Malignant atrophic papulosis
Malignant atrophic papulosis
Clinical features Malignant atrophic papulosis (Degos disease, Köhlmeier-Degos disease, lethal intestinocutaneous syndrome) is a rare disorder affecting multiple systems and usually associated with a poor prognosis.1–4 It is of unknown etiology, shows a male predominance (3 : 1), and usually affects the young and middle aged. The mean age at presentation is 33 years; however, a wide age range at diagnosis (from infancy to 67 years) has been described.5,6 Occasional instances of familial involvement have been recorded.7–9 Presentation during pregnancy may rarely occur.10
B
The cutaneous lesions are distinctive, although similar lesions can be a manifestation of other diseases, including SLE, systemic sclerosis, dermatomyositis, rheumatoid arthritis, and Crohn disease.11–17 It has been proposed that malignant atrophic papulosis represents a reaction pattern mainly seen in lupus erythematosus and not a specific disease per se.17,18 Lesions, which may be quite numerous, appear in crops, initially as pinkish or yellow-gray papules up to 5 mm in diameter and showing a predilection for the trunk and proximal extremities. Characteristically, the palms, soles, face, and scalp are spared.19 The papules are usually asymptomatic and do not ulcerate or scar. With progression, they develop a characteristic appearance: discrete small patches composed of a central zone with a depressed white, porcelain-like appearance and a fine scale, surrounded by a narrow red or violaceous rim associated with fine telangiectasia (Fig. 16.101).19 On rare occasions, similar lesions are found on the buccal and genital mucosa. Penile ulceration has rarely been documented.19,20 Sometimes, avascular conjunctival pale patches are seen.21
Intestinal manifestations are variable. While any segment of the intestinal system from the oral cavity to the anus may be involved, it is predominantly the small intestine that is affected.13 Some patients are asymptomatic while others complain of indigestion, diarrhea, constipation or abdominal distension and pain. Laparoscopy usually reveals characteristic subserosal white, yellow, or pinkish plaques, typically slightly depressed and several centimeters in diameter.22 Of great importance, some patients develop small intestinal perforation with resultant peritonitis. Fistulae involving the small bowel may develop as a complication.22–24 Omental necrosis may also be seen.25 Rarely, intestinal involvement precedes the cutaneous features.26 Acute small bowel perforation can be the first manifestation of the disease.27 In addition, intestinal lesions sometimes develop many years after an initial cutaneous presentation.
The condition may involve both the peripheral and central nervous systems and occasionally such lesions dominate the clinical features.27–35 Symptoms are variable and are occasionally multiple due to various sites
756 Vascular diseases
being affected. For example, hemi- and quadriplegias, sensory losses, and cranial nerve lesions may all be encountered.35,36
Malignant atrophic papulosis is a truly systemic illness in most patients. Lesions are found in a variety of sites including the heart, lungs, kidneys, bladder, and liver.19,22,37–44
Although this disease is usually associated with a poor prognosis and high mortality, there does appear to be a subset of patients in whom the cutaneous features are the sole manifestation and evolution is benign.10,45–51 Intestinal involvement appears to correlate particularly with a poor outlook.52,53 Mortality is especially correlated with intestinal perforation.53
Malignant atrophic papulosis has been reported in a patient with acquired immunodeficiency syndrome.54
Pathogenesis and histologic features The precise etiology is unknown, although viral, genetic, autoimmune mechanisms, and fibrinolysis have all been implicated.55,56 Since lesions are sometimes not associated with significant inflammation, it is debatable whether classification as a true vasculitis is appropriate. The pathogenesis is that of vascular thrombosis, the essential pathology of the lesions being that of infarction.1 A focal fibrinolytic defect within the center of the infarcted lesions and alterations of fibrinolysis and platelet function have been described, but these are not consistent findings.1,57,58 It has been proposed that endothelial swelling and proliferation with secondary thrombosis is the primary pathogenesis.1 Consistent with this hypothesis is the documentation of a patient with malignant atrophic papulosis associated with elevated anticardiolipin antibodies.59 Others, however, have not been able to corroborate this finding.60
In most cases, the cause of the initial endothelial vascular insult is unknown, but a mononuclear vasculitis may play a role in the pathogenesis.4 Most authors regard the mucin deposition described below as a secondary event developing as a consequence of dermal ischemia.
