臨床特徵 (Clinical Features)
- 類風濕性中性球性皮膚炎 (rheumatoid neutrophilic dermatitis) 是一種少見的皮疹,見於罹患類風濕性關節炎 (rheumatoid arthritis) 的患者。
- 最常表現為四肢伸側、頸部與軀幹上的丘疹、結節與斑塊。在某些患者,臨床上可能類似蕁麻疹 (urticaria)。亦曾有報導出現水疱性 (bullous) 與膿疱性 (pustular) 病灶。
- 病灶可發生潰瘍,常伴隨搔癢或疼痛,有時呈環狀 (annular) 構型。本病少見,由文獻記載的情形即可佐證。
- 一般而言,病灶可持續長達數週。在某些患者,病情會自行緩解;在另一些患者,則對 steroid、dapsone 或 sulfamethoxypyridamine 治療有反應。
- 近期已有報導:血清陰性關節炎 (seronegative arthritis) 患者出現與 rheumatoid neutrophilic dermatitis 類似的皮膚表現。
- Magro 與 Crowson 描述了一種無菌性中性球性毛囊炎 (sterile neutrophilic folliculitis),其組織學類似 Sweet 症候群 (Sweet syndrome),發生於包含類風濕性關節炎、Crohn disease、結締組織病 (connective tissue disease)、肝炎、Behçet disease、異位性體質 (atopy)、血液惡液質 (hematological dyscrasia) 與分枝桿菌感染 (mycobacterial infection) 等全身性疾病的背景下。在潰瘍性結腸炎 (ulcerative colitis) 患者中也記載過類似的以毛囊為中心 (folliculocentric) 的急性發炎過程。這些報導似乎很可能反映了一種類似的病況或疾病譜,可能共享共同的組織病理發生機制。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- rheumatoid neutrophilic dermatitis 的致病機轉尚未充分了解,但有些作者認為它可能代表一種免疫複合體媒介 (immune complex-mediated) 的疾病。它很可能與一種自體發炎性疾病 (autoinflammatory disease) 相關,涉及 IL-1、TNF-α 及其他細胞激素 (cytokines) 的組合,與其他中性球性皮膚病 (neutrophilic dermatoses) 類似。
- 組織學上,本病的特徵為真皮內中性球浸潤,伴有程度不一的核破裂 (karyorrhexis)(圖 15-23)。然而在某些病例,核破裂極微或缺如。可能出現數量不等的組織球 (histiocytes)、漿細胞 (plasma cells) 與嗜酸性球 (eosinophils);有時以膿瘍形成 (abscess formation) 為特徵。發炎浸潤偶爾會延伸至皮下脂肪。其上覆的表皮可能顯示海綿水腫 (spongiosis) 與表皮內水疱形成 (intraepidermal vesiculation)(圖 15-24)。
