嗜酸性蜂窩組織炎 (Eosinophilic Cellulitis)
臨床特徵 (Clinical Features)
- 嗜酸性蜂窩組織炎 (eosinophilic cellulitis;Wells syndrome) 是一種不常見的疾病,特徵為反覆出現的紅斑性、水腫性斑塊。其性別比相等,發病年齡範圍廣,平均年齡為 37 歲。
- 偶爾也見於兒童,並有罕見病例記載於新生兒。發生於兒童期的病例似乎可能特別嚴重。部分患者以頭皮受累、伴隨脫髮 (alopecia) 與瘢痕 (scarring) 為特徵。
- 本病特別侵犯四肢與軀幹。雖然最常以界限分明的(類似蜂窩組織炎的)環狀紅斑性斑塊呈現,且這些斑塊呈水腫且質地堅實,但已描述過各式各樣的臨床表現,包括水疱性 (blistering)、結節性 (nodular)、丘疹水疱性 (papulovesicular) 的疹子,以及搔癢、抓破的發炎性丘疹 (Figs 15.49–15.51)。這些斑塊在部分患者會造成疼痛與搔癢 (pruritus),典型上癒合後不留瘢痕。
- 嗜酸性蜂窩組織炎曾與蕁麻疹 (urticaria) 相關聯。皮膚劃痕症 (dermatographism) 可為其特徵之一。隨著病程進展,病灶有時會帶有綠色調。臨床上,病灶偶爾可能被誤認為感染過程。本病傾向呈陣發性 (episodic),有緩解與復發,病程可持續數月至數年。
- 罕見患者可見大型大疱 (large bullae)。曾有報告其受累呈沿 Blaschko lines 分布的不尋常型態,並有人提出此型代表皮膚鑲嵌現象 (cutaneous mosaicism)。
- 嗜酸性蜂窩組織炎罕見地與惡性腫瘤相關聯。曾描述伴隨嗜酸性白血病 (eosinophilic leukemia)、結腸癌 (colonic carcinoma)、肺鱗狀細胞癌 (squamous cell carcinoma of the lung) 及非何杰金氏淋巴瘤 (non-Hodgkin lymphoma) 的病例。偶爾也曾記載與 HIV、hypereosinophilic syndrome、潰瘍性結腸炎 (ulcerative colitis)、含破傷風 (tetanus) 或 thiomersal 的疫苗、水痘 (varicella) 感染、Churg-Strauss syndrome 及 IgG4-related disease 的相關聯。某些嗜酸性蜂窩組織炎病例似乎由藥物所誘發,包括 antibiotics、anticholinergic agents、anesthetics、non-steroidal anti-inflammatory drugs、thyroid medications 及 thiazide diuretics。亦曾報告一例與 henna 刺青相關的病例。
- 曾有報告極少數的家族性病例。在一個家族中,本病呈現體染色體顯性 (autosomal dominant) 的遺傳模式,並與發展遲緩 (developmental delay) 及異常的體型 (dysmorphic body habitus) 相關聯。在另一個家族中,病灶首次被注意到是在嬰兒期。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- 致病機轉不明,可能只是代表對各種傷害所產生的富含嗜酸性球 (eosinophil-rich) 的發炎反應。唯一一致的相關聯似乎是周邊嗜酸性球增多 (peripheral eosinophilia),表現為嗜酸性球總數升高,或嗜酸性球百分比增加。臨床活動度似乎與周邊血中 eosinophil cation protein 及 IL-5 濃度升高,以及血液與骨髓的嗜酸性球增多有關。
- 偶爾會出現紅血球沉降率 (ESR) 升高。有可能部分患者代表前一節所討論之 hypereosinophilic syndrome 譜系的良性端。
