惡性萎縮性丘疹病 (Malignant Atrophic Papulosis)
臨床特徵 (Clinical Features)
- 惡性萎縮性丘疹病 (malignant atrophic papulosis;Degos disease、Köhlmeier-Degos disease、致死性腸皮膚症候群 lethal intestinocutaneous syndrome) 是一種罕見、侵犯多重系統的疾病,通常預後不良。其病因不明,男性居多 (3 : 1),多侵犯年輕與中年人。發病時的平均年齡為 33 歲;然而文獻所述診斷時的年齡範圍很廣 (從嬰兒期至 67 歲)。偶有家族性侵犯的紀錄。妊娠期間發病則罕見。
- 皮膚病灶具特徵性,雖然類似病灶也可能是其他疾病的表現,包括 SLE、systemic sclerosis、dermatomyositis、rheumatoid arthritis 與 Crohn disease。有學者提出,malignant atrophic papulosis 代表一種主要見於 lupus erythematosus 的反應型態,而非一種本身獨立的特定疾病。病灶可能數量相當多,呈批 (crops) 出現,初起為粉紅色或黃灰色丘疹,直徑可達 5 mm,好發於軀幹與四肢近端。其特徵為手掌、足底、顏面與頭皮不受侵犯。這些丘疹通常無症狀,不會潰瘍或結疤。隨病程進展,發展出特徵性外觀:散在的小斑塊,由中央凹陷、呈白色瓷樣 (porcelain-like) 外觀並帶細鱗屑的區域組成,周圍環繞一圈狹窄的紅色或紫紅色邊緣,並伴有細微的微血管擴張 (telangiectasia) (Fig. 16.101)。罕見情況下,類似病灶可見於頰黏膜與生殖器黏膜。陰莖潰瘍的紀錄極少。有時可見結膜上無血管的蒼白斑塊。
- 腸道表現多變。雖然從口腔至肛門的腸道系統任何一段皆可能受侵犯,但主要受影響的是小腸。部分病人無症狀,其他人則訴有消化不良、腹瀉、便秘或腹脹與腹痛。腹腔鏡檢查通常顯示特徵性的漿膜下白色、黃色或粉紅色斑塊,典型呈輕度凹陷、直徑數公分。極為重要的是,部分病人會發生小腸穿孔,進而導致腹膜炎。可能併發侵犯小腸的瘻管 (fistulae)。亦可見大網膜壞死 (omental necrosis)。罕見情況下,腸道侵犯先於皮膚表現出現。急性小腸穿孔可為本病的首發表現。此外,腸道病灶有時在初次皮膚表現後多年才出現。
- 本病可侵犯周邊與中樞神經系統,偶爾此類病灶主導臨床表現。症狀多變,並因侵犯多處而偶有多重表現。例如,半身與四肢癱瘓 (hemi- and quadriplegias)、感覺喪失與顱神經病灶皆可能出現。
- 在多數病人中,malignant atrophic papulosis 是一種真正的全身性疾病。病灶可見於多種部位,包括心臟、肺、腎、膀胱與肝。
- 雖然本病通常預後不良且死亡率高,但確實存在一個亞群的病人,其皮膚表現為唯一的表現,且病程演變為良性。腸道侵犯似乎與不良預後特別相關。死亡率與腸道穿孔尤其相關。
- 曾有後天性免疫缺乏症候群 (acquired immunodeficiency syndrome) 病人發生 malignant atrophic papulosis 的報告。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- 確切病因不明,雖然病毒、遺傳、自體免疫機轉與纖維蛋白溶解 (fibrinolysis) 皆曾被提及。由於病灶有時並未伴隨顯著發炎,將其歸類為真正的血管炎 (vasculitis) 是否恰當尚有爭議。其致病機轉為血管栓塞 (vascular thrombosis),病灶的根本病理為梗塞 (infarction)。