Eosinophilic cellulitis
Eosinophilic cellulitis
Clinical features Eosinophilic cellulitis (Wells syndrome) is an uncommon disorder, characterized by recurrent erythematous and edematous plaques.1–6 It occurs with an equal sex ratio, and there is a large age range, with a mean age of 37 years.7 It is sometimes also encountered in children and rare cases have been documented in neonates.7–11 It appears that cases occurring in childhood may be particularly severe. Scalp involvement, with alopecia and scarring, is a feature in some patients.7,8
The disease particularly affects the extremities and trunk. Although it presents most commonly as well-defined (cellulitis-like) annular erythematous plaques, which are edematous and firm, a wide variety of clinical appearances have been described including blistering, nodular, papulovesicular eruptions, and itchy excoriated inflammatory papules (Figs 15.49–15.51).7,12–14 The plaques, which cause pain and pruritus in some patients, typically heal without scarring.7 Eosinophilic cellulitis has been associated with urticaria.15 Dermatographism can be a feature.16 With progression, the lesions sometimes adopt a greenish hue. Clinically, the lesion may occasionally be mistaken for an infective process.17 The disease tends to be episodic, with remissions and relapses, which can last from months to years.
Large bullae are seen in rare patients.18 An unusual pattern of involvement following Blaschko lines has been reported, and it has been proposed that this form represents cutaneous mosaicism.19
Rarely, eosinophilic cellulitis is associated with a malignant neoplasm. Cases accompanied by eosinophilic leukemia, colonic carcinoma, squamous cell carcinoma of the lung, and non-Hodgkin lymphoma have been described.20–23 Associations with HIV, hypereosinophilic syndrome, ulcerative colitis, tetanus or thiomersal-containing vaccine, varicella infection, Churg Strauss syndrome, and IgG4-related disease have occasionally been documented.24–33 Some cases of eosinophilic cellulitis appear to be triggered by medications, including antibiotics, anticholinergic agents, anesthetics, non-steroidal anti-inflammatory drugs, thyroid medications, and thiazide diuretics.34 A case associated with a henna tattoo has also been reported.35
Exceptional familial cases have been reported.36,37 In one family, the disease showed an autosomal dominant pattern of inheritance and was
705 Eosinophilic cellulitis
associated with developmental delay and dysmorphic body habitus.36 In another family, the lesions were first noted during infancy.37
Pathogenesis and histologic features The pathogenesis is unknown and may simply represent an eosinophil-rich inflammatory reaction to a variety of insults. The only consistent association appears to be a peripheral eosinophilia, manifested either as an elevated total eosinophil count or as an increased percentage of eosinophils. Clinical activity appears to correlate with increased eosinophil cation protein and IL-5 levels in the peripheral blood in addition to blood and bone marrow eosinophilia.38
and occasionally intraepidermal vesicles are present.39 Early lesions may be indistinguishable from an arthropod bite reaction.41 Over a period of 1–3 weeks, the eosinophils degranulate and degenerate, and eosinophilic material and nuclear debris are deposited on collagen fibers to produce ‘flame figures’ (Fig. 15.55).39–42 Sometimes these are surrounded by histiocytes and multinucleated giant cells (Fig. 15.56). There is no evidence of primary collagen degeneration. It is likely that flame figures represent a non-specific eosinophil reaction pattern to a variety of different provoking stimuli.42 Later, the lesion becomes more granulomatous and giant cells are occasionally prominent.43 Extravasation of red blood cells is sometimes evident, but vasculitis is not usually a feature, except for rare cases reported to evolve into Churg-Strauss syndrome.31,32,40
An elevated ESR is occasionally present. It is possible that some patients represent the benign end of the spectrum of the hypereosinophilic syndrome discussed in the previous section.
