臨床特徵 (Clinical Features)
-
假性紫質症 (pseudoporphyria)(藥物誘發性假性紫質症 (drug-induced pseudoporphyria)、藥物誘發性假性遲發性皮膚紫質症 (drug-induced pseudoporphyria cutanea tarda)、假性遲發性皮膚紫質症 (pseudoporphyria cutanea tarda)、末期腎衰竭水疱性皮膚病 (bullous dermatosis in end-stage renal failure)、血液透析水疱性皮膚病 (bullous dermatosis of hemodialysis))係指一種呈光分布 (photodistributed) 的水疱性皮膚病,型態類似遲發性皮膚紫質症 (porphyria cutanea tarda),但缺乏任何血清、尿液或糞便的紫質 (porphyrin) 異常 (Figs 13.122–13.125)。
-
目前已知其成因眾多,包括藥物、過度的 UVA 曝露(含使用日光浴床 (sunbeds))以及日光曝曬,並可能發生於因慢性腎衰竭而接受血液透析 (hemodialysis) 的病人。
-
在接受血液透析的病人中,pseudoporphyria 的發生率高達 6%。
-
亦曾描述於以葉綠素 (chlorophyll) 自行用藥的病人。
-
小而緊張的水疱發生於手背與手指背側,偶爾侵犯臉部、上胸部及腿部。
-
常合併粟粒疹 (milia)、皮膚脆弱 (skin fragility)、光敏感 (photosensitivity) 與疤痕形成。
-
多毛症 (hypertrichosis)、色素沉著 (hyperpigmentation)、硬皮病樣變化 (sclerodermoid changes),以及如見於 porphyria cutanea tarda 的營養不良性鈣化 (dystrophic calcification),並非 pseudoporphyria 的特徵。
-
在罹患此病的兒童(通常為因幼年型關節炎 (juvenile arthritis) 服用 naproxen 者)中,曾記錄到類似紅血球生成性原紫質症 (erythropoietic protoporphyria) 的臉部疤痕。
-
一般而言,似乎不存在肝臟異常。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
-
pseudoporphyria 為一種與 UVA 相關的光毒性 (phototoxic) 皮膚病。
-
它可能在血液透析 (hemodialysis) 與腹膜透析 (peritoneal dialysis) 之後發生,也可能在未接受透析的慢性腎衰竭病人中發生。
-
在此類病人中,建議的危險因子包括鐵負荷過量 (iron overload)、鋁中毒 (aluminum intoxication)、PVC 誘發的光敏感、藥物及乙醇 (ethanol)。
-
此病亦曾記錄於使用非類固醇抗發炎藥物 (nonsteroidal anti-inflammatory medications) 後,包括 naproxen 與環氧合酶抑制劑 (cyclooxygenase inhibitors)。
-