曾有報告描述梗塞病灶中央有局部纖維蛋白溶解缺陷 (focal fibrinolytic defect) 以及纖維蛋白溶解與血小板功能的改變,但這些並非一致的發現。有學者提出,內皮腫脹與增生並繼發栓塞 (endothelial swelling and proliferation with secondary thrombosis) 為主要致病機轉。一份記載有 malignant atrophic papulosis 病人伴隨 anticardiolipin antibodies 升高的報告與此假說一致。然而其他學者未能證實此一發現。
- 在多數病例中,最初的內皮血管損傷之原因不明,但單核球性血管炎 (mononuclear vasculitis) 可能在致病機轉中扮演角色。多數作者認為下文所述的黏蛋白 (mucin) 沉積為次發性事件,是真皮缺血 (dermal ischemia) 的結果。
- 已成形的皮膚病灶具有特徵性外觀。其上覆表皮呈過度角化 (hyperkeratotic) 且萎縮 (atrophic)。緊鄰其下為一楔形 (wedge-shaped) 的真皮梗塞區,基底與表面上皮平行:其典型為色澤蒼白、細胞相對稀少,並伴有黏蛋白沉積 (Figs 16.102 and 16.103)。後者以 toluidine blue 染色呈異染性 (metachromatic),並顯示對 hyaluronidase 敏感的 Alcian blue 染色。較陳舊的病灶常見潰瘍。梗塞區鄰近與深部的血管常呈玻璃樣變 (hyalinized),並顯示血管周圍淋巴球浸潤 (Figs 16.104 and 16.105)。通常 (但非總是) 在病灶頂端的血管中可見內皮血管炎 (endovasculitis):由內皮細胞增生組成,有時併發栓塞。內彈性膜 (internal elastic lamina)、中膜 (media) 與漿膜 (serosa) 通常不受侵犯。曾有描述模擬 lupus erythematosus profundus 的脂膜炎 (panniculitis)。
- 腸道病灶的顯微鏡檢查顯示透壁性 (transmural) 腸道發炎,伴有潰瘍與出血。後者可侵犯小腸與大腸,包括直腸 (Figs 16.106–16.109)。血管變化包括嚴重的內膜增厚 (intimal thickening) 以致管腔直徑嚴重縮小、栓塞與急性血管炎。
鑑別診斷 (Differential Diagnosis)
- 如上所述,皮膚表現具特徵性,診斷應相對直接。然而須謹記,雖然 malignant atrophic papulosis 的皮膚病灶具典型性,類似病灶亦曾見於其他疾病的病人,例如 SLE、systemic sclerosis、rheumatoid arthritis、dermatomyositis 與 Crohn disease。因此建議搜尋潛在或相關的疾病。

圖 16-101 (A, B):惡性萎縮性丘疹病 (malignant atrophic papulosis):注意典型的小丘疹,具凹陷中央與細微的白色鱗屑。By courtesy of the Institute of Dermatology, London, UK.
Fig. 16.101 (A, B) Malignant atrophic papulosis: note the typical small papules with depressed centers and fine white scaling. By courtesy of the Institute of Dermatology, London, UK.