The established cutaneous lesion has a characteristic appearance.61,62 The overlying epidermis is hyperkeratotic and atrophic. Immediately beneath this is a wedge-shaped zone of dermal infarction with the base parallel to the surface epithelium: it is typically pale in color, relatively acellular, and associated with mucin deposition (Figs 16.102 and 16.103).63 The latter is metachromatic with toluidine blue and demonstrates hyaluronidase-sensitive Alcian blue staining. Older lesions are frequently ulcerated. Often, the vessels adjacent and deep to the infarct are hyalinized and show a perivascular lymphocytic infiltrate (Figs 16.104 and 16.105). Usually, but not invariably, an endovasculitis can be demonstrated in the blood vessels at the apex of the lesion: this consists of endothelial cell hyperplasia, sometimes complicated by thrombosis. The internal elastic lamina, media, and serosa
757 Livedoid vasculopathy and atrophie blanche
are usually not involved. A panniculitis mimicking lupus erythematosus profundus has been described.64
Microscopic examination of the bowel lesions reveals transmural intestinal inflammation with ulceration and hemorrhage. The latter may involve the small and large intestines including the rectum (Figs 16.106–16.109). Vascular changes have included gross intimal thickening with consequent severe diminution in the lumen diameter, thrombosis, and acute vasculitis.65
Differential diagnosis As mentioned above, the cutaneous findings are distinctive and diagnosis should be relatively straightforward. However, it should be kept in mind that although the cutaneous lesions of malignant atrophic papulosis are typical, similar lesions have been described in patients with other diseases, such as SLE, systemic sclerosis, rheumatoid arthritis, dermatomyositis, and Crohn disease.11–16,66 A search for underlying or associated disorders is therefore advised.

Fig. 16.101 (A, B) Malignant atrophic papulosis: note the typical small papules with depressed centers and fine white scaling. By courtesy of the Institute of Dermatology, London, UK.
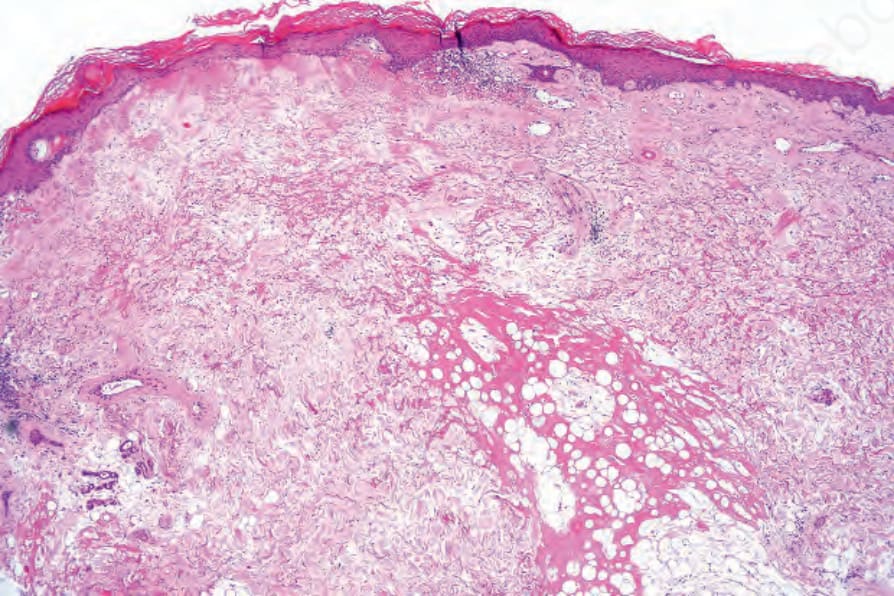
Fig. 16.102 Malignant atrophic papulosis: there is hyperkeratosis and epidermal atrophy associated with a zone of dermal infarction. Note the ectatic vessels.