多種其他藥物亦曾被指為禍首,包括各種抗生素(例如 nalidixic acid、tetracyclines 與 ciprofloxacin)、抗黴菌劑(例如 voriconazole)、利尿劑(例如 furosemide (frusemide)、torsemide)、metformin、finasteride、酪胺酸激酶抑制劑 (tyrosine kinase inhibitors)、ciclosporin 及口服避孕藥 (oral contraceptives)。
-
使用 UVA 助曬床 (suntanning beds) 亦是公認的 pseudoporphyria 成因。
-
受影響者幾乎全為年輕女性,PUVA 療法亦曾少數被指為誘因。
-
曾報告一例罕見的窄波 UVB (narrow-band UVB) 誘發之 pseudoporphyria,發生於接受乾癬 (psoriasis) 治療的病人。
-
水疱位於表皮下 (subepidermal) 且相當平淡 (bland),內含或許少量的纖維蛋白 (fibrin),偶有紅血球 (Fig. 13.126)。
-
水疱底部典型地由保存良好的真皮乳頭 (dermal papillae) 襯覆(呈花彩狀 festooning)。
-
通常無明顯的發炎成分,但偶爾在淺層真皮可見輕度的血管周圍淋巴球浸潤。
-
淺層血管可能出現增厚(以 PAS 染色可凸顯),並可能呈現伴有彈性纖維增生 (elastosis) 的真皮硬化 (dermal sclerosis)。
-
直接免疫螢光 (Direct immunofluorescence) 顯示淺層血管周圍有免疫球蛋白 (Ig,通常為 IgG、IgM,有時為 IgA) 與 C3,呈甜甜圈狀分布 (donut distribution),並在表皮基底膜區 (epidermal basement membrane region) 呈細顆粒狀沉積 (Fig. 13.127)。
-
間接免疫螢光 (Indirect immunofluorescence) 一律為陰性。
-
在電子顯微鏡檢查下,分裂平面 (plane of cleavage) 不一:在某些病例顯示位於透明板 (lamina lucida) 內,而在另一些則位於緻密板 (lamina densa) 深部 (Fig. 13.128)。
-
如同 porphyria cutanea tarda,基底膜重複增生 (basement membrane reduplication) 典型地同時出現於真皮–表皮交界 (dermal–epidermal junction) 及淺層血管周圍 (Fig. 13.129)。
鑑別診斷 (Differential Diagnosis)
- 一律為陰性的間接免疫螢光 (indirect immunofluorescence) 與缺乏紫質 (porphyrin) 異常,可將此病與自體免疫水疱性皮膚病 (autoimmune bullous dermatoses) 及 porphyria cutanea tarda 區別。
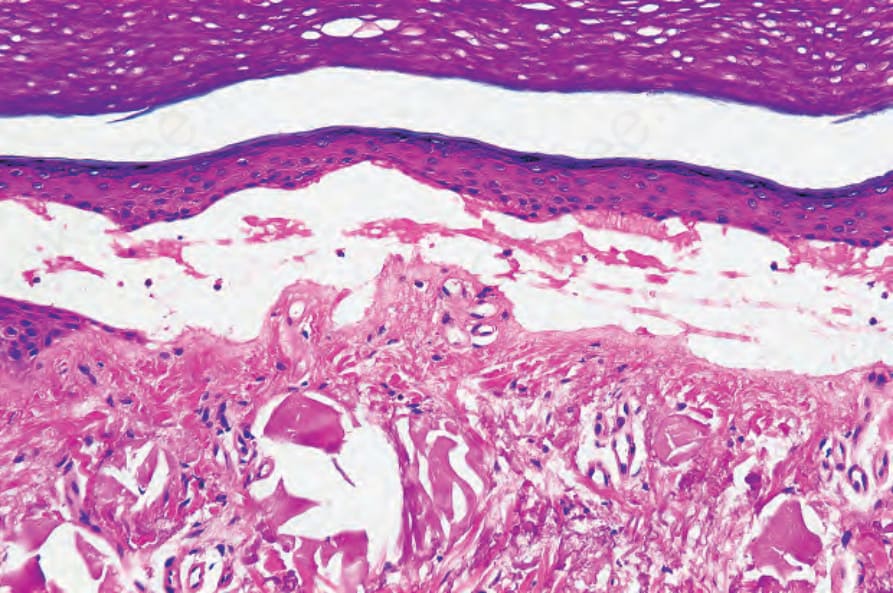
圖 13.119:遲發性皮膚紫質症 (porphyria cutanea tarda):此水疱深部可見類膠樣粟粒疹樣 (colloid milium-like) 的日光性彈性纖維變性 (solar elastosis)。
Fig. 13.119 Porphyria cutanea tarda: there is colloid milium-like solar elastosis deep to this blister.