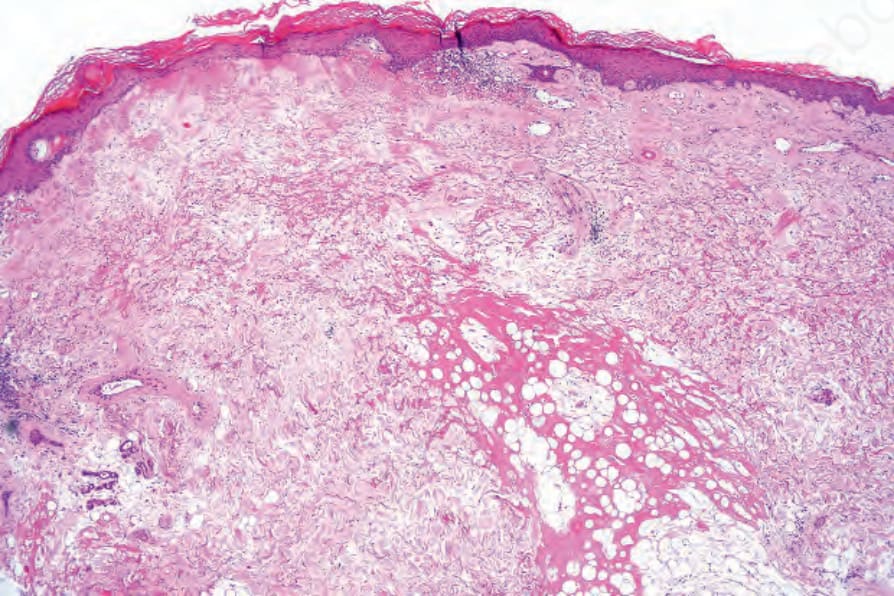
圖 16-102:惡性萎縮性丘疹病 (malignant atrophic papulosis):可見過度角化 (hyperkeratosis) 與表皮萎縮 (epidermal atrophy),並伴有一區真皮梗塞 (dermal infarction)。注意擴張的血管 (ectatic vessels)。
Fig. 16.102 Malignant atrophic papulosis: there is hyperkeratosis and epidermal atrophy associated with a zone of dermal infarction. Note the ectatic vessels.
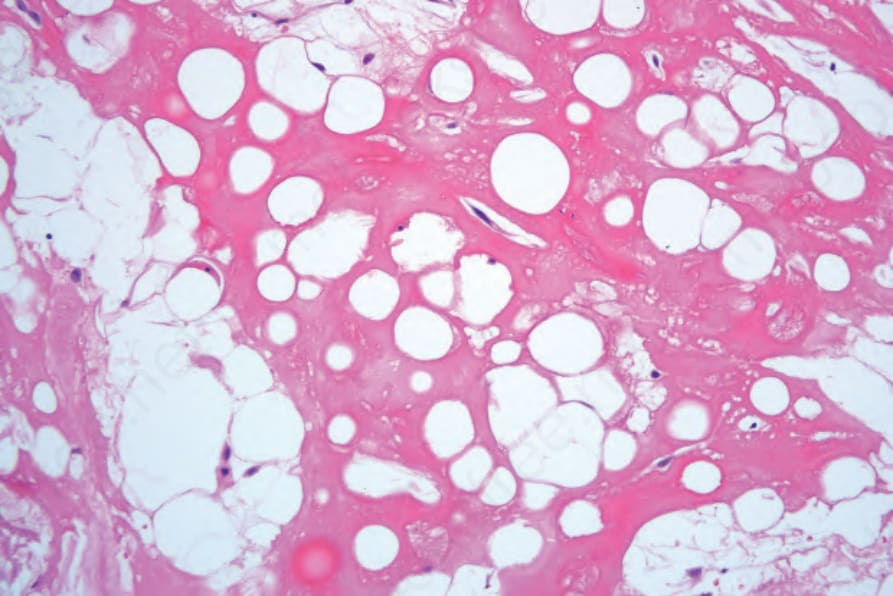
圖 16-103:惡性萎縮性丘疹病 (malignant atrophic papulosis):高倍視野顯示玻璃樣化的脂肪壞死 (hyalinized fat necrosis)。
Fig. 16.103 Malignant atrophic papulosis: high-power view showing hyalinized fat necrosis.
