Exanthematous reactions
Exanthematous reactions
Clinical features Exanthematous (morbilliform, maculopapular) reactions are the most frequently encountered adverse drug reaction, accounting for 51% to 95% of skin reactions, and mimic a variety of infective conditions including scarlet fever, measles, and rubella (Figs 14.1 and 14.2).1–5 Patients present with erythematous macules and papules that may become confluent or gyrate/polycyclic. Pruritus, low-grade fever, and eosinophilia are sometimes present.2 The eruption is often symmetrical and usually presents on the trunk and extremities or sites of pressure and trauma.1 The palms and soles are sometimes affected but the mucous membranes are not usually involved.
Exanthematous eruptions typically develop within 1–2 weeks of starting the drug.1 Occasionally, the eruption is delayed and may even present after the treatment has ceased.1,6 In more seriously affected patients the eruption can progress to erythroderma (exfoliative dermatitis), in which the erythema becomes generalized and is often accompanied by scaling.7 Resolution of exanthematous drug reactions is characterized by exfoliation and sometimes
Box 14.1 Clinical manifestations of adverse drug reactions
• Exanthematous reactions
• Urticaria, angioedema and anaphylaxis
• Serum sickness
• Phototoxic/photoallergic eruptions
• Hypersensitivity syndrome
• Lichenoid drug reactions
• Fixed drug eruptions
• Erythema multiforme
• Stevens-Johnson syndrome/toxic epidermal necrolysis
• Pigmentary abnormalities
• Vasculitis
• Purpura
• Granulomatous drug reactions
• Erythema nodosum
• Drug-induced alopecia
• Lupus erythematosus-like drug reactions
• Bullous drug reactions
• Psoriasiform drug reactions
• Pityriasis rosea-like eruptions
• Pustular drug reactions
• Ichthyosiform drug reactions
• Pseudolymphomatous drug reactions
• Eczematous drug reactions
636 Cutaneous adverse reactions to drugs
is followed by postinflammatory hyper- or hypopigmentation.1 Penicillin, sulfonamides, ampicillin, amoxicillin, phenylbutazone, isoniazid, barbiturates, phenytoin, carbamazepine, benzodiazepines, gold, and trimethoprim are especially incriminated, but a wide range of medications can induce exanthematous drug eruptions.1,8–11 Patients who suffer from infectious mononucleosis are at risk of developing an exanthematous reaction following therapy with ampicillin or amoxicillin.12 Dietary supplements can also induce a similar cutaneous eruption.13
Pathogenesis and histologic features The pathogenesis of exanthematous drug reactions is not fully understood, although a cytotoxic T-cell-mediated reaction is likely in most cases (see below).
The histologic features are often subtle. Although the epidermis may appear normal, focal parakeratosis is commonly present. The characteristic changes include lymphocytic exocytosis with mild spongiosis, typically accompanied by basal cell liquefactive degeneration and a few dyskeratotic keratinocytes (Figs 14.3–14.7).14,15 In some cases, no interface change is histologically apparent. The dermis shows a perivascular infiltrate of lymphocytes and histiocytes with variable numbers of eosinophils. Eosinophils – although often emphasized in the literature as an important feature of drug reactions – can, in our experience, be very scanty or even absent. Sometimes marked edema is seen, particularly if an urticarial element is clinically evident. Red cell extravasation may also be a feature in those lesions that include a purpuric component.
By immunohistochemistry, the lymphocytes are largely CD3+ T-cells with a predominance of CD4+ cells in the superficial perivascular infiltrate.16 Lymphocytes at the dermal–epidermal junction and within the epidermis consist of approximately equal numbers of CD4+ and CD8+ forms.16–21 These latter cells regularly express human leukocyte antigen (HLA)-DR and a subpopulation also expresses CD25.21 There is an admixture of T-helper Th1 and Th2 cells.20 Occasionally, the infiltrate is almost entirely composed of the CD4+ lymphocytes and, contrariwise in human immunodeficiency virus (HIV)-positive patients, the infiltrate may consist of CD8+ cells alone.16,19 CD1a+ dendritic cells and CD68+ histiocytes are also present.20
CD56+ natural killer (NK) cells may be identified.19 Cytotoxic pathways mediated by perforin and granzyme B have been shown to be of particular importance in exanthematous drug reactions.18,20,21 Fas/Fas-L cytotoxic mechanisms are not thought to be of relevance.16
The features of drug-induced erythroderma are rather non-specific and include parakeratosis and psoriasiform hyperplasia, sometimes accompanied by mild spongiosis. Eosinophils may be identified within the dermal chronic inflammatory cell infiltrate.
