發疹型反應 (Exanthematous Reactions)
臨床特徵 (Clinical Features)
- 發疹型 (exanthematous,亦稱 morbilliform、maculopapular) 反應是最常見的藥物不良反應,占所有皮膚反應的 51% 至 95%,並可模擬多種感染性疾病,包括猩紅熱 (scarlet fever)、麻疹 (measles) 與德國麻疹 (rubella)(圖 14.1 與 14.2)。1–5 病人表現為紅斑性斑疹 (erythematous macules) 與丘疹 (papules),這些病灶可能融合或呈迴旋狀/多環狀 (gyrate/polycyclic)。有時會出現搔癢 (pruritus)、低度發燒 (low-grade fever) 與嗜伊紅性白血球增多 (eosinophilia)。2 皮疹常呈對稱性,通常出現於軀幹與四肢,或壓迫與外傷部位。1 手掌與腳掌有時會受侵犯,但黏膜通常不會被侵犯。
- 發疹型皮疹通常於開始用藥後 1–2 週內出現。1 偶爾,皮疹會延遲發生,甚至可能在停藥後才出現。1,6 在較嚴重的病人中,皮疹可能進展為紅皮症 (erythroderma,即剝脫性皮膚炎 [exfoliative dermatitis]),此時紅斑變得全身性,且常伴隨脫屑 (scaling)。7 發疹型藥物反應的緩解以脫皮 (exfoliation) 為特徵,有時隨後出現發炎後色素增加或減少 (postinflammatory hyper- or hypopigmentation)。1
- penicillin、sulfonamides、ampicillin、amoxicillin、phenylbutazone、isoniazid、barbiturates、phenytoin、carbamazepine、benzodiazepines、gold 與 trimethoprim 特別容易被歸咎,但廣泛的各種藥物都可誘發發疹型藥物疹。1,8–11 罹患傳染性單核球增多症 (infectious mononucleosis) 的病人,在接受 ampicillin 或 amoxicillin 治療後有發生發疹型反應的風險。12 膳食補充品 (dietary supplements) 亦可誘發類似的皮膚皮疹。13
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- 發疹型藥物反應的致病機轉尚未完全明瞭,雖然在多數病例中很可能是細胞毒性 T 細胞媒介 (cytotoxic T-cell-mediated) 的反應(見下文)。
- 組織學特徵通常很細微。雖然表皮可能看似正常,但局部角化不全 (focal parakeratosis) 常常出現。特徵性的變化包括淋巴球外移 (lymphocytic exocytosis) 伴隨輕度海綿水腫 (mild spongiosis),典型上伴有基底細胞液化變性 (basal cell liquefactive degeneration) 及少數異常角化 (dyskeratotic) 角質細胞(圖 14.3–14.7)。14,15 在某些病例中,組織學上看不到界面變化 (interface change)。真皮顯示淋巴球與組織球 (histiocytes) 的血管周圍浸潤,伴隨數量不等的嗜伊紅性白血球。嗜伊紅性白血球——雖然在文獻中常被強調為藥物反應的重要特徵——但依我們的經驗,它們可能非常稀少甚至完全缺如。有時可見明顯水腫,尤其在臨床上有蕁麻疹性 (urticarial) 成分時。在含有紫斑性 (purpuric) 成分的病灶中,紅血球外滲 (red cell extravasation) 也可能是一項特徵。
- 經免疫組織化學,這些淋巴球主要為 CD3+ T 細胞,在淺層血管周圍浸潤中以 CD4+ 細胞為主。16 位於真皮–表皮交界處 (dermal–epidermal junction) 及表皮內的淋巴球,由大約等量的 CD4+ 與 CD8+ 型態組成。16–21 後者這些細胞經常表現人類白血球抗原 (human leukocyte antigen, HLA)-DR,且其中一個亞群亦表現 CD25。21 其中混雜有 T 輔助型 Th1 與 Th2 細胞。20 偶爾,浸潤幾乎完全由 CD4+ 淋巴球組成;相反地,在人類免疫缺乏病毒 (human immunodeficiency virus, HIV) 陽性病人中,浸潤可能僅由 CD8+ 細胞組成。16,19 亦可見 CD1a+ 樹突細胞 (dendritic cells) 與 CD68+ 組織球。20
- 可辨識出 CD56+ 自然殺手 (natural killer, NK) 細胞。19 由 perforin 與 granzyme B 媒介的細胞毒性途徑已被證實在發疹型藥物反應中特別重要。18,20,21 Fas/Fas-L 細胞毒性機轉則不被認為具有相關性。16
- 藥物誘發紅皮症的特徵相當非特異性,包括角化不全 (parakeratosis) 與乾癬樣增生 (psoriasiform hyperplasia),有時伴隨輕度海綿水腫。真皮慢性發炎細胞浸潤中可辨識出嗜伊紅性白血球。
鑑別診斷 (Differential Diagnosis)
- 發疹型藥物不良反應在移植病人中是常見的特徵,這些病人通常服用多種藥物,因此必須與急性移植物對抗宿主病 (acute GVHD) 區別。實際上,兩者即使不是無法區分,也往往難以區分,雖然嗜伊紅性白血球的存在可能傾向藥物反應。

圖 14-1:發疹型藥物反應 (Exanthematous drug reaction):因 ampicillin 引起、典型的下肢紅斑性斑丘疹皮疹 (erythematous maculopapular eruption)。承蒙倫敦皮膚科研究所 (Institute of Dermatology, London, UK) 提供。
Fig. 14.1 Exanthematous drug reaction: typical erythematous maculopapular eruption on the lower extremities due to ampicillin. By courtesy of the Institute of Dermatology, London, UK.