- 組織學上,嗜酸性蜂窩組織炎的早期病灶特徵為真皮內瀰漫且濃密的嗜酸性球浸潤:此浸潤可出現於表淺真皮、呈帶狀 (bandlike) 浸潤,或出現於深部真皮並延伸至下方的皮下組織、筋膜 (fascia) 與肌肉 (Figs 15.52 and 15.53)。此外,可能出現淋巴球 (lymphocytes) 與漿細胞 (plasma cells)。乳頭層真皮 (papillary dermis) 有時水腫至如此程度,以致發生表皮下大疱 (subepidermal bullae) (Fig. 15.54)。表皮可呈海綿水腫 (spongiotic),偶爾出現表皮內水疱 (intraepidermal vesicles)。
- 早期病灶可能與節肢動物叮咬反應 (arthropod bite reaction) 無法區分。在 1–3 週的期間內,嗜酸性球去顆粒化 (degranulate) 並退化,嗜酸性物質與核碎屑 (nuclear debris) 沉積於膠原纖維 (collagen fibers) 上,形成「火焰圖像」(‘flame figures’) (Fig. 15.55)。有時這些火焰圖像被組織球 (histiocytes) 與多核巨細胞 (multinucleated giant cells) 所環繞 (Fig. 15.56)。並無原發性膠原退化 (primary collagen degeneration) 的證據。火焰圖像很可能代表對各種不同激發刺激所產生的非特異性嗜酸性球反應型態。較後期,病灶變得更具肉芽腫性 (granulomatous),偶爾巨細胞 (giant cells) 顯著。有時可見紅血球外滲 (extravasation of red blood cells),但血管炎 (vasculitis) 通常並非其特徵,除了罕見報告演變為 Churg-Strauss syndrome 的病例。

圖 15-49:嗜酸性蜂窩組織炎:可見一大片紅斑性腫脹斑塊。四肢常受累。 (Eosinophilic cellulitis) From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
Fig. 15.49 Eosinophilic cellulitis: there is a large erythematous swollen plaque. The limbs are commonly affected. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
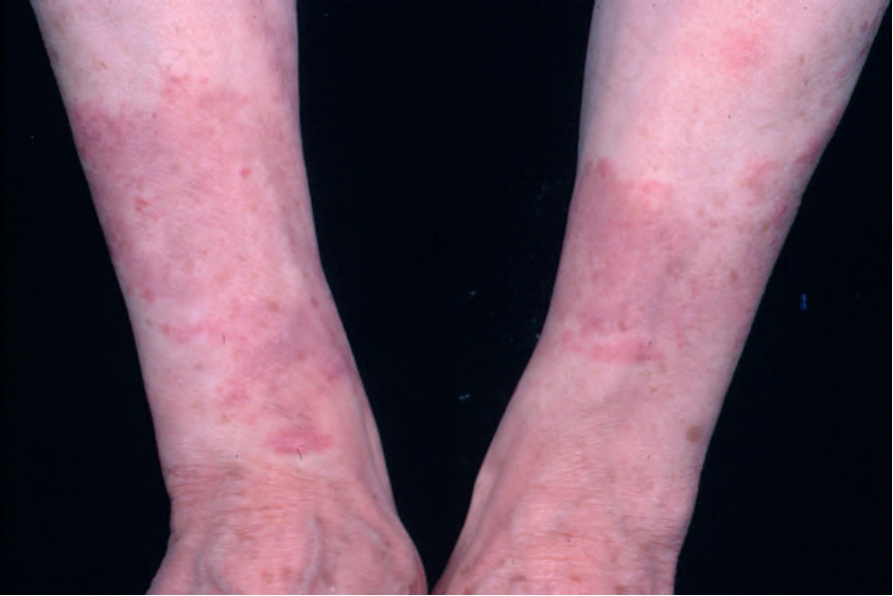
圖 15-50:嗜酸性蜂窩組織炎:此患者呈現顯著的對稱性。 (Eosinophilic cellulitis) From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
Fig. 15.50 Eosinophilic cellulitis: in this patient, there is striking symmetry. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 15-51:嗜酸性蜂窩組織炎:水疱性病灶,鄰近皮膚帶有些許綠色變色。 (Eosinophilic cellulitis; bullous lesion with greenish discoloration) From the collection of the late N.P. Smith, MD, Institute of Dermatology, London, UK.
Fig. 15.51 Eosinophilic cellulitis: bullous lesion with a hint of greenish discoloration in the adjacent skin. From the collection of the late N.P. Smith, MD, Institute of Dermatology, London, UK.