Differential diagnosis Exanthematous adverse drug reactions are a frequent feature in transplantation patients who are usually taking multiple medications and, therefore, must be distinguished from acute GVHD. In reality, it is difficult, if not
637 Serum sickness/serum sickness-like drug reactions
often indistinguishable although the presence of eosinophils may favor a drug reaction.

Fig. 14.1 Exanthematous drug reaction: typical erythematous maculopapular eruption on the lower extremities due to ampicillin. By courtesy of the Institute of Dermatology, London, UK.
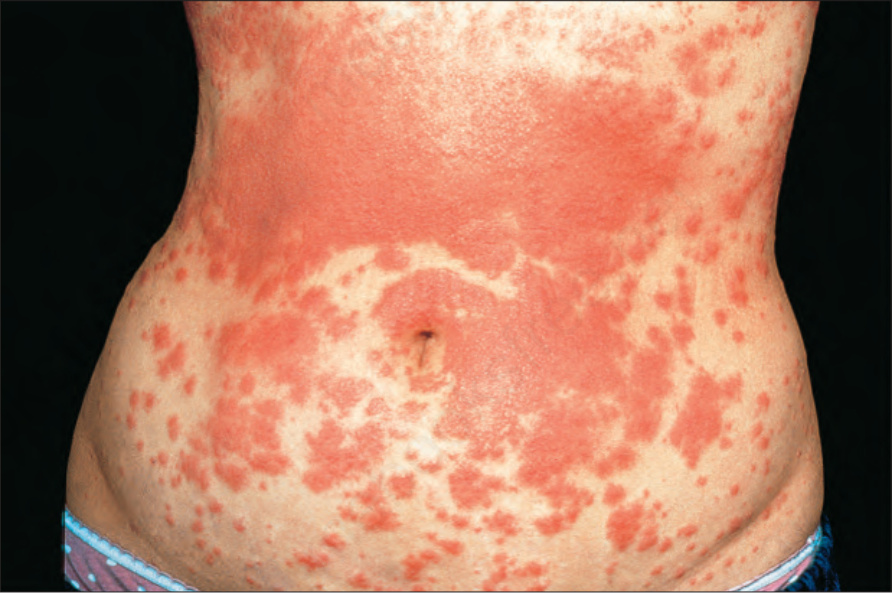
Fig. 14.2 Exanthematous drug reaction: more extensive lesions on the abdomen associated with amoxicillin therapy. By courtesy of the Institute of Dermatology, London, UK.
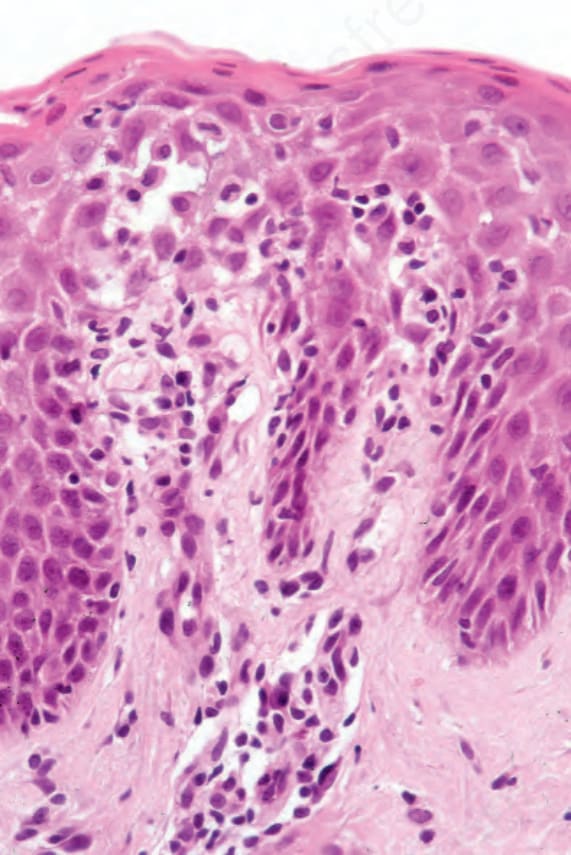
Fig. 14.3 Exanthematous drug reaction: early lesion due to penicillin showing slight interface change, spongiosis, and lymphocytic exocytosis. There is a superficial perivascular lymphocytic infiltrate, and one or two plasma cells are present.