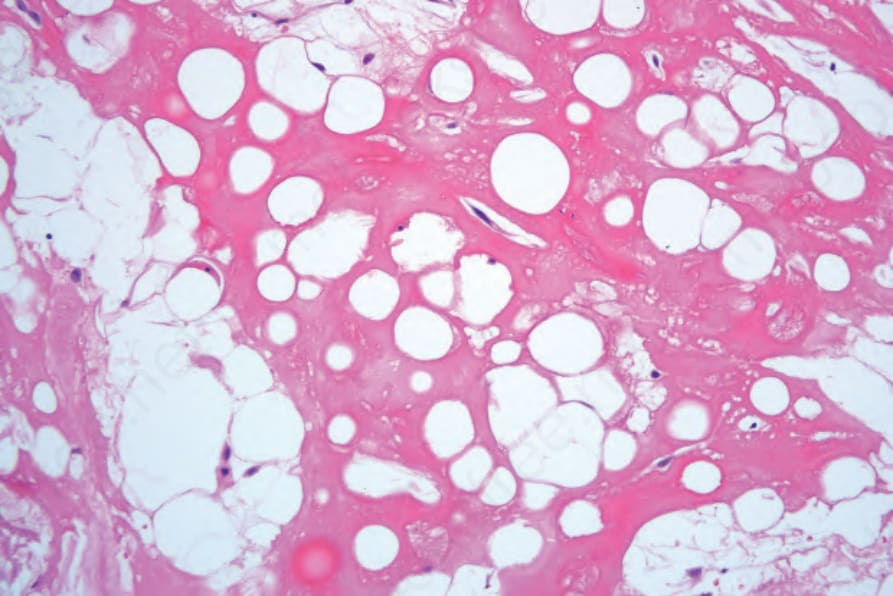
Fig. 16.103 Malignant atrophic papulosis: high-power view showing hyalinized fat necrosis.
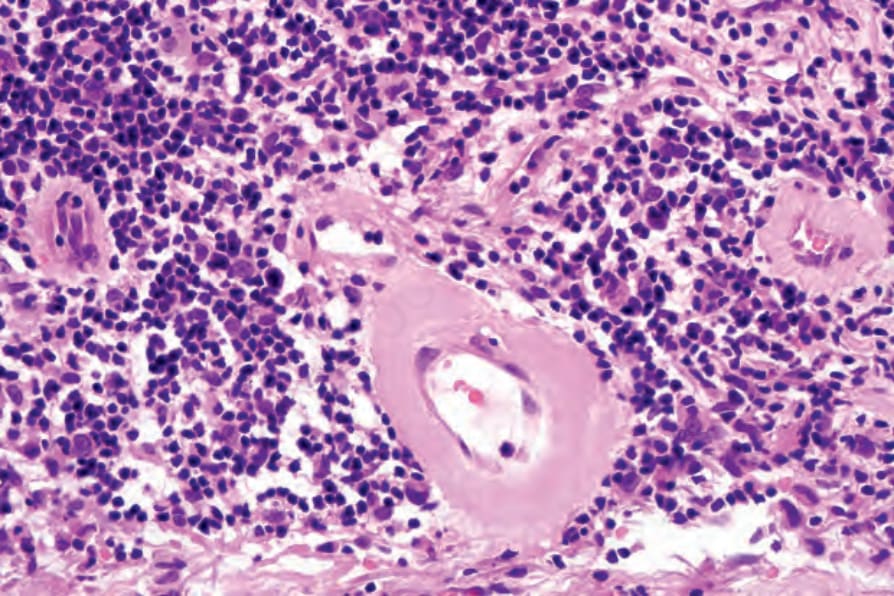
Fig. 16.104 Malignant atrophic papulosis: high-power view showing blood vessel wall hyalinization and a heavy lymphocytic infiltrate.
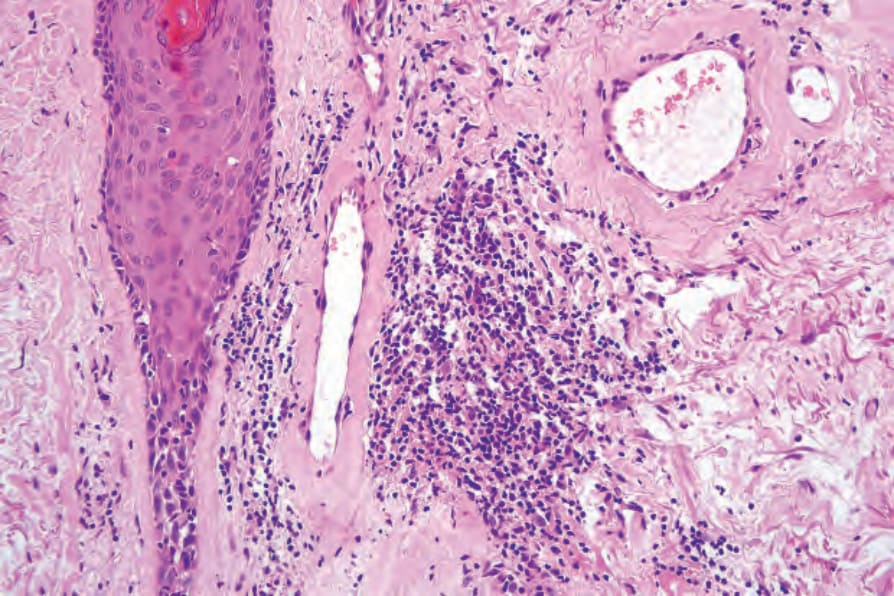
Fig. 16.105 Malignant atrophic papulosis: the superficial blood vessels are thickened and hyalinized.