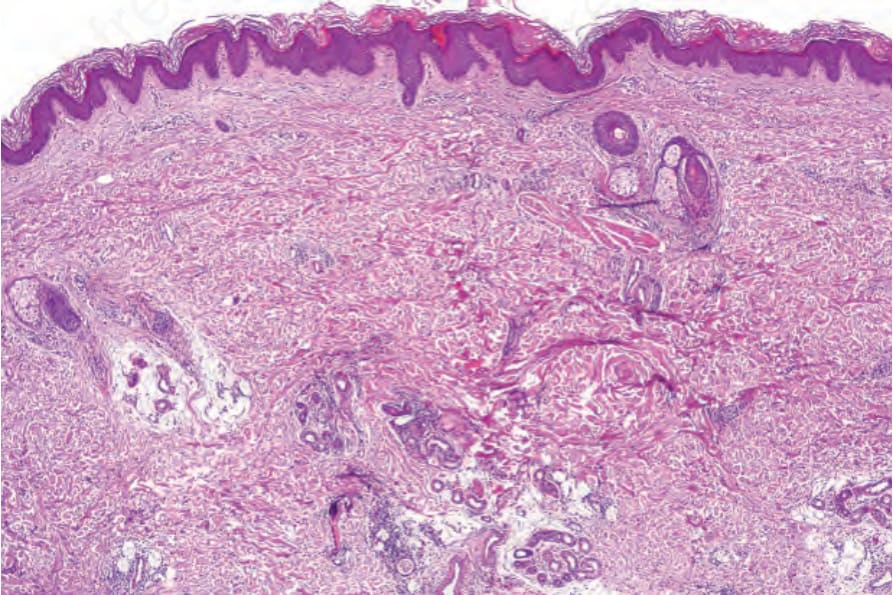
圖 15-52:嗜酸性蜂窩組織炎:可見輕度的深部真皮慢性發炎細胞浸潤。出現一個火焰圖像 (flame figure)。
Fig. 15.52 Eosinophilic cellulitis: there is a light, deep dermal chronic inflammatory cell infiltrate. A flame figure is present.
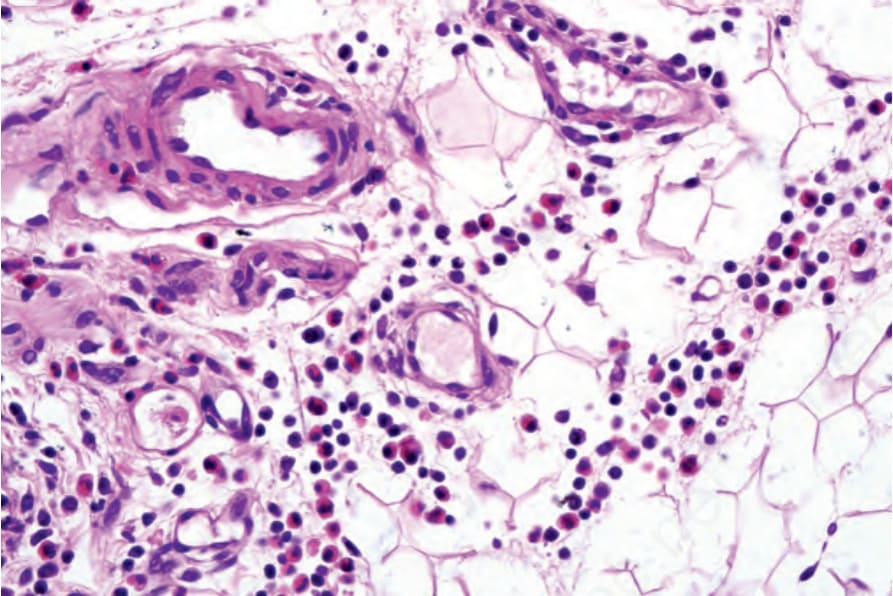
圖 15-53:嗜酸性蜂窩組織炎:浸潤由淋巴球 (lymphocytes) 與組織球 (histiocytes) 組成,並有顯著的嗜酸性球 (eosinophils),且延伸至皮下脂肪。
Fig. 15.53 Eosinophilic cellulitis: the infiltrate is composed of lymphocytes and histiocytes with conspicuous eosinophils and extends into the subcutaneous fat.