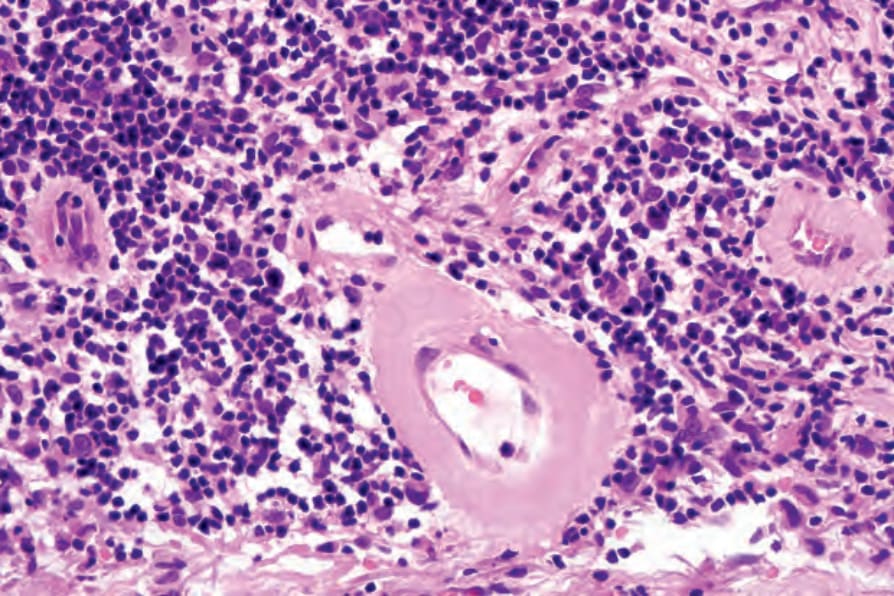
圖 16-104:惡性萎縮性丘疹病 (malignant atrophic papulosis):高倍視野顯示血管壁玻璃樣變 (blood vessel wall hyalinization) 與大量淋巴球浸潤。
Fig. 16.104 Malignant atrophic papulosis: high-power view showing blood vessel wall hyalinization and a heavy lymphocytic infiltrate.
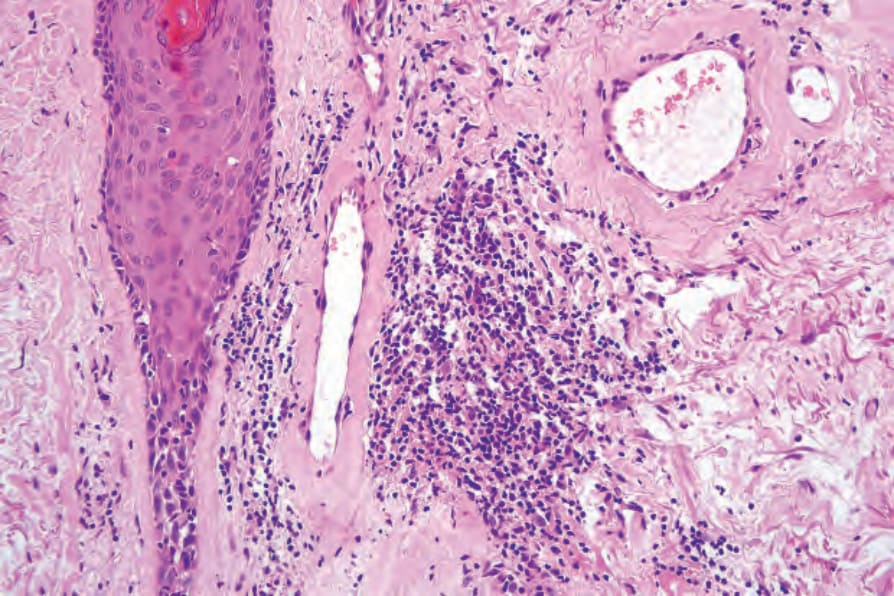
圖 16-105:惡性萎縮性丘疹病 (malignant atrophic papulosis):淺層血管增厚並玻璃樣變 (hyalinized)。
Fig. 16.105 Malignant atrophic papulosis: the superficial blood vessels are thickened and hyalinized.