- 壞疽性膿皮症 (pyoderma gangrenosum) 可能顯示類似、甚至完全相同的特徵,但其區別在於進行性潰瘍。應記得類風濕性關節炎患者也可能發生 pyoderma gangrenosum。臨床對照對於區分這些病種是必要的。pyoderma gangrenosum 可能構成一個連續譜的一部分,最終或許證實共享相似的致病機制。對於持此觀點者而言,記載到一位同時具有 pyoderma gangrenosum 與 rheumatoid neutrophilic dermatitis 典型特徵的患者,並不令人意外。
- 有些作者指出,rheumatoid neutrophilic dermatitis 或可歸類為 Sweet syndrome 的一種變異型。誠然,切片發現可能非常相似。缺乏 Sweet syndrome 所伴隨的發燒與全身倦怠是區別性的臨床發現。胃腸道疾病的存在可將 rheumatoid neutrophilic dermatitis 與 BADAS 區分開來。如同 pyoderma gangrenosum,人們或可將 Sweet syndrome 與 rheumatoid neutrophilic dermatitis 視為構成一個疾病譜。正是這些特徵性的臨床背景,使得這些病症得以被區分。
鑑別診斷 (Differential Diagnosis)
- 鑑別診斷中必須考慮感染,尤其因為患者常由於免疫抑制治療而處於感染風險中。此外,皮膚皮疹可能以 steroid 治療,而未能診斷出潛在的感染過程可能導致災難性後果。針對微生物的 Gram、AFB/抗酸 (acid fast) 與銀染色 (silver stains) 應常規進行,且僅在排除感染後才作出診斷。我們曾遇到數位接受 steroid 治療的類風濕性關節炎患者,發生與 Mycobacterium chelonae 感染相關的膿疱性浸潤。
- 類風濕性關節炎患者有時會發生與 rheumatoid neutrophilic dermatitis 在組織學上重疊的病灶,但可藉由存在柵欄狀壞死性與肉芽腫性成分(稱為 palisaded neutrophilic granulomatous dermatitis)加以區別。此疾病譜亦包含在全身性疾病(包括類風濕性關節炎)背景下所見的間質性肉芽腫性皮膚炎 (interstitial granulomatous dermatitis)。患者以成人為主,表現為丘疹與結節,特別侵犯四肢或軀幹;這些病灶常呈線狀 (linear) 分布。除了急性發炎與程度不一的核破裂之外,伴隨組織球反應(讓人聯想到環狀肉芽腫 (granuloma annulare) 或類脂質壞死 (necrobiosis lipoidica))的壞死 (necrobiosis) 之存在,有助於將這些病灶與典型的 rheumatoid neutrophilic dermatitis 區分。曾有一例描述發生於一位接受 adalimumab 治療的類風濕性關節炎患者。
- 中性球浸潤伴隨真皮乳頭膿瘍形成 (dermal papillary abscess formation) 的病灶,可能被誤認為疱疹樣皮膚炎 (dermatitis herpetiformis)、線狀 IgA 疾病 (linear IgA disease) 與水疱性 SLE (bullous SLE)。在疑難病例中可能需要進行 IMF 染色。
- 血管壞死與纖維素樣變化 (fibrinoid change) 的存在,可將 rheumatoid neutrophilic dermatitis 與血管炎 (vasculitis) 區分開來。必須強調,仔細搜尋血管炎的證據並非僅是學術性的工作,因為類風濕性關節炎患者也有發生血管炎的風險。事實上,類風濕性關節炎患者可能表現出組織學上顯示血管外柵欄狀肉芽腫 (extravascular palisading granulomas)、瀰漫性中性球浸潤,或血管炎(中性球性、淋巴球性或肉芽腫性)的病灶。不同的型態可能彼此重疊,分類應依據主要的組織學型態。