Histologically, early lesions of eosinophilic cellulitis are characterized by a diffuse and heavy dermal infiltrate of eosinophils: this occurs either in the superficial dermis, as a bandlike infiltrate, or in the deep dermis with extension into the underlying subcutaneous tissue, fascia, and muscle (Figs 15.52 and 15.53).2,39,40 In addition, lymphocytes and plasma cells may be present. There is sometimes edema of the papillary dermis to such an extent that subepidermal bullae develop (Fig. 15.54).39 The epidermis can be spongiotic
Indirect immunofluorescence studies have shown that flame figures contain extracellular eosinophil granule major basic protein.44 Ultrastructural investigation confirms that the eosinophil granules invest the associated collagen fibers.45 Direct immunofluorescence has demonstrated immunoglobulins and/or complement in blood vessel walls in a minority of cases.2,7,17,42
Differential diagnosis The histologic features of eosinophilic infiltration with ‘flame figures’, although characteristic of Wells syndrome, are not pathognomonic.46 Similar
706 Neutrophilic and eosinophilic dermatoses
category does not form a distinct condition.5,13,33,37 In children, the scalp is particularly involved. There is less of a tendency to affect the seborrheic regions and polycyclic patterns are not evident.30
Eosinophilic pustular folliculitis has been described in association with non-Hodgkin lymphoma, Hodgkin lymphoma, polycythemia rubra vera, myelodysplastic syndrome, bone marrow transplant for aplastic anemia, eosinophilic cellulitis, hepatitis C viral infection, and the nevoid basal cell carcinoma syndrome.13,38–46 A few cases induced by allopurinol, timepidium bromide, carbamazepine, and chemotherapy for breast carcinoma have also been documented.47–50
Pathogenesis and histologic features The etiology and pathogenesis of eosinophil pustular folliculitis are unknown. The possibility of an inherited or contagious cause for the disease has been raised by the observation of the disease in siblings.51 However, there is no firm evidence of an infective cause. A variety of immunological abnormalities have been described including:
• raised IgE levels,
• low immunoglobulin levels,
• defects of neutrophil motility.6,20,33
A pemphigus-like antibody and an antibasal keratinocyte antibody have also been recorded in patients with this disease.52,53
The seborrheic distribution raises a possible role for sebaceous glands in the pathogenesis.10 A lipid-soluble eosinophil chemotactic factor has been identified from epidermal surface lipids.54 The association of eosinophil pustular folliculitis with AIDS (if indeed this is the same disease) raises the interesting possibility of a diminished T-helper lymphocyte-mediated pathogenesis. An increased number of mast cells have been described around hair follicles and sebaceous glands, suggesting a role for these cells in the development of the disease.55 A more recent study demonstrated that prostaglandin synthase may result in sebocyte production of eotaxin, a chemoattractant for eosinophils.56
features may be seen in arthropod bite reactions, spider bites, onchocerciasis, drug hypersensitivity reactions, diffuse erythema, tinea infection, atopic eczema, allergic contact dermatitis, urticarial vasculitis, eosinophilic pustular folliculitis, bullous pemphigoid, herpes gestationis, the hypereosinophilic syndrome, and cutaneous mastocytoma.2,42,47–53 Prominent flame figures are also seen in eosinophilic ulcer of the oral mucosa.54–56 It should be emphasized that in regions where parasitic infections are endemic, lesions with the histologic appearance of eosinophilic cellulitis have a high likelihood of representing parasitic infection such as giardiasis, toxocariasis, and onchocerciasis.57–59 In eosinophilic fasciitis, diffuse fibrosis of the deep dermis with extension into the fibrous septa of the subcutaneous fat and involvement of the fascia allow for easy distinction from Wells syndrome.