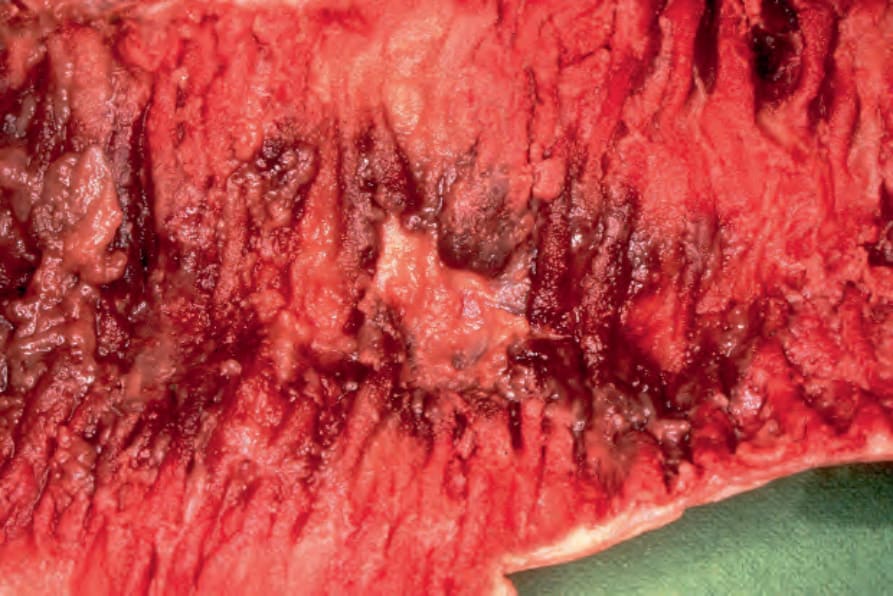
圖 16-106:惡性萎縮性丘疹病 (malignant atrophic papulosis):空腸 (jejunum) 切面顯示黏膜潰瘍,周圍伴有強烈充血 (congestion)。By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.
Fig. 16.106 Malignant atrophic papulosis: section of jejunum showing ulceration of the mucosa with surrounding intense congestion. By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.
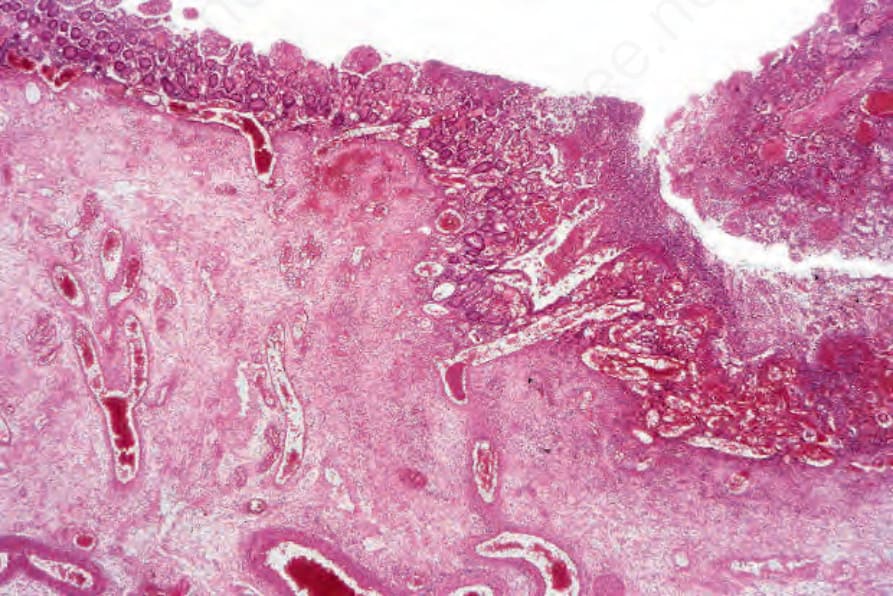
圖 16-107:惡性萎縮性丘疹病 (malignant atrophic papulosis):Fig. 16.106 所示空腸 (jejunum) 的組織學切片。注意急性發炎與潰瘍。By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.
Fig. 16.107 Malignant atrophic papulosis: histologic section of jejunum shown in Fig. 16.106. Note the acute inflammation and ulceration. By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.