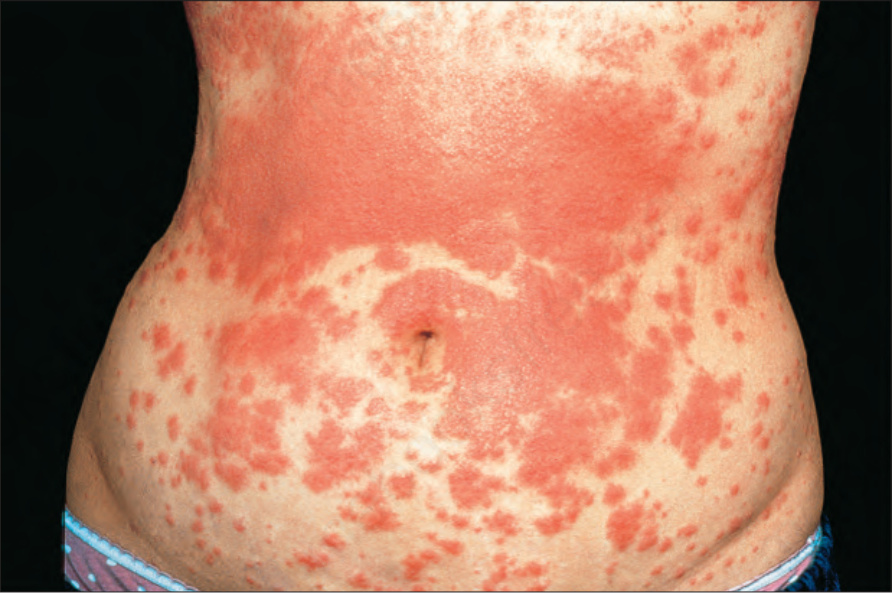
圖 14-2:發疹型藥物反應 (Exanthematous drug reaction):與 amoxicillin 治療相關、腹部較廣泛的病灶。承蒙倫敦皮膚科研究所 (Institute of Dermatology, London, UK) 提供。
Fig. 14.2 Exanthematous drug reaction: more extensive lesions on the abdomen associated with amoxicillin therapy. By courtesy of the Institute of Dermatology, London, UK.
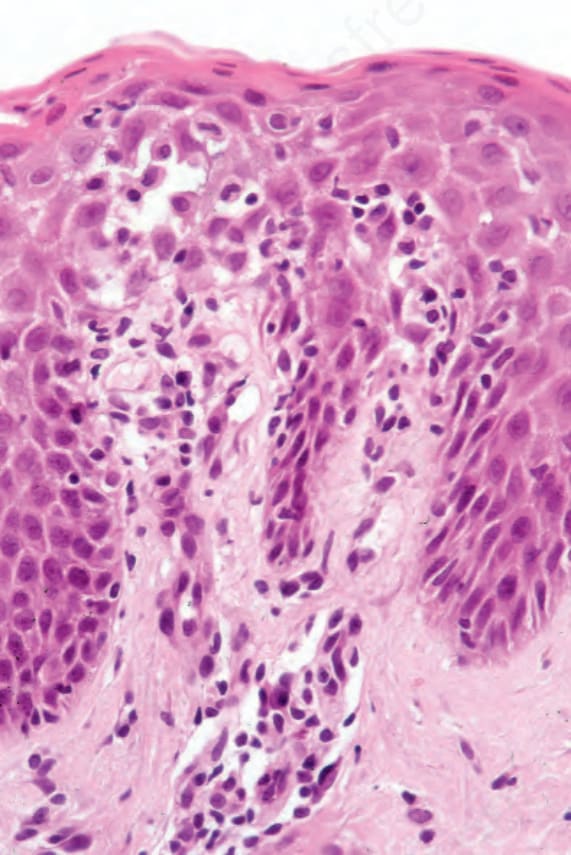
圖 14-3:發疹型藥物反應 (Exanthematous drug reaction):因 penicillin 引起的早期病灶,顯示輕微界面變化 (interface change)、海綿水腫 (spongiosis) 與淋巴球外移 (lymphocytic exocytosis)。可見淺層血管周圍淋巴球浸潤,並有一兩個漿細胞 (plasma cells)。
Fig. 14.3 Exanthematous drug reaction: early lesion due to penicillin showing slight interface change, spongiosis, and lymphocytic exocytosis. There is a superficial perivascular lymphocytic infiltrate, and one or two plasma cells are present.