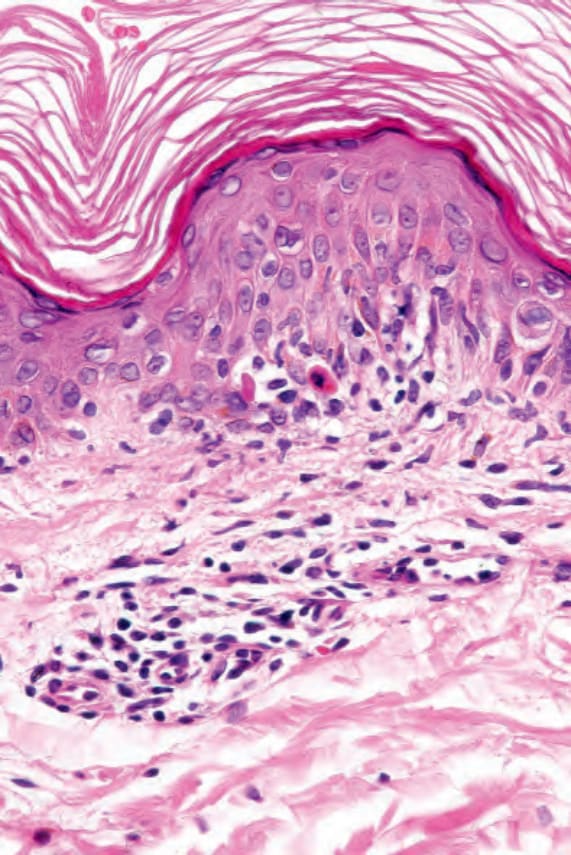
Fig. 14.4 Exanthematous drug reaction: in this example, due to carbamazepine therapy, there is spongiosis, dyskeratosis, and interface change associated with lymphocytic exocytosis.
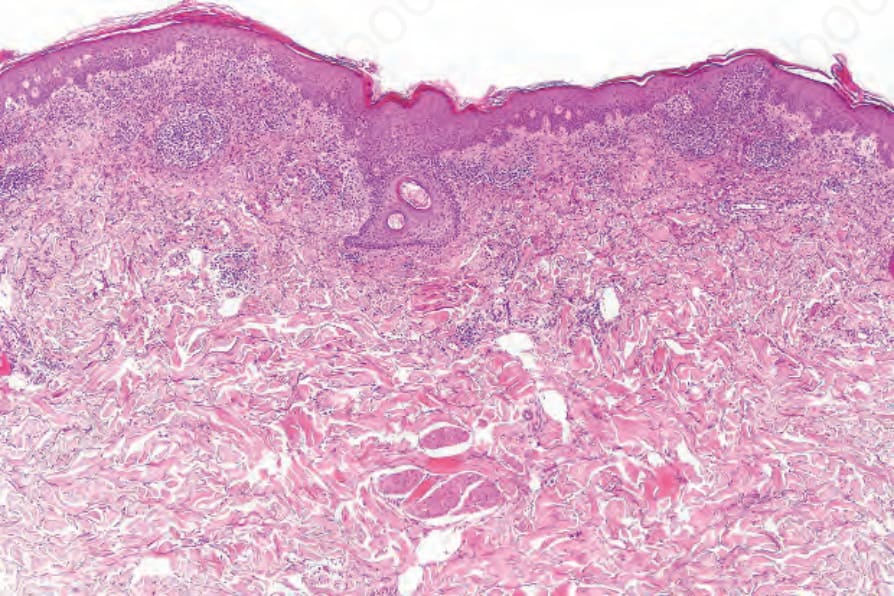
Fig. 14.5 Exanthematous drug reaction: low-power view showing focal parakeratosis, mild acanthosis, and a heavy upper dermal inflammatory cell infiltrate.