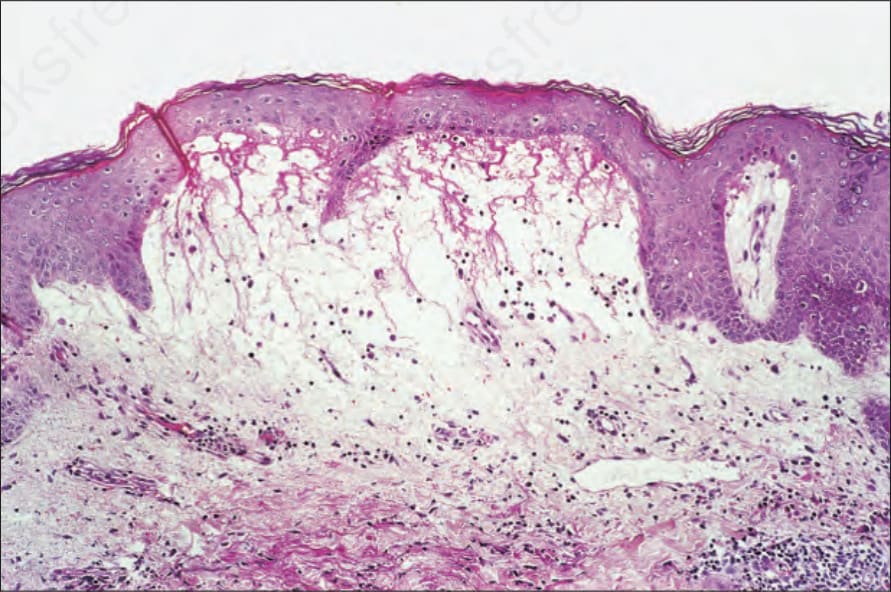
圖 15-54:嗜酸性蜂窩組織炎:如此處所見的表皮下水疱形成 (subepidermal vesiculation) 並不少見。水疱腔內可能含有大量嗜酸性球,類似類天疱瘡 (bullous pemphigoid)。
Fig. 15.54 Eosinophilic cellulitis: subepidermal vesiculation as seen here is not uncommon. The blister cavity may contain numerous eosinophils reminiscent of bullous pemphigoid.
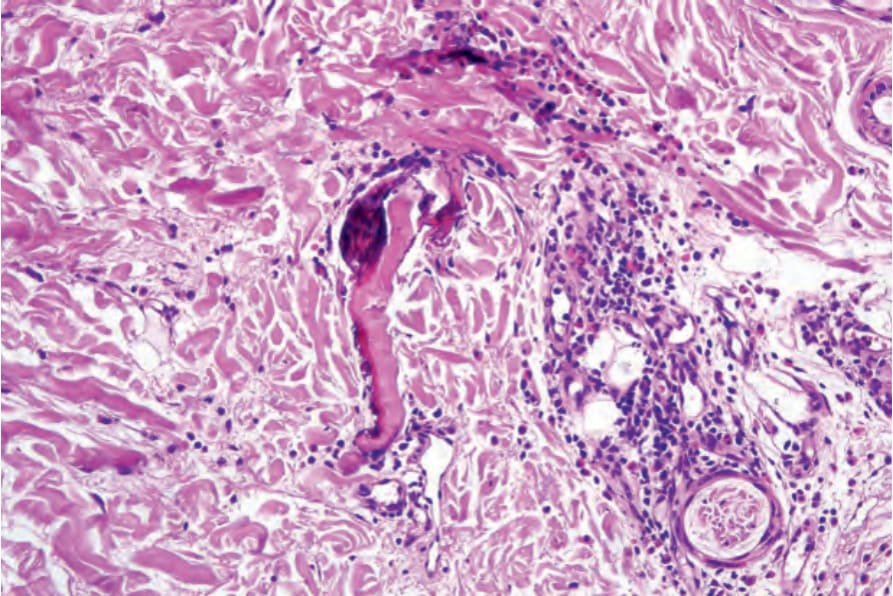
圖 15-55:嗜酸性蜂窩組織炎:典型上可見火焰圖像 (flame figures)。
Fig. 15.55 Eosinophilic cellulitis: flame figures are typically present.
