Rheumatoid neutrophilic dermatitis
Rheumatoid neutrophilic dermatitis
Clinical features Rheumatoid neutrophilic dermatitis is an uncommon eruption seen in patients with rheumatoid arthritis.1 It presents most often as papules, nodules, and plaques on the extensor surfaces of the extremities, neck, and trunk. In some patients, it may clinically resemble urticaria.2–7 Bullous and pustular lesions have also been described.8–11 The lesions, which can ulcerate, are often pruritic or painful, and sometimes show an annular configuration.3,12,13 The disease is uncommon, as evidenced by documentation in
Typically, lesions last for up to several weeks.2 In some patients, the condition resolves spontaneously; in others, it responds to steroid, dapsone, or sulfamethoxypyridamine therapy.2,5,12
Patients with seronegative arthritis but with cutaneous findings similar to rheumatoid neutrophilic dermatitis have recently been reported.15–18
Magro and Crowson have described sterile neutrophilic folliculitis associated with a Sweet syndrome-like histology in a setting of systemic disease including rheumatoid arthritis, Crohn disease, connective tissue disease, hepatitis, Behçet disease, atopy, hematological dyscrasia, and mycobacterial infection.19 A similar folliculocentric acute inflammatory process has also been documented in patients with ulcerative colitis.20,21 It would seem probable that these reports reflect a similar condition or spectrum of disease that likely shares common histopathogenetic mechanisms.
692 Neutrophilic and eosinophilic dermatoses
A
B
Pathogenesis and histologic features The pathogenesis of rheumatoid neutrophilic dermatitis is not well understood, but some authors have suggested that it may represent an immune complex-mediated disease.3,5 Likely, it is related to autoinflammatory disease related to a combination of IL-1, TNF-α and other cytokines similar to other neutrophilic dermatoses.22
Histologically, it is characterized by a dermal neutrophilic infiltrate with variable karyorrhexis (Fig. 15.23). In some cases, however, karyorrhexis is minimal or absent. Variable numbers of histiocytes, plasma cells, and eosinophils may be present; abscess formation is sometimes a feature.2,3,5 Occasionally, the inflammatory infiltrate extends into the subcutaneous fat.3,7 The overlying epidermis may show spongiosis and intraepidermal vesiculation (Fig. 15.24).5
Pyoderma gangrenosum may show similar, if not identical, features but differs by progressive ulceration. It should be remembered that patients with rheumatoid arthritis may also develop pyoderma gangrenosum.4 Clinical correlation is necessary to distinguish these entities. Pyoderma gangrenosum may form part of a continuum that may eventually prove to share similar pathogenetic mechanisms. To those who hold this view, documentation of a patient with concurrent typical features of both pyoderma gangrenosum and rheumatoid neutrophilic dermatitis should not be surprising.23
Some authors have pointed out that rheumatoid neutrophilic dermatitis might be classified as a variant of Sweet syndrome.2 Certainly, the biopsy findings may be very similar. The lack of fever and the general malaise that accompany Sweet syndrome are distinguishing clinical findings. The presence of gastrointestinal disease distinguishes rheumatoid neutrophilic dermatitis from BADAS. As with pyoderma gangrenosum, one might consider Sweet syndrome and rheumatoid neutrophilic dermatitis to form a spectrum of disease.2 It is the characteristic clinical settings that allow these disorders to be distinguished.
Differential diagnosis Infection must be considered in the differential diagnosis, particularly as patients are often at risk of infection as a result of immunosuppressive therapy. Furthermore, the cutaneous eruption may be treated with steroids, and failure to diagnose an underlying infective process could have disastrous consequences. Gram, AFB/acid fast, and silver stains for microorganisms should be routinely performed and the diagnosis made only after infection has been excluded. We have encountered several patients with rheumatoid arthritis on steroid therapy who developed pustular infiltrates associated with Mycobacterium chelonae infection.