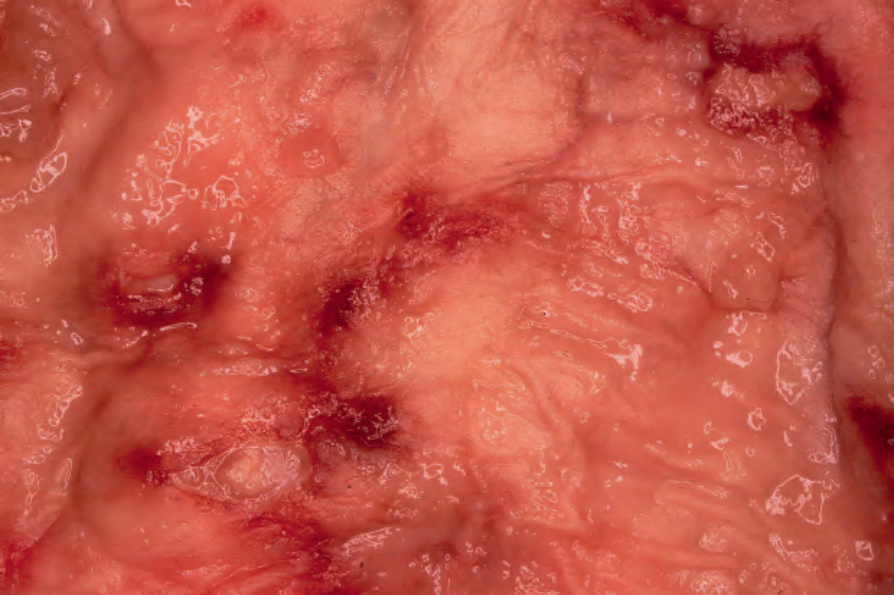
圖 16-108:惡性萎縮性丘疹病 (malignant atrophic papulosis):直腸 (rectum) 切面顯示局部充血 (congestion) 與潰瘍。By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.
Fig. 16.108 Malignant atrophic papulosis: section of rectum showing focal congestion and ulceration. By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.
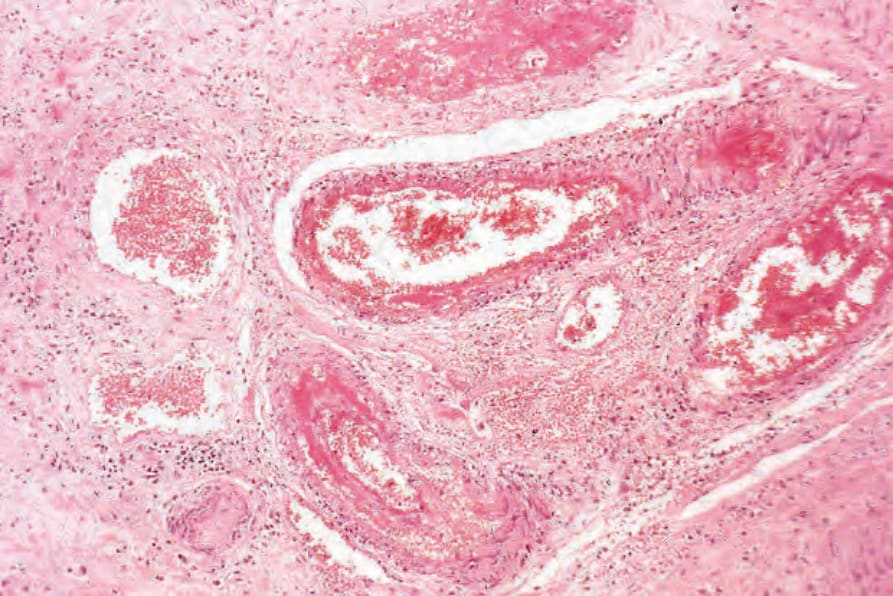
圖 16-109:惡性萎縮性丘疹病 (malignant atrophic papulosis):直腸黏膜下層 (submucosa) 的組織學切片。可見急性血管炎 (acute vasculitis) 伴栓塞 (thrombosis)。By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.
Fig. 16.109 Malignant atrophic papulosis: histologic section of the submucosa of the rectum. There is acute vasculitis with thrombosis. By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.