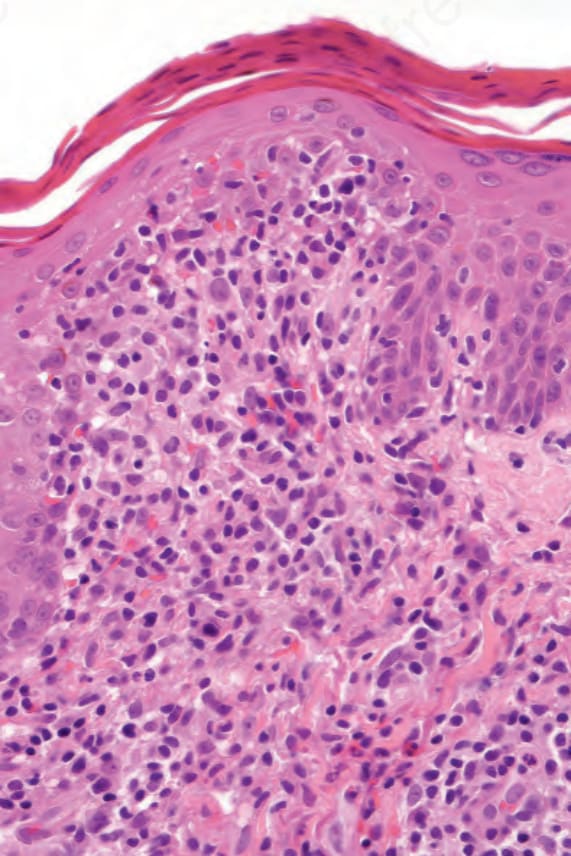
Fig. 14.6 Exanthematous drug reaction: in this high-power view, there is parakeratosis, focal spongiosis and lymphocytic exocytosis. A heavy dermal infiltrate is present with one or two eosinophils.
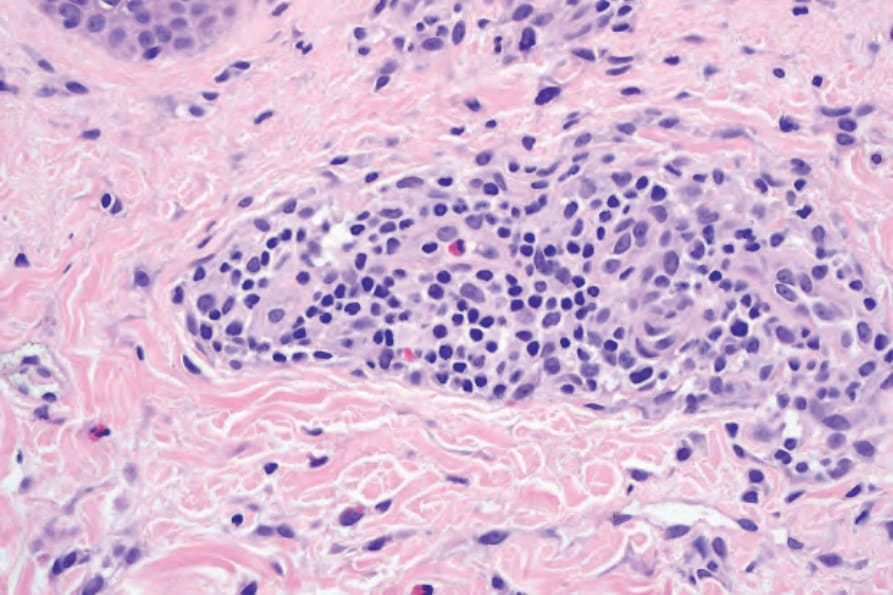
Fig. 14.8 Urticarial drug reaction: high-power view showing a predominately perivascular lymphohistiocytic infiltrate with one or two eosinophils.