Pseudoporphyria
Pseudoporphyria
Clinical features Pseudoporphyria (drug-induced pseudoporphyria, drug-induced pseudoporphyria cutanea tarda, pseudoporphyria cutanea tarda, bullous dermatosis in end-stage renal failure, bullous dermatosis of hemodialysis) refers to a photodistributed blistering dermatosis resembling porphyria cutanea tarda but in the absence of any serum, urine, or stool porphyrin abnormality (Figs 13.122–13.125).1 It is now recognized as having many causes including drugs, excessive UVA (including the use of sunbeds), and sunlight exposure and may develop in patients undergoing hemodialysis for chronic renal failure.1–24 Pseudoporphyria occurs in up to 6% of patients receiving hemodialysis.25 It has also been described in patients self-medicating with chlorophyll.26
Small tense blisters develop on the backs of the hands and fingers, and occasionally involve the face, upper chest, and legs.1,2 Milia, skin fragility, photosensitivity, and scarring are often present. Hypertrichosis, hyperpigmentation, sclerodermoid changes, and dystrophic calcification as seen in porphyria cutanea tarda are not features of pseudoporphyria.1 In children affected with this condition (usually receiving naproxen for juvenile arthritis), facial scarring reminiscent of erythropoietic protoporphyria has been documented.7,27 In general, hepatic abnormalities appear to be absent.1
Pathogenesis and histologic features Pseudoporphyria is a UVA-related phototoxic dermatosis.1 It may develop following both hemodialysis and peritoneal dialysis and also in patients with chronic renal failure in the absence of dialysis. Suggested risk factors in such patients include iron overload, aluminum intoxication, PVC-induced photosensitivity, drugs, and ethanol.1,2 The condition has also been documented following use of nonsteroidal anti-inflammatory medications, including naproxen and cyclooxygenase inhibitors.7–10,19 A wide variety of other drugs, including various antibiotics (e.g., nalidixic acid, tetracyclines, and ciprofloxacin), antifungals (e.g., voriconazole), diuretics (e.g., furosemide
600 Degenerative and metabolic diseases
(frusemide), torsemide), metformin, finasteride, tyrosine kinase inhibitors, ciclosporin, and oral contraceptives have also been incriminated. 13–24,27–34 The use of UVA suntanning beds is also a well-recognized cause of pseudoporphyria.12,35 Young females are almost exclusively affected and PUVA therapy has also rarely been incriminated.1 A rare case of narrow-band UVB-induced pseudoporphyria has been reported in a patient being treated for psoriasis. 24
The blisters are subepidermal and rather bland, containing perhaps a little fibrin and, occasionally, red blood cells (Fig. 13.126).7,11,34,36 The floor of the blister is typically lined by well-preserved dermal papillae (festooning). There is usually no significant inflammatory component although occasionally, a light perivascular lymphocytic infiltrate may be seen in the
superficial dermis. Thickening of the superficial vessels (highlighted by a PAS stain) and dermal sclerosis with elastosis may be apparent.
Direct immunofluorescence reveals Ig (usually IgG, IgM, and sometimes IgA) with C3 around the superficial vasculature in a donut distribution and as a fine granular deposit at the epidermal basement membrane region (Fig. 13.127).2,7,27,28,35–37 Indirect immunofluorescence is invariably negative.2
