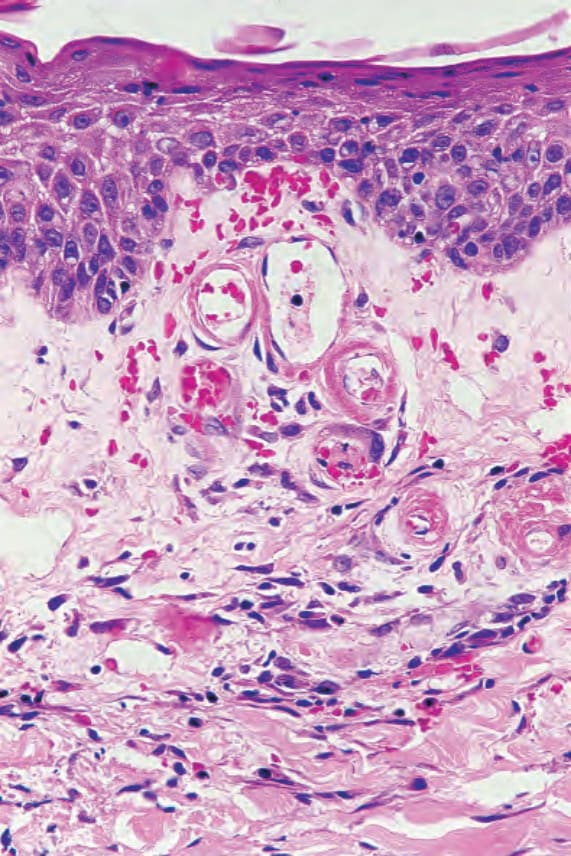
Fig. 16.113 Livedoid vasculopathy: high-power view of vessels.
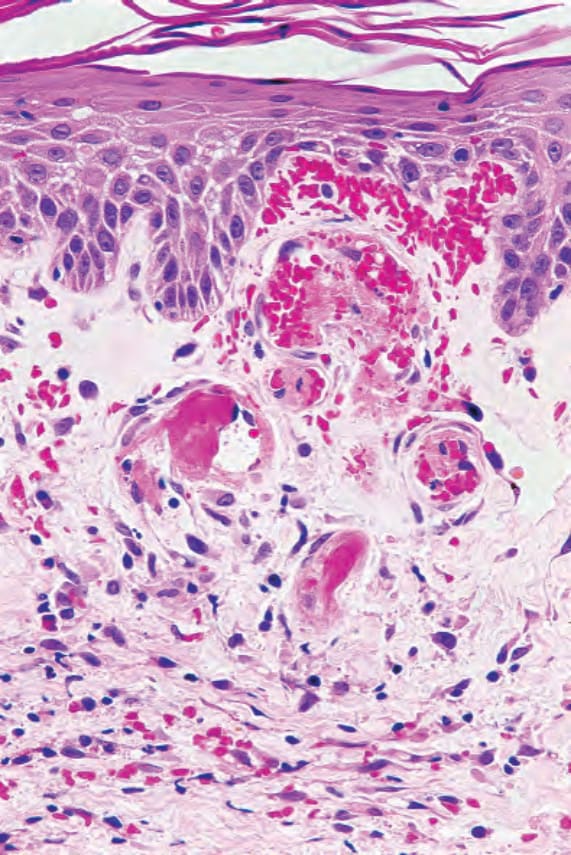
Fig. 16.114 Livedoid vasculopathy: occluded vessels are present. There is marked red blood cell extravasation.
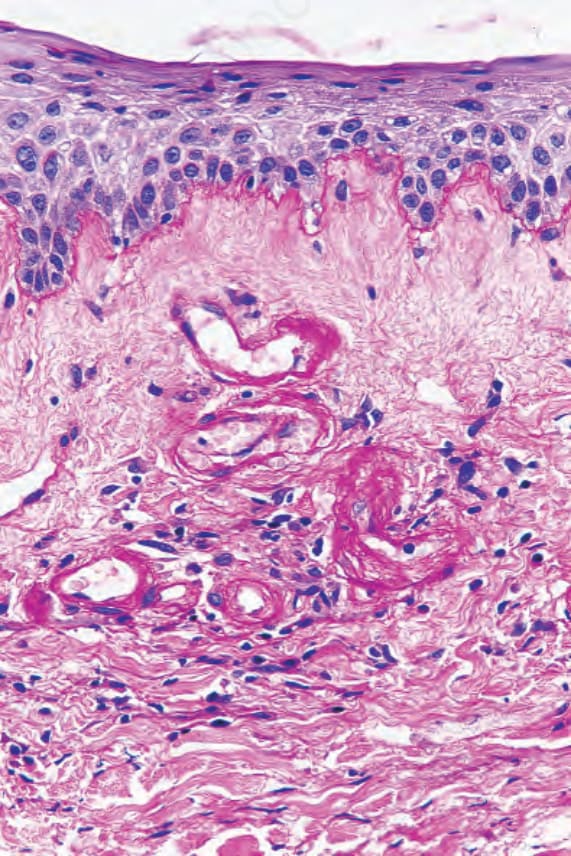
Fig. 16.115 Livedoid vasculopathy: the vessel walls are strongly PAS positive, diastase resistant.

Fig. 16.116 Cholesterol embolism: there is extensive infarction of the toes of this elderly male patient.
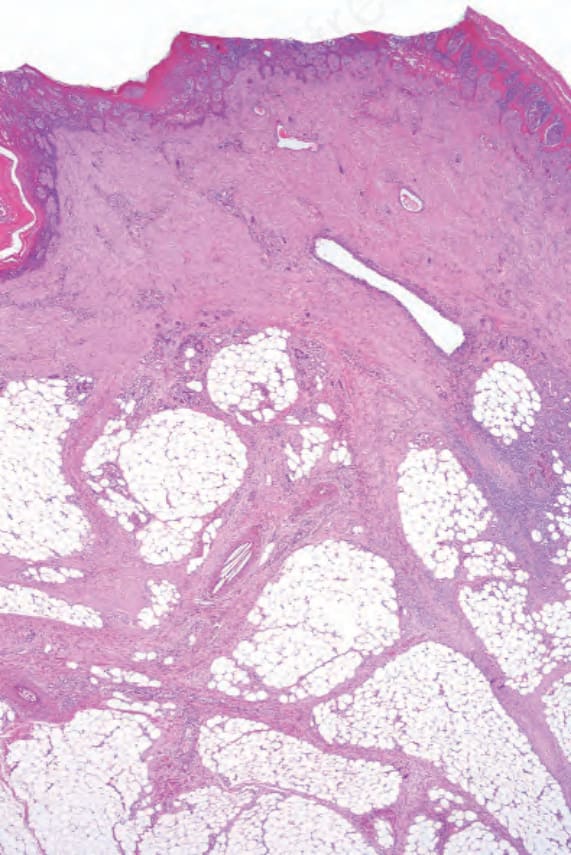
Fig. 16.117 Cholesterol emboli: there is ulceration and dermal scar tissue extending into the septa of the subcutaneous fat. Needle-shaped crystals are present in the lumen of an artery in the middle of the field.