In early lesions, spongiosis of the outer root sheath of the infundibulum with an accompanying eosinophil and mononuclear cell infiltrate is characteristic.6,57 As the disease progresses, vesiculation and pustulation are seen deep to the stratum corneum, often extending into the sebaceous gland (Fig. 15.56). The epithelium is infiltrated by large numbers of eosinophils with an admixture of neutrophils and mononuclear cells. In the superficial dermis, there is a perivascular mononuclear and eosinophil infiltrate. Follicular mucinosis has been described.57–62

Fig. 15.49 Eosinophilic cellulitis: there is a large erythematous swollen plaque. The limbs are commonly affected. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
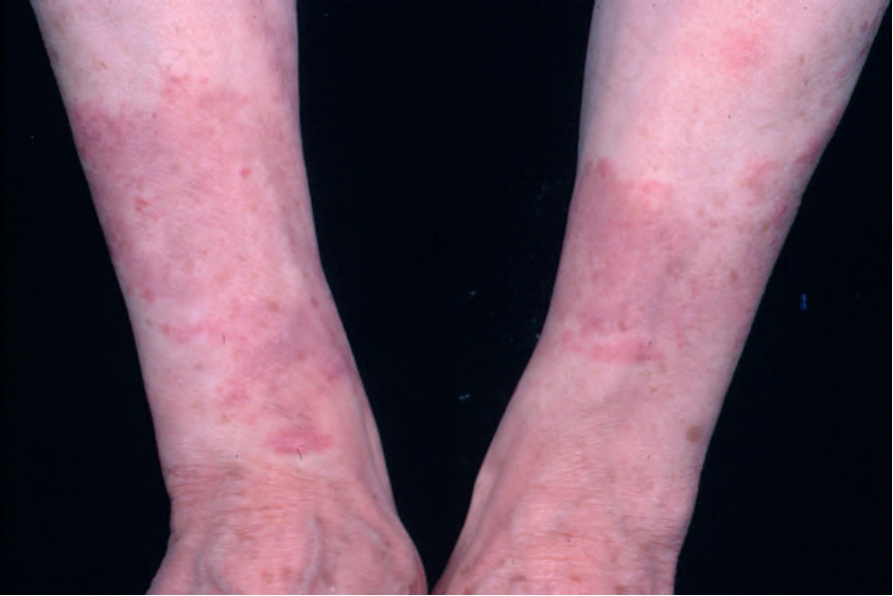
Fig. 15.50 Eosinophilic cellulitis: in this patient, there is striking symmetry. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 15.51 Eosinophilic cellulitis: bullous lesion with a hint of greenish discoloration in the adjacent skin. From the collection of the late N.P. Smith, MD, Institute of Dermatology, London, UK.
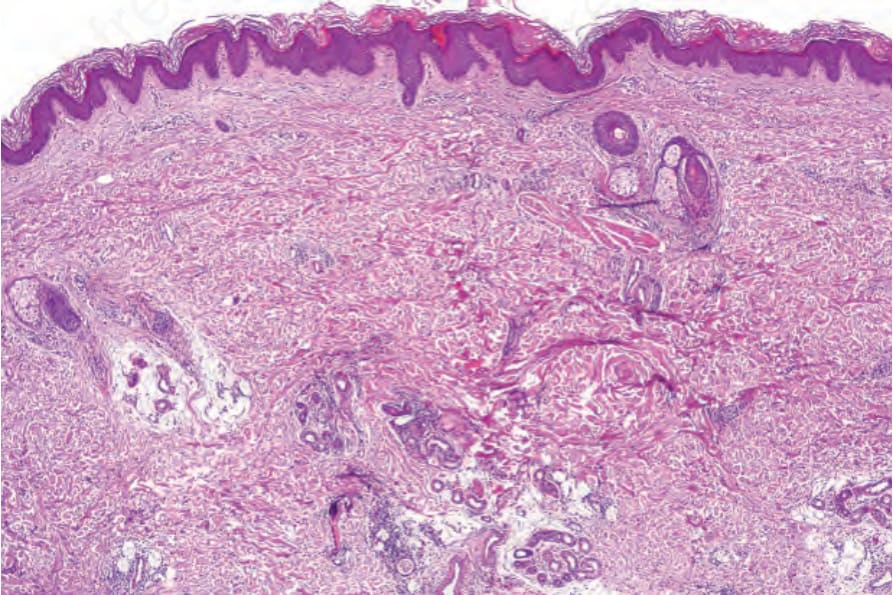
Fig. 15.52 Eosinophilic cellulitis: there is a light, deep dermal chronic inflammatory cell infiltrate. A flame figure is present.