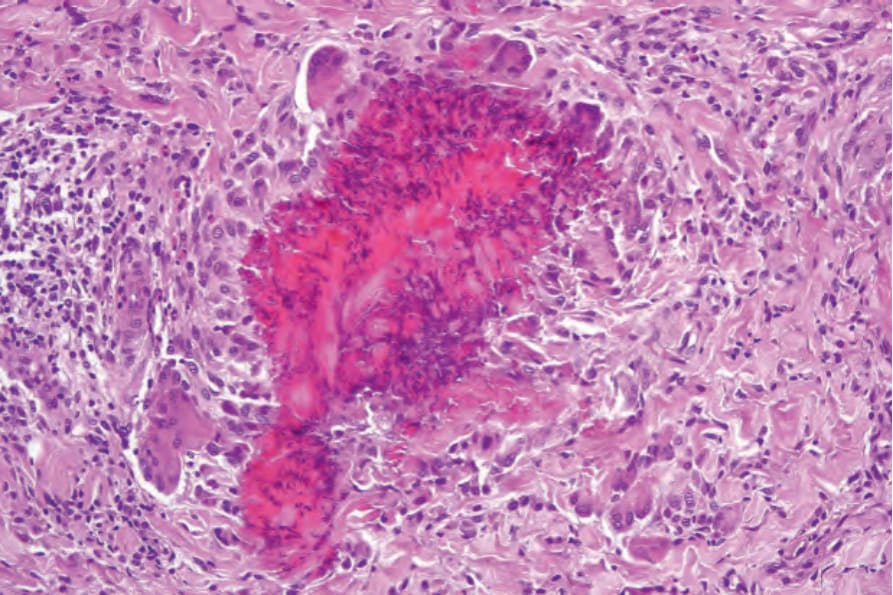
圖 15-56:嗜酸性蜂窩組織炎:在此例中,一個火焰圖像 (flame figure) 被強烈的肉芽腫性浸潤 (granulomatous infiltrate) 所環繞。
Fig. 15.56 Eosinophilic cellulitis: in this example, a flame figure is surrounded by an intense granulomatous infiltrate.
免疫螢光與超微結構 (Immunofluorescence and Ultrastructure)
- 間接免疫螢光 (indirect immunofluorescence) 研究顯示火焰圖像含有細胞外的 eosinophil granule major basic protein。超微結構 (ultrastructural) 研究證實嗜酸性球顆粒包覆於相關的膠原纖維上。直接免疫螢光 (direct immunofluorescence) 在少數病例中顯示血管壁有免疫球蛋白 (immunoglobulins) 及/或補體 (complement)。
鑑別診斷 (Differential Diagnosis)
- 雖然伴有「火焰圖像」的嗜酸性球浸潤之組織學特徵為 Wells syndrome 的特色,但並非具病理特異性 (pathognomonic)。類似的特徵也可見於節肢動物叮咬反應 (arthropod bite reactions)、蜘蛛咬傷 (spider bites)、蟠尾絲蟲病 (onchocerciasis)、藥物過敏反應 (drug hypersensitivity reactions)、瀰漫性紅斑 (diffuse erythema)、tinea 感染、異位性濕疹 (atopic eczema)、過敏性接觸性皮膚炎 (allergic contact dermatitis)、蕁麻疹性血管炎 (urticarial vasculitis)、eosinophilic pustular folliculitis、bullous pemphigoid、herpes gestationis、hypereosinophilic syndrome 及皮膚肥大細胞瘤 (cutaneous mastocytoma)。顯著的火焰圖像也可見於口腔黏膜的嗜酸性潰瘍 (eosinophilic ulcer of the oral mucosa)。
- 應強調的是,在寄生蟲感染流行的地區,具有嗜酸性蜂窩組織炎組織學外觀的病灶極有可能代表寄生蟲感染,例如梨形鞭毛蟲病 (giardiasis)、弓蛔蟲病 (toxocariasis) 及蟠尾絲蟲病 (onchocerciasis)。在嗜酸性筋膜炎 (eosinophilic fasciitis) 中,深部真皮的瀰漫性纖維化 (diffuse fibrosis) 並延伸至皮下脂肪的纖維間隔 (fibrous septa) 以及筋膜 (fascia) 受累,使其易於與 Wells syndrome 區分。