Patients with rheumatoid arthritis may sometimes develop lesions which show histologic overlap with rheumatoid neutrophilic dermatitis but which can be distinguished by the presence of a palisading necrobiotic and granulomatous component (termed palisaded neutrophilic granulomatous dermatitis).24 This spectrum also includes interstitial granulomatous dermatitis encountered in a setting of systemic disease (including rheumatoid arthritis). Patients, predominantly adults, present with papules and nodules which particularly affect the extremities or trunk; these are often distributed in a linear pattern.25,26 The presence of necrobiosis associated with a histiocytic response reminiscent of granuloma annulare or necrobiosis lipoidica in addition to acute inflammation and variable karyorrhexis helps distinguish these lesions from typical rheumatoid neutrophilic dermatitis. A case has been described in a patient with rheumatoid arthritis treated with adalimumab.27
693 Arthropod and arachnid bite reactions
Lesions in which the neutrophilic infiltrate is associated with dermal papillary abscess formation may be mistaken for dermatitis herpetiformis, linear IgA disease, and bullous SLE. IMF staining may be necessary in problematic cases.
The presence of vascular necrosis and fibrinoid change distinguishes rheumatoid neutrophilic dermatitis from vasculitis.28 It must be emphasized that a careful search for evidence of vasculitis is not simply an academic exercise, since patients with rheumatoid arthritis are also at risk of developing vasculitis. In fact, patients with rheumatoid arthritis may present with lesions histologically showing extravascular palisading granulomas, diffuse neutrophilic infiltrates, or vasculitis (neutrophilic, lymphocytic, or granulomatous). The different patterns may overlap, and classification should be based on the dominant histologic pattern.