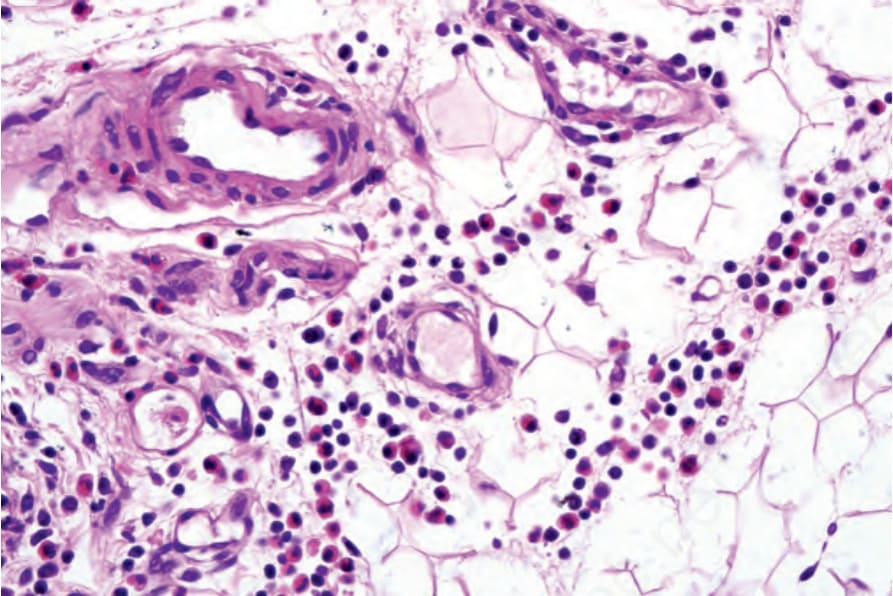
Fig. 15.53 Eosinophilic cellulitis: the infiltrate is composed of lymphocytes and histiocytes with conspicuous eosinophils and extends into the subcutaneous fat.
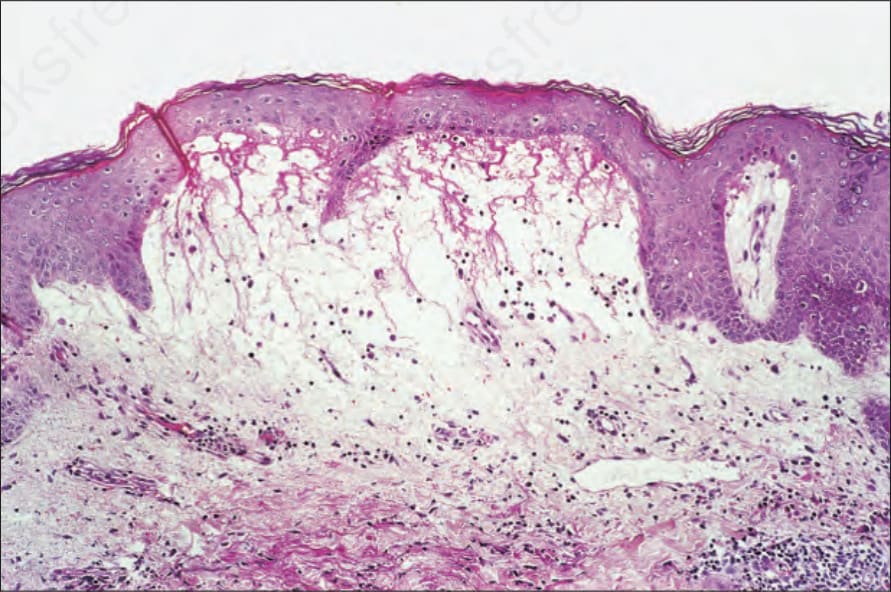
Fig. 15.54 Eosinophilic cellulitis: subepidermal vesiculation as seen here is not uncommon. The blister cavity may contain numerous eosinophils reminiscent of bullous pemphigoid.