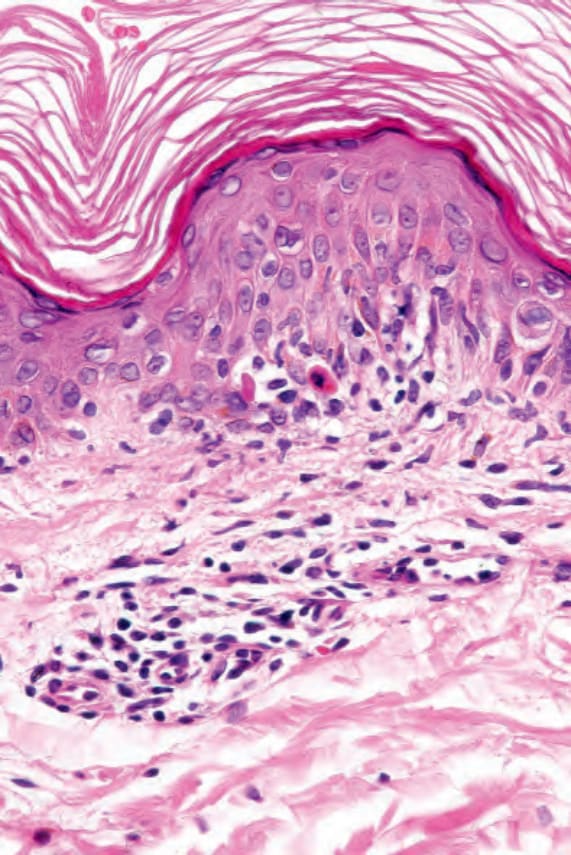
圖 14-4:發疹型藥物反應 (Exanthematous drug reaction):在此例(因 carbamazepine 治療所致),可見海綿水腫 (spongiosis)、異常角化 (dyskeratosis) 與界面變化 (interface change),並伴隨淋巴球外移 (lymphocytic exocytosis)。
Fig. 14.4 Exanthematous drug reaction: in this example, due to carbamazepine therapy, there is spongiosis, dyskeratosis, and interface change associated with lymphocytic exocytosis.
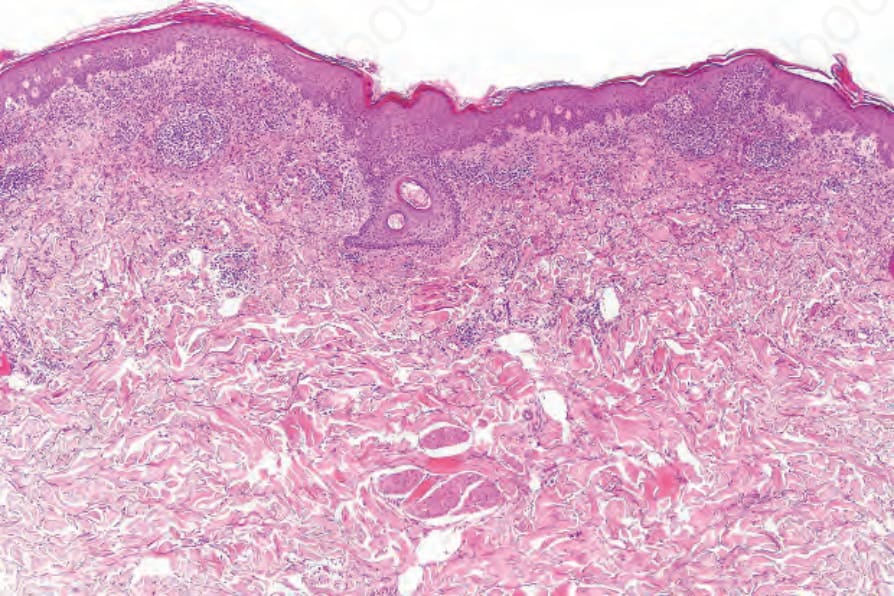
圖 14-5:發疹型藥物反應 (Exanthematous drug reaction):低倍視野顯示局部角化不全 (focal parakeratosis)、輕度棘層肥厚 (mild acanthosis),以及上真皮層大量發炎細胞浸潤。
Fig. 14.5 Exanthematous drug reaction: low-power view showing focal parakeratosis, mild acanthosis, and a heavy upper dermal inflammatory cell infiltrate.