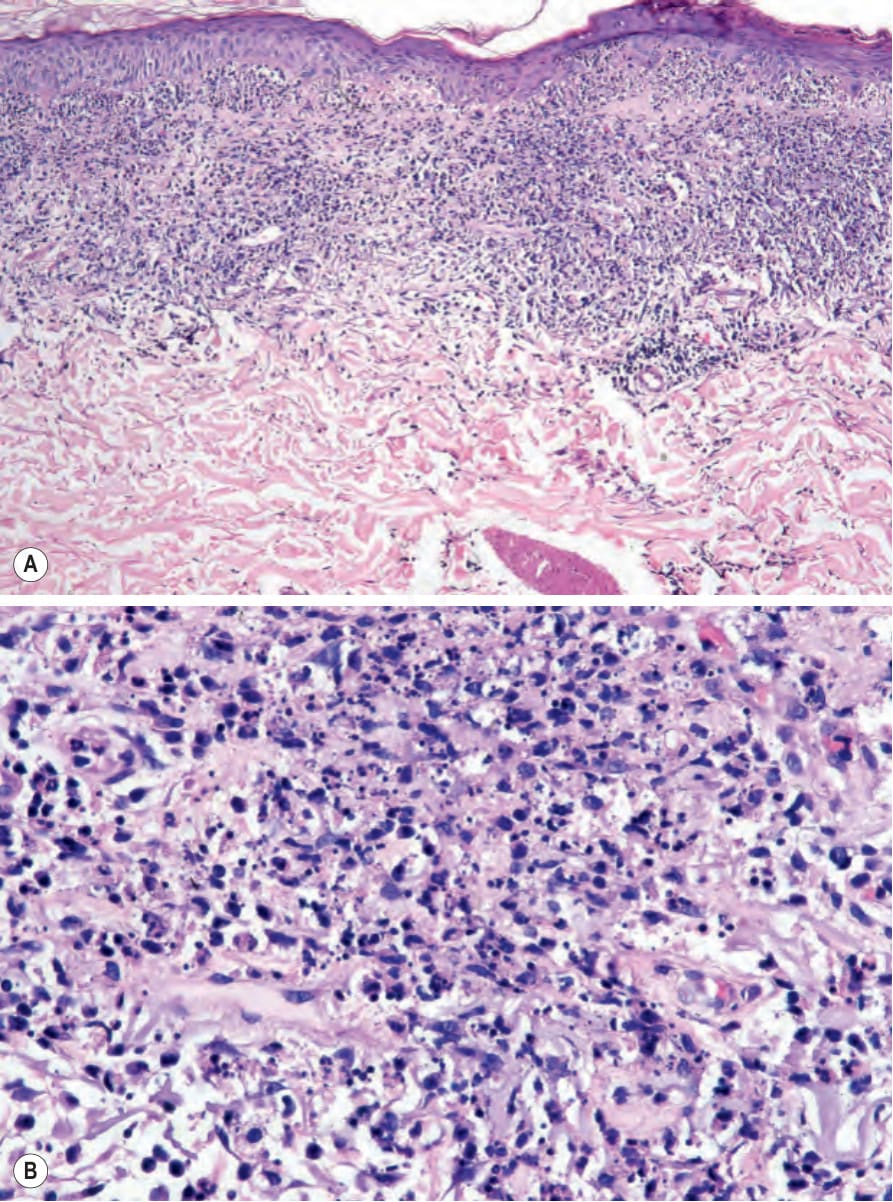
圖 15-23:(A, B) 類風濕性中性球性皮膚炎 (rheumatoid neutrophilic dermatitis):可見上真皮處密集的中性球浸潤,伴有明顯的核破裂 (karyorrhexis)。承蒙 J. Cohen, MD, Dermatopathology Laboratory, Tucson, USA 提供。
Fig. 15.23 (A, B) Rheumatoid neutrophilic dermatitis: there is an intense upper dermal neutrophilic infiltrate with conspicuous karyorrhexis. By courtesy of J. Cohen, MD, Dermatopathology Laboratory, Tucson, USA.
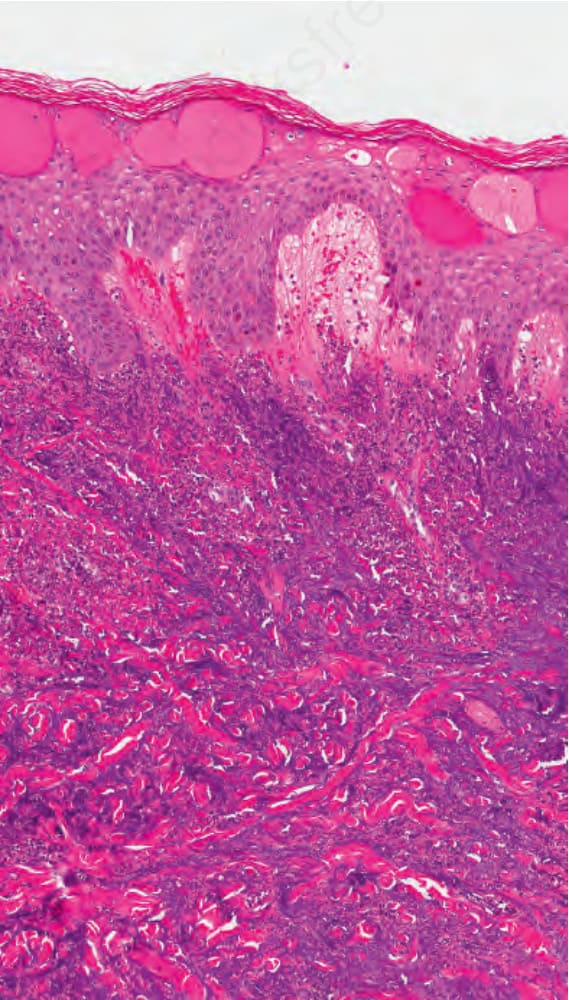
圖 15-24:類風濕性中性球性皮膚病 (rheumatoid neutrophilic dermatosis):在某些病例,表皮可見明顯的海綿水腫 (spongiosis) 並伴有微小水疱形成 (microvesicle formation)。承蒙 Dr. Jennifer S. Ko, MD, PhD, Cleveland Clinic, Cleveland, USA 提供。
Fig. 15.24 Rheumatoid neutrophilic dermatosis: in some cases, there is prominent spongiosis of the epidermis with microvesicale formation. By courtesy of Dr. Jennifer S. Ko, MD, PhD, Cleveland Clinic, Cleveland, USA.

圖 15-25:水疱性昆蟲叮咬反應 (bullous insect bite reaction):此小腿近距離視野中可見大型充滿液體的水疱 (bullae)。From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK。
Fig. 15.25 Bullous insect bite reaction: there are large fluid-filled bullae in this close-up view from the lower leg. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 15-26:蜘蛛叮咬 (spider bite):注意中央的焦痂 (eschar) 與周圍的紅斑。Courtesy of Al Mahmoud, MD, Doha, Qatar。
Fig. 15.26 Spider bite: note the central eschar and surrounding erythema. Courtesy of Al Mahmoud, MD, Doha, Qatar.