On electron microscopic examination, the plane of cleavage is variable: in some it has been shown to be within the lamina lucida, whereas in others it has been deep to the lamina densa (Fig. 13.128).7,38,39 As in porphyria cutanea tarda, basement membrane reduplication is typically present both at the dermal–epidermal junction and also around the superficial vasculature (Fig. 13.129).7
601 Gout
A
therapy with cytotoxic drugs. Less commonly, gout represents a primary inherited disorder of purine metabolism. A number of enzymatic defects are recognized, including hypoxanthine guanine phosphoribosyltransferase activity (X-linked recessive), abnormal phosphoribosylpyrophosphate synthetase variants (X-linked dominant) and glucose-6-phosphatase deficiency.4 These defects represent a small proportion of patients with gout. More recent genome-wide association studies have rapidly expanded the knowledge of other genetic defects responsible for the disease.7–10 Many of the implicated genes are believed to function as urate transporters in the renal tubules.8–10
B
Males are affected more often than females and presentation is usually in the fourth to sixth decades. However, the incidence in females is rising, particularly in those on diuretics and those with altered renal function.11 The prevalence of the disease is higher in black patients.12
Gout produces recurrent, acute, exceedingly painful monoarticular arthritis, classically of the great toe, but also of the large joints of the legs. Many patients present initially with acute inflammation of the first metatarsophalangeal joint (podagra).13 The affected joint is characteristically exceedingly tender, hot, and erythematous, and cellulitis may therefore enter the differential diagnosis. Precipitating factors include trauma, excessive alcohol consumption, dietary excess (particularly red meat consumption), lead exposure, hypertension, renal insufficiency, surgery, and infections.4,13–16 Alcohol and obesity are associated with increased nucleotide catabolism and decreased urate excretion.17–19 Not surprisingly, more recent studies indicate a close relationship with the metabolic syndrome, and as a consequence patients with gout also have an increased risk of diabetes, myocardial infarction, and premature death.8,20 Certain medications, including diuretics (loop and thiazide), low-dose aspirin, and ciclosporin increase the risk of gout.15,21 With chronicity, a disabling and often crippling arthritis may develop, particularly affecting the hands and feet.3 Subsequently, uric acid crystal deposition in skin and soft tissues produces gouty tophi; these nodules are seen most commonly on the external ear, but also over the elbows and on the digits (Fig. 13.130). When large, they often discharge a chalky material. Rare clinical presentations include bullous lesions, a fungating mass, and sparing of hemiplegic limbs by the tophi.22–24 Nowadays, only a minority of patients
Differential diagnosis The invariably negative indirect immunofluorescence and absence of porphyrin abnormalities distinguish this disease from autoimmune bullous dermatoses and porphyria cutanea tarda.40,41
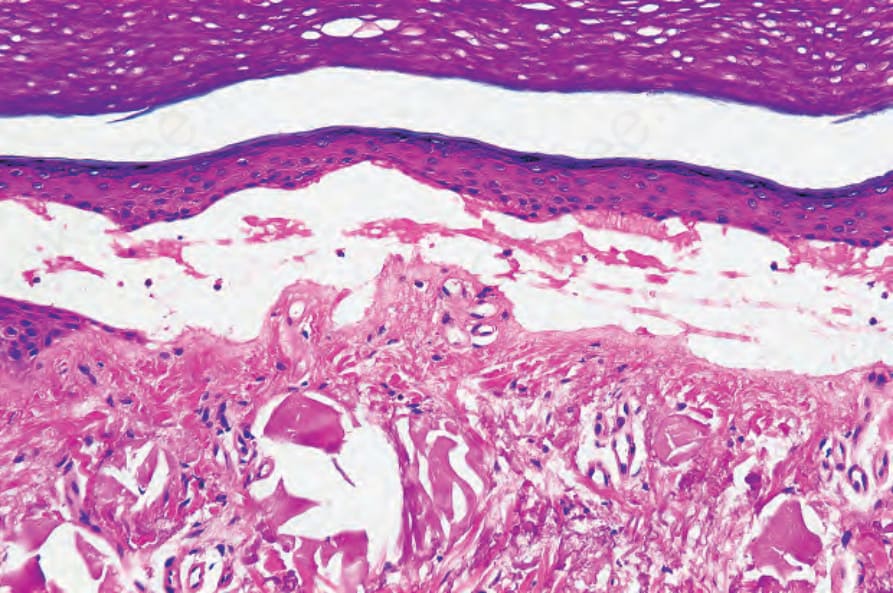
Fig. 13.119 Porphyria cutanea tarda: there is colloid milium-like solar elastosis deep to this blister.
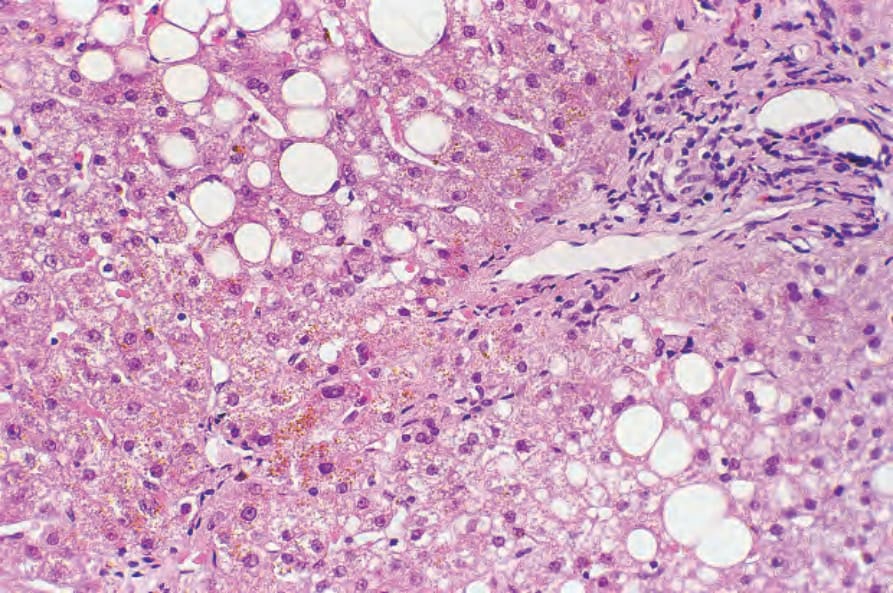
Fig. 13.120 Porphyria cutanea tarda: in addition to fatty change and mild chronic inflammation, brown uroporphyrin crystals are evident.