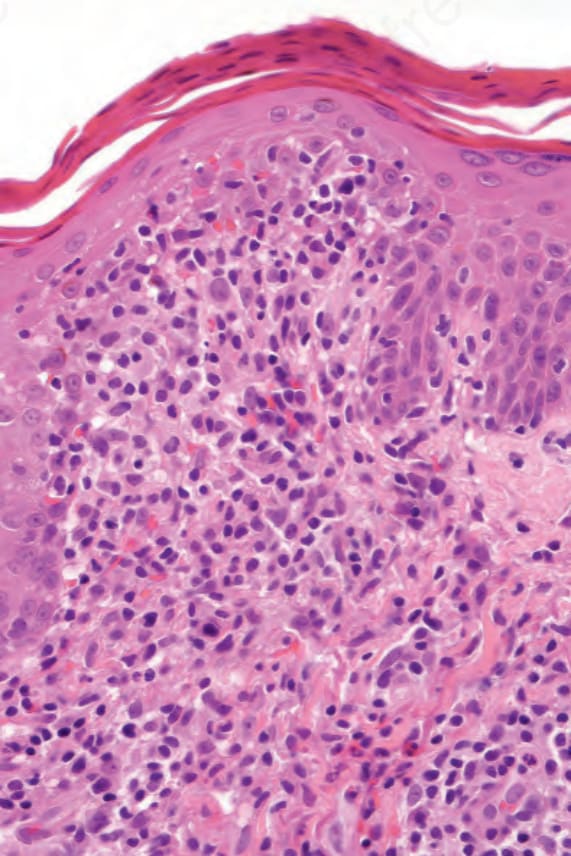
圖 14-6:發疹型藥物反應 (Exanthematous drug reaction):在此高倍視野中,可見角化不全 (parakeratosis)、局部海綿水腫 (focal spongiosis) 與淋巴球外移 (lymphocytic exocytosis)。可見大量真皮浸潤,並有一兩個嗜伊紅性白血球 (eosinophils)。
Fig. 14.6 Exanthematous drug reaction: in this high-power view, there is parakeratosis, focal spongiosis and lymphocytic exocytosis. A heavy dermal infiltrate is present with one or two eosinophils.
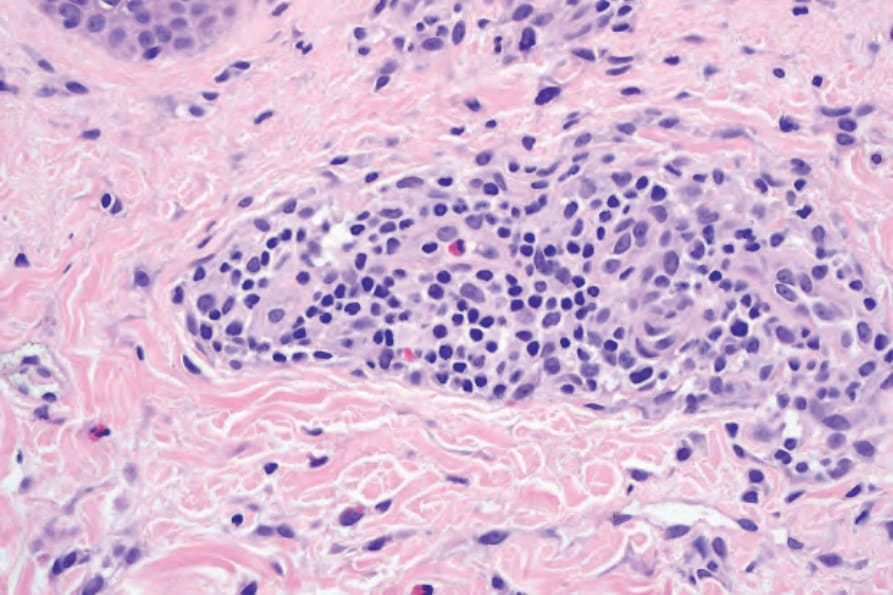
圖 14-8:蕁麻疹性藥物反應 (Urticarial drug reaction):高倍視野顯示以血管周圍為主的淋巴組織球浸潤 (lymphohistiocytic infiltrate),並有一兩個嗜伊紅性白血球 (eosinophils)。
Fig. 14.8 Urticarial drug reaction: high-power view showing a predominately perivascular lymphohistiocytic infiltrate with one or two eosinophils.