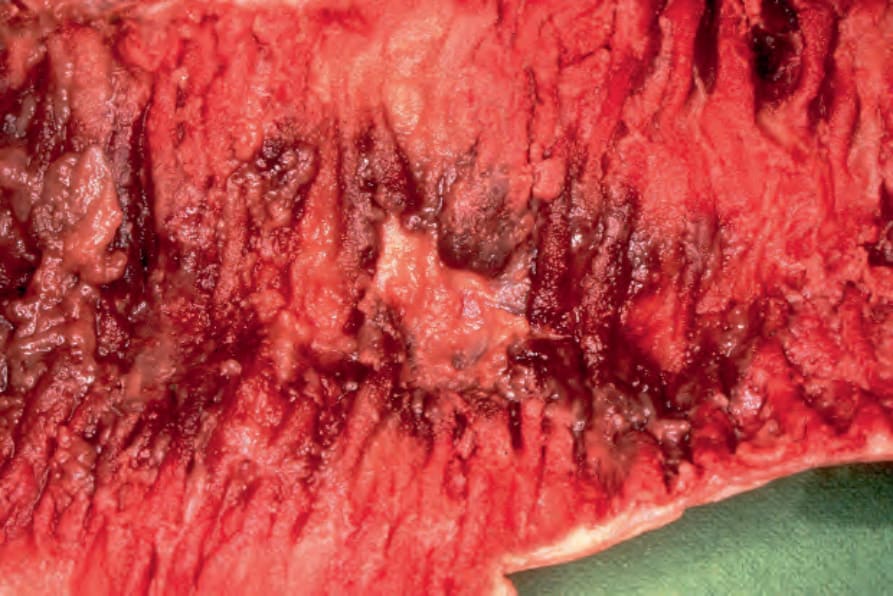
Fig. 16.106 Malignant atrophic papulosis: section of jejunum showing ulceration of the mucosa with surrounding intense congestion. By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.
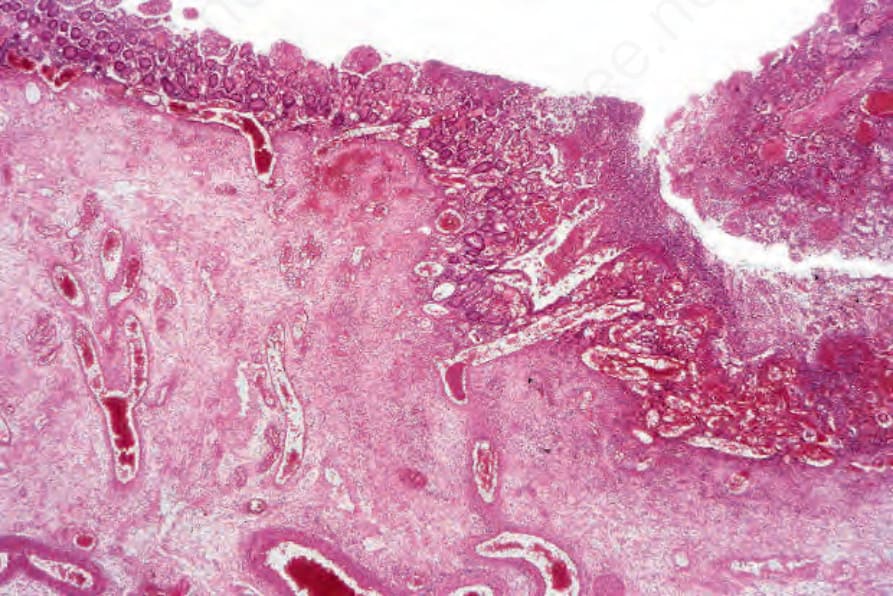
Fig. 16.107 Malignant atrophic papulosis: histologic section of jejunum shown in Fig. 16.106. Note the acute inflammation and ulceration. By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.