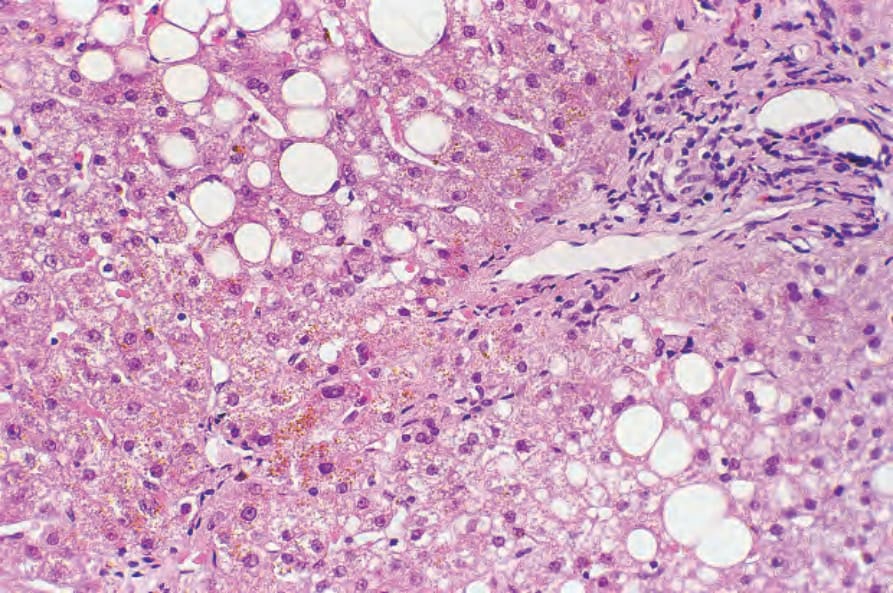
圖 13.120:遲發性皮膚紫質症 (porphyria cutanea tarda):除了脂肪變性 (fatty change) 與輕度慢性發炎外,可見明顯的棕色尿紫質 (uroporphyrin) 結晶。
Fig. 13.120 Porphyria cutanea tarda: in addition to fatty change and mild chronic inflammation, brown uroporphyrin crystals are evident.

圖 13.122:假性紫質症 (pseudoporphyria):可見廣泛的紫斑 (purpura),伴有雀斑樣斑點 (freckling) 與明顯的抓痕 (excoriations)。此病人使用日光浴床 (sunbed) 多年。承蒙 G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire 提供。
Fig. 13.122 Pseudoporphyria: there is extensive purpura with freckling and conspicuous excoriations. The patient had used a sunbed for a number of years. By courtesy of G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire.

圖 13.123:假性紫質症 (pseudoporphyria):手臂上可見小而緊張、成群的小水疱 (vesicles)。承蒙 G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire 提供。
Fig. 13.123 Pseudoporphyria: small tense grouped vesicles are present on the arm. By courtesy of G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire.

圖 13.124:假性紫質症 (pseudoporphyria):注意覆蓋於指關節 (knuckle) 上的出血性水疱 (hemorrhagic blister)。承蒙 G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire 提供。
Fig. 13.124 Pseudoporphyria: note the hemorrhagic blister overlying the knuckle. By courtesy of G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire.

圖 13.125:假性紫質症 (pseudoporphyria):可見多處糜爛 (erosions) 與粟粒疹 (milia)。承蒙 the Institute of Dermatology, London, UK 提供。
Fig. 13.125 Pseudoporphyria: there are multiple erosions and milia. By courtesy of the Institute of Dermatology, London, UK.