vernacular name of ‘fiddleback’ spider.8 Most bites are seasonal, occurring between the months of April and October.9 However, other spiders are often misidentified as brown recluse, and the diagnosis may be overused as the spider is often not identified at the time of the bite.10–14 This makes much of the existing literature suspect.15
Phospholipase D/sphingomyelinase-D in the venom of the brown recluse spider is thought to be responsible for the extensive necrosis that results in some patients.16,17 Spider bites may be associated with morbilliform rash, malaise, fever, nausea, hemoglobinuria, arthralgias, and vomiting.6,18–20 More serious complications (e.g., renal failure, shock, disseminated intravascular coagulation, acute hemolytic anemia, intravascular hemolysis, and a single case of bilateral optic neuropathy) have also been described.18,21–26 Many of the effects of the venom appear to be dose-dependent rather than idiosyncratic.27,28 ELISA-based assays to detect the Loxosceles venom at the site of the bite are available and can be helpful to confirm the diagnosis, as detectable toxin may persist for more than 2 weeks.29–33 Anti-loxoscelic sera are available for use in severe cases.34,35
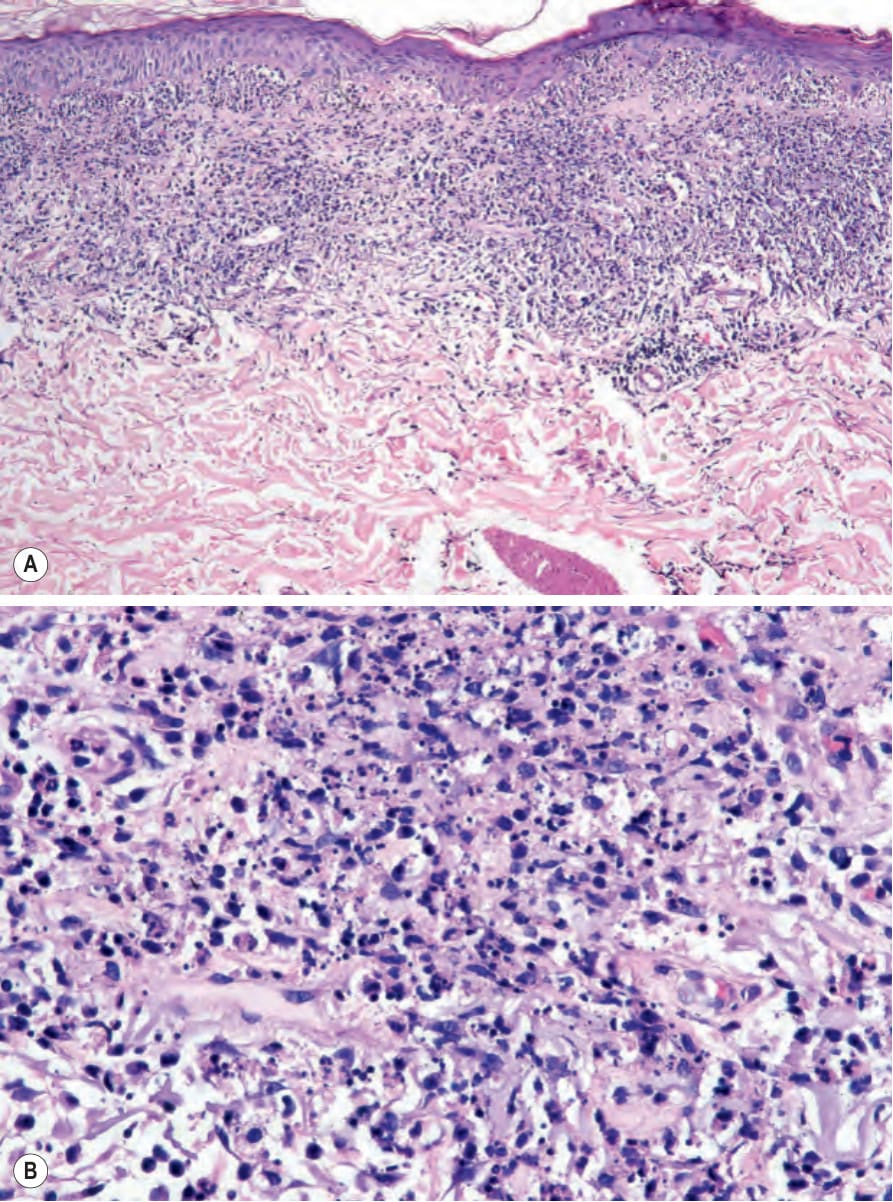
Fig. 15.23 (A, B) Rheumatoid neutrophilic dermatitis: there is an intense upper dermal neutrophilic infiltrate with conspicuous karyorrhexis. By courtesy of J. Cohen, MD, Dermatopathology Laboratory, Tucson, USA.
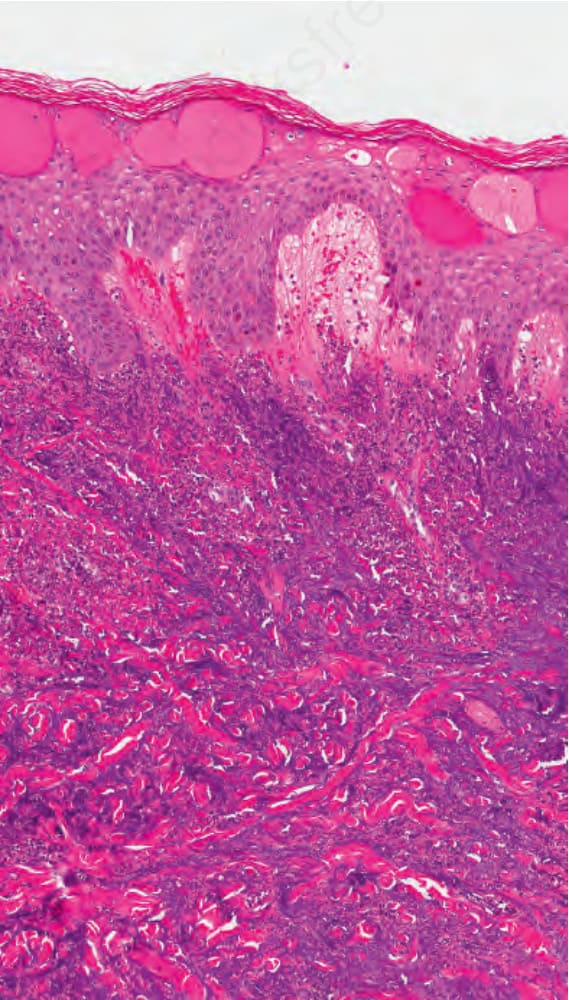
Fig. 15.24 Rheumatoid neutrophilic dermatosis: in some cases, there is prominent spongiosis of the epidermis with microvesicale formation. By courtesy of Dr. Jennifer S. Ko, MD, PhD, Cleveland Clinic, Cleveland, USA.

Fig. 15.25 Bullous insect bite reaction: there are large fluid-filled bullae in this close-up view from the lower leg. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 15.26 Spider bite: note the central eschar and surrounding erythema. Courtesy of Al Mahmoud, MD, Doha, Qatar.