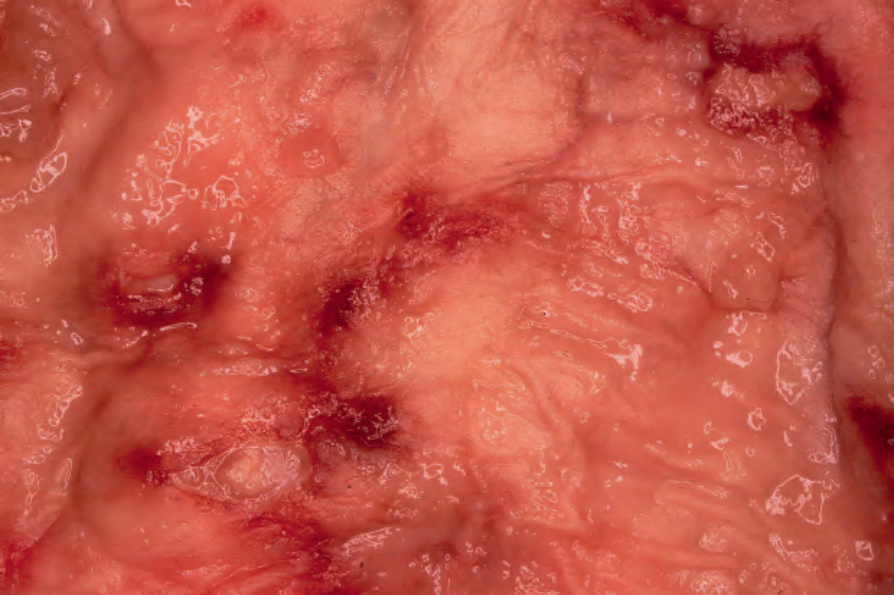
Fig. 16.108 Malignant atrophic papulosis: section of rectum showing focal congestion and ulceration. By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.
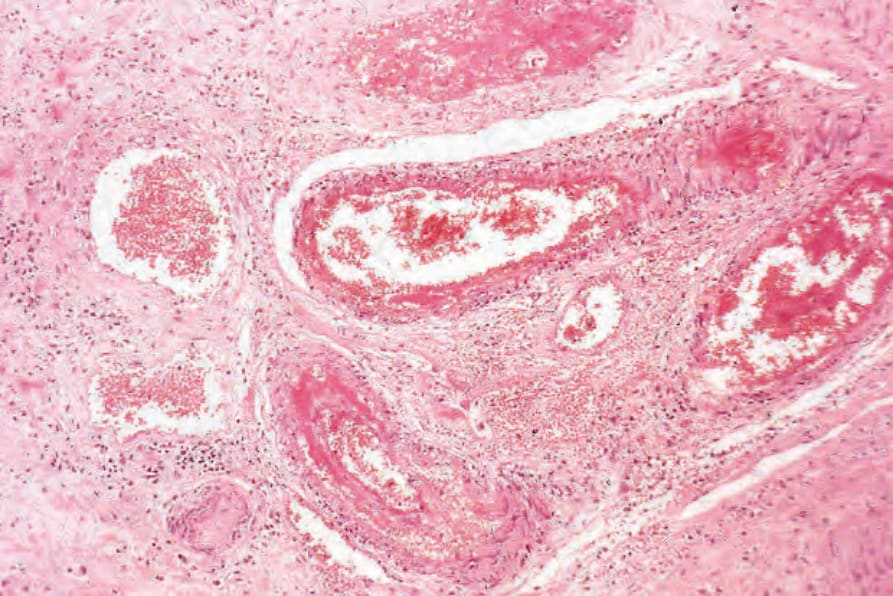
Fig. 16.109 Malignant atrophic papulosis: histologic section of the submucosa of the rectum. There is acute vasculitis with thrombosis. By courtesy of C.J.J. Mulder, MD, Rijnstate Hospital, Arnhem, The Netherlands.