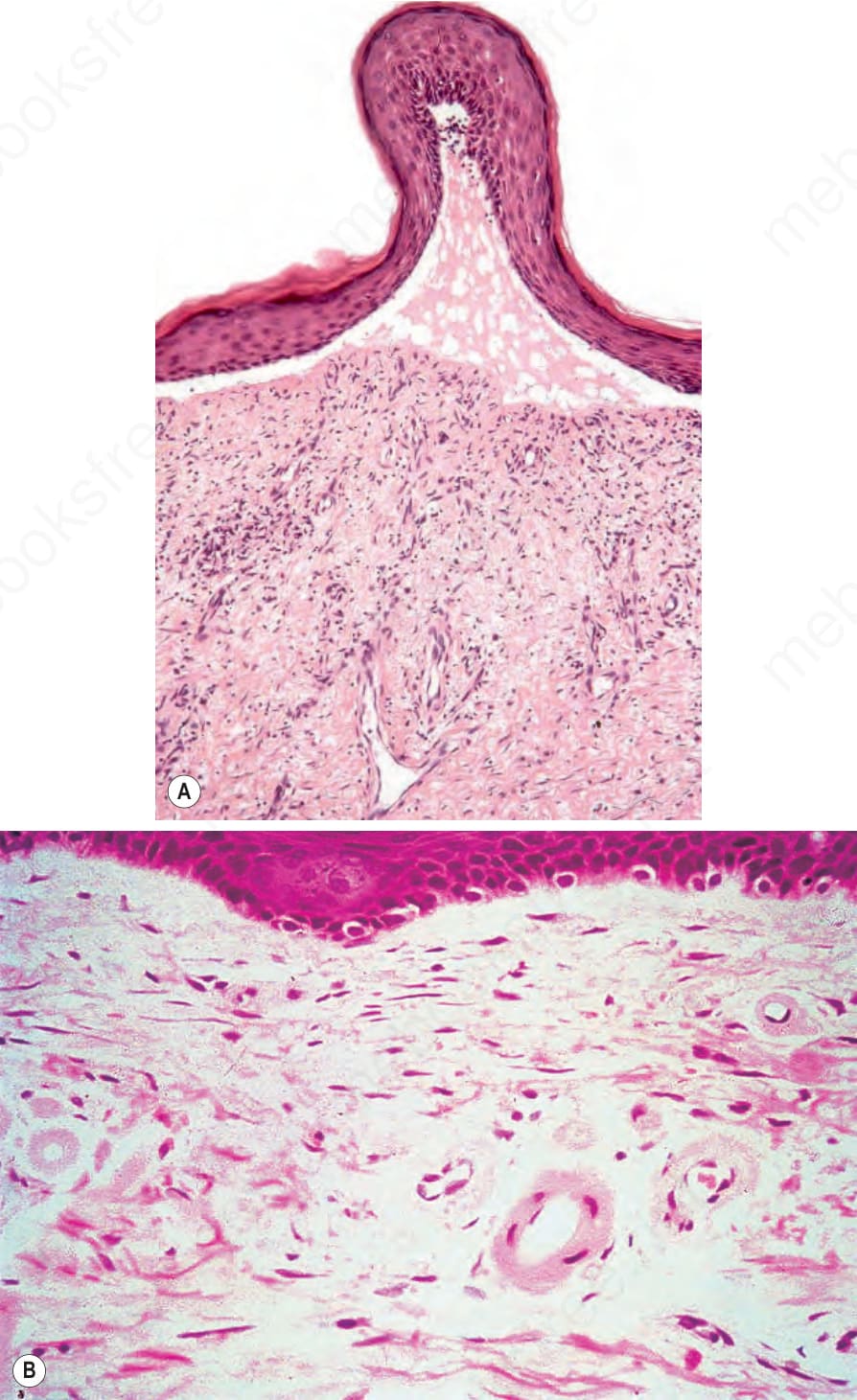
圖 13.126:假性紫質症 (pseudoporphyria):(A) 可見一表皮下水疱 (subepidermal blister);(B) 淺層真皮血管增厚並帶有玻璃樣沉積 (hyaline deposit)。(B) 承蒙 G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire 提供。
Fig. 13.126 Pseudoporphyria: (A) there is a subepidermal blister; (B) the superficial dermal vessels are thickened with a hyaline deposit. (B) By courtesy of G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire.