Fig. 13.122 Pseudoporphyria: there is extensive purpura with freckling and conspicuous excoriations. The patient had used a sunbed for a number of years. By courtesy of G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire.

Fig. 13.123 Pseudoporphyria: small tense grouped vesicles are present on the arm. By courtesy of G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire.

Fig. 13.124 Pseudoporphyria: note the hemorrhagic blister overlying the knuckle. By courtesy of G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire.

Fig. 13.125 Pseudoporphyria: there are multiple erosions and milia. By courtesy of the Institute of Dermatology, London, UK.
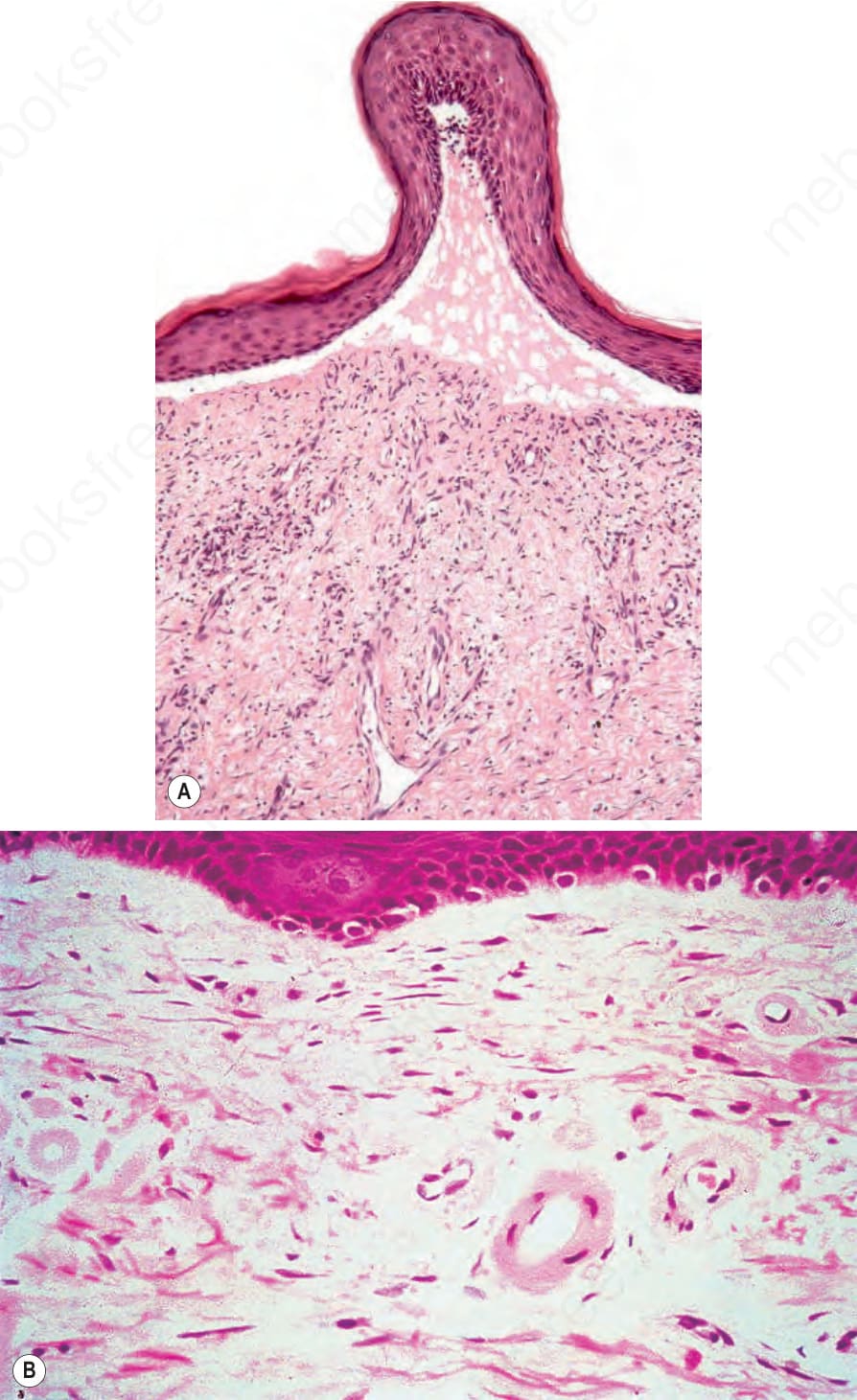
Fig. 13.126 Pseudoporphyria: (A) there is a subepidermal blister; (B) the superficial dermal vessels are thickened with a hyaline deposit. (B) By courtesy of G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire.
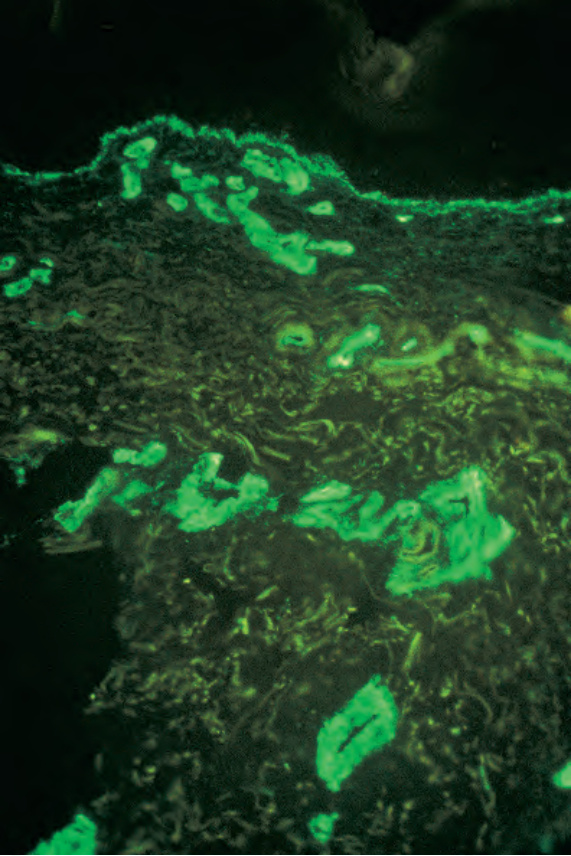
Fig. 13.127 Pseudoporphyria: the vessel wall thickening is in part due to excess type IV collagen, as shown in this field. By courtesy of G.M. Murphy, MD, Beaumont Hospital, Dublin, Eire.
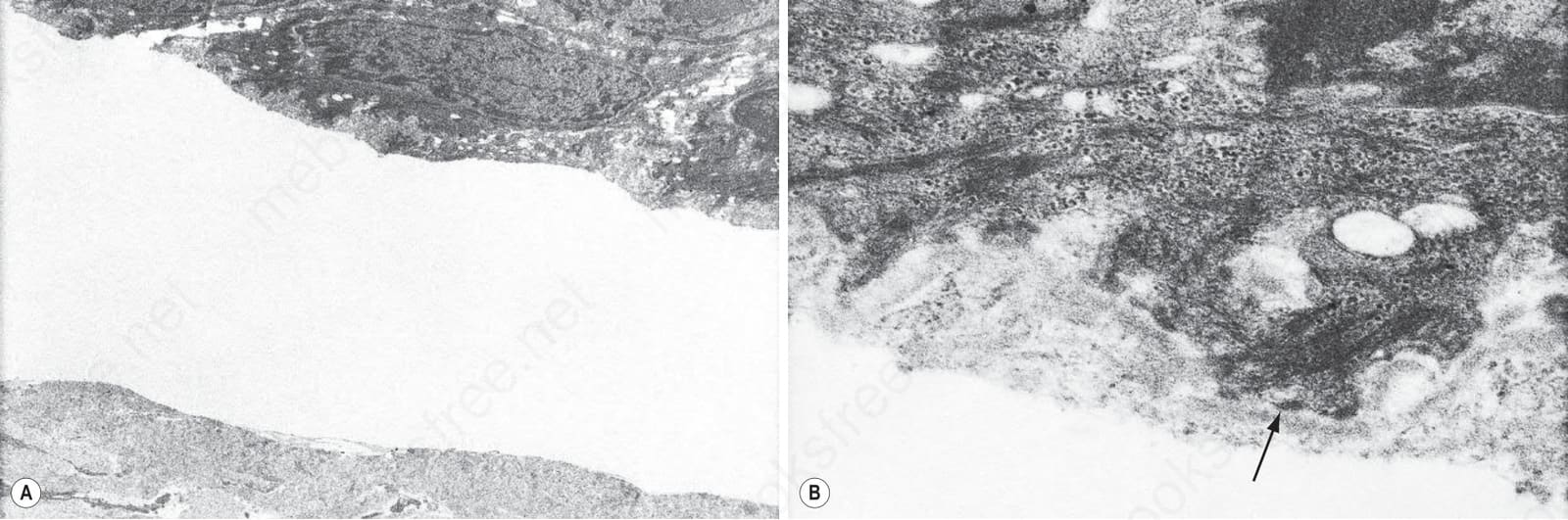
Fig. 13.128 (A, B) Pseudoporphyria: in this example, the blister is located in the superficial papillary dermis deep to the lamina densa (arrowed).