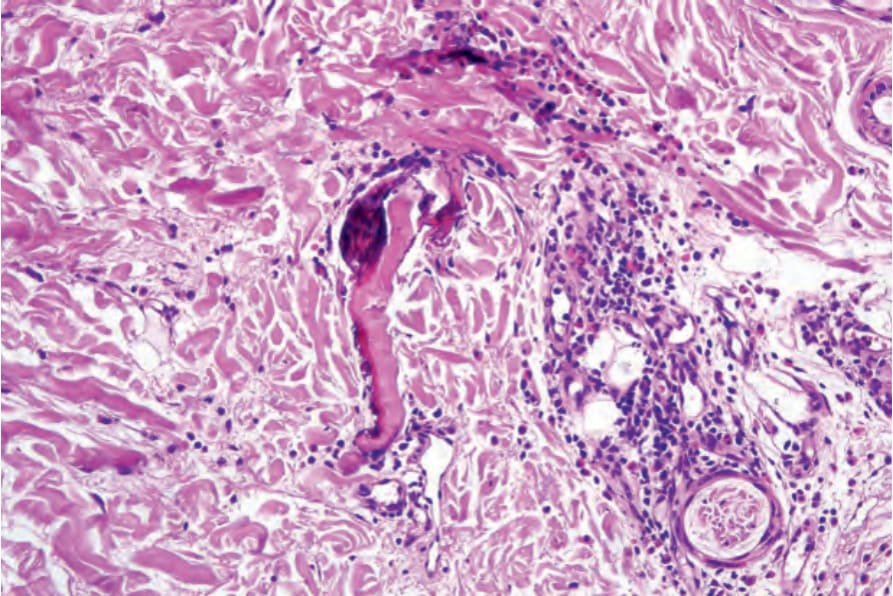
Fig. 15.55 Eosinophilic cellulitis: flame figures are typically present.
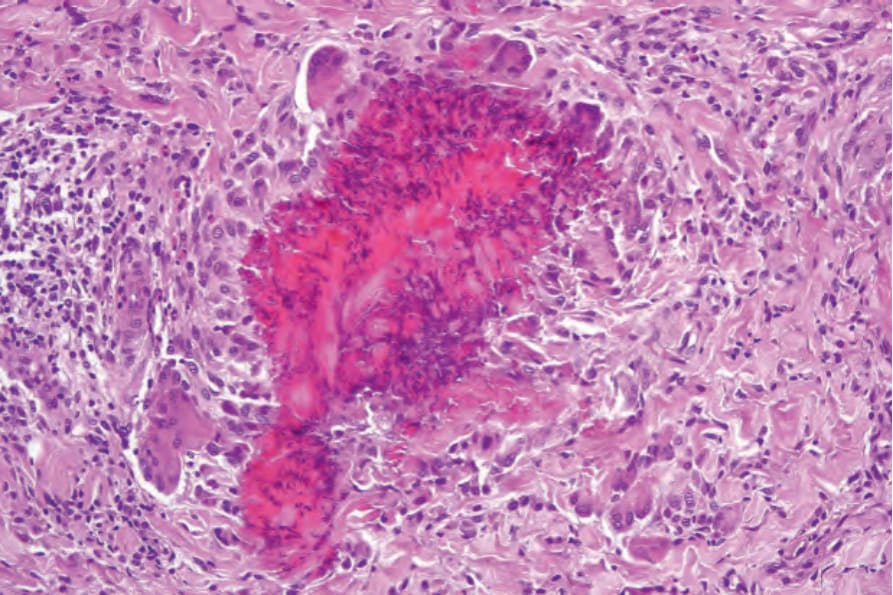
Fig. 15.56 Eosinophilic cellulitis: in this example, a flame figure is surrounded by an intense granulomatous infiltrate.