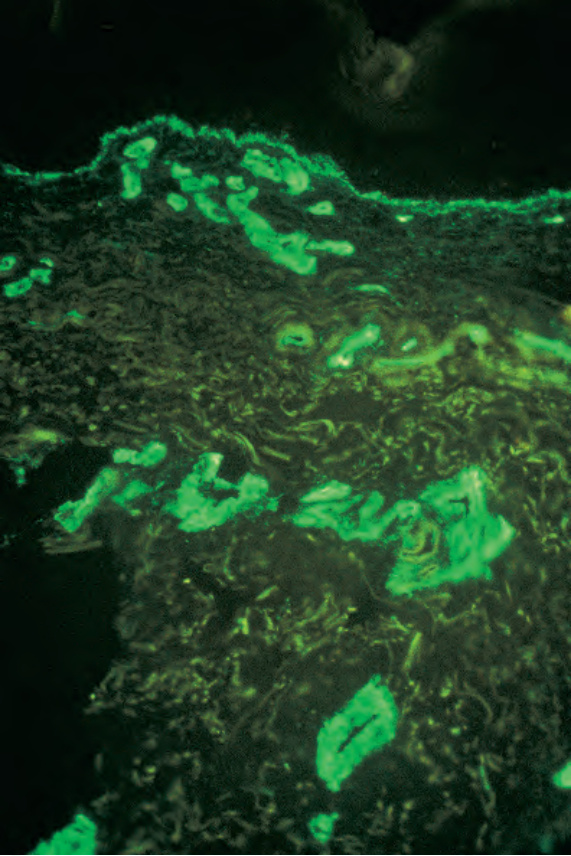
圖 13.127:假性紫質症 (pseudoporphyria):如此視野所示,血管壁增厚部分肇因於過量的第四型膠原蛋白 (type IV collagen)。承蒙 G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire 提供。
Fig. 13.127 Pseudoporphyria: the vessel wall thickening is in part due to excess type IV collagen, as shown in this field. By courtesy of G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire.
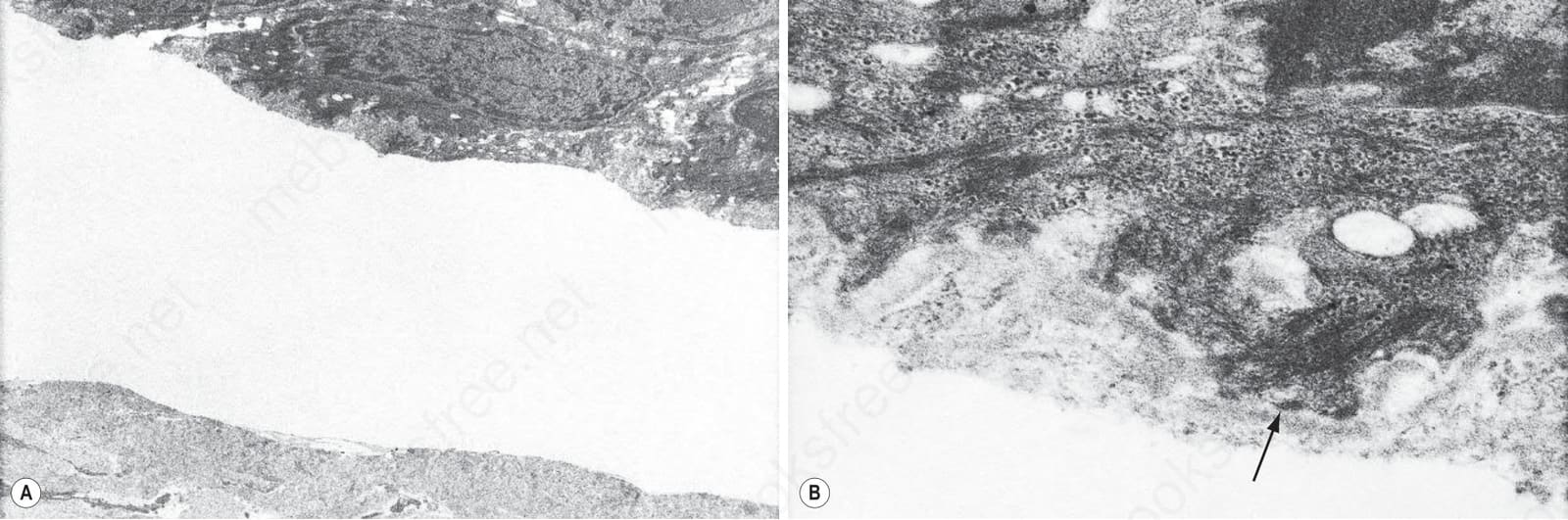
圖 13.128:(A, B) 假性紫質症 (pseudoporphyria):在此例中,水疱位於淺層乳頭真皮 (superficial papillary dermis)、緻密板 (lamina densa)(箭頭所示)深部。
Fig. 13.128 (A, B) Pseudoporphyria: in this example, the blister is located in the superficial papillary dermis deep to the lamina densa (arrowed).
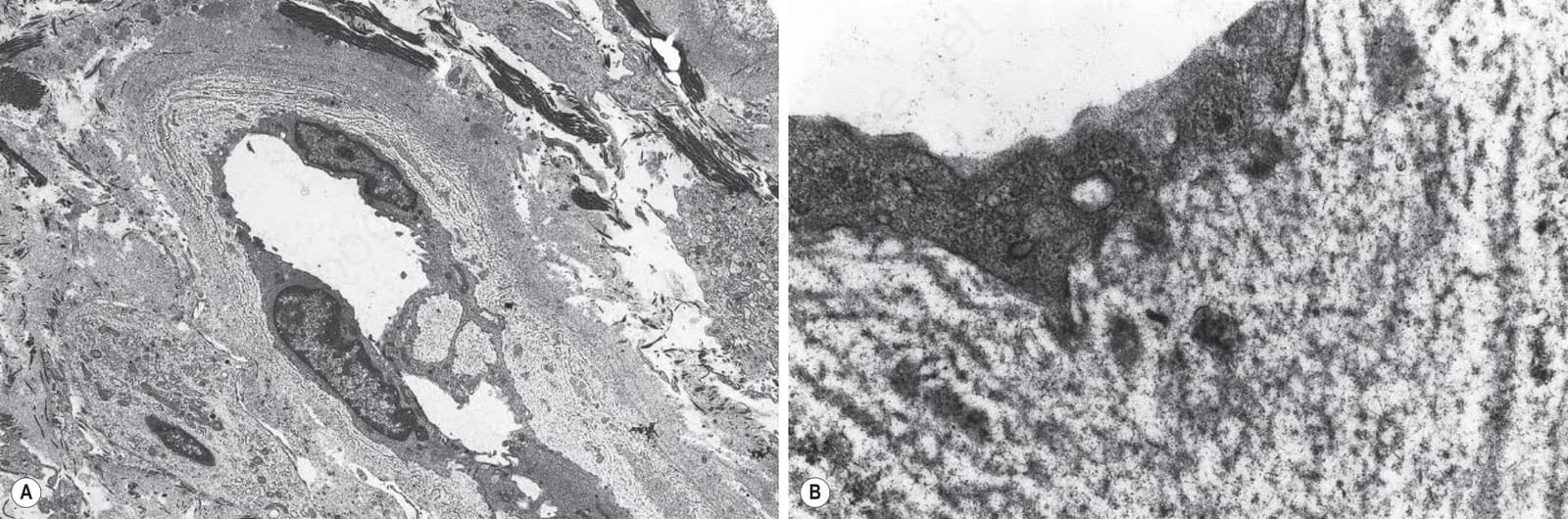
圖 13.129:(A, B) 假性紫質症 (pseudoporphyria):注意顯著的基底膜重複增生 (basement membrane duplication)。
Fig. 13.129 (A, B) Pseudoporphyria: note the striking basement membrane duplication.

圖 13.130:痛風 (gout):手背側面 (dorsal aspect) 的大量沉積物。
Fig. 13.130 Gout: massive deposit on the dorsal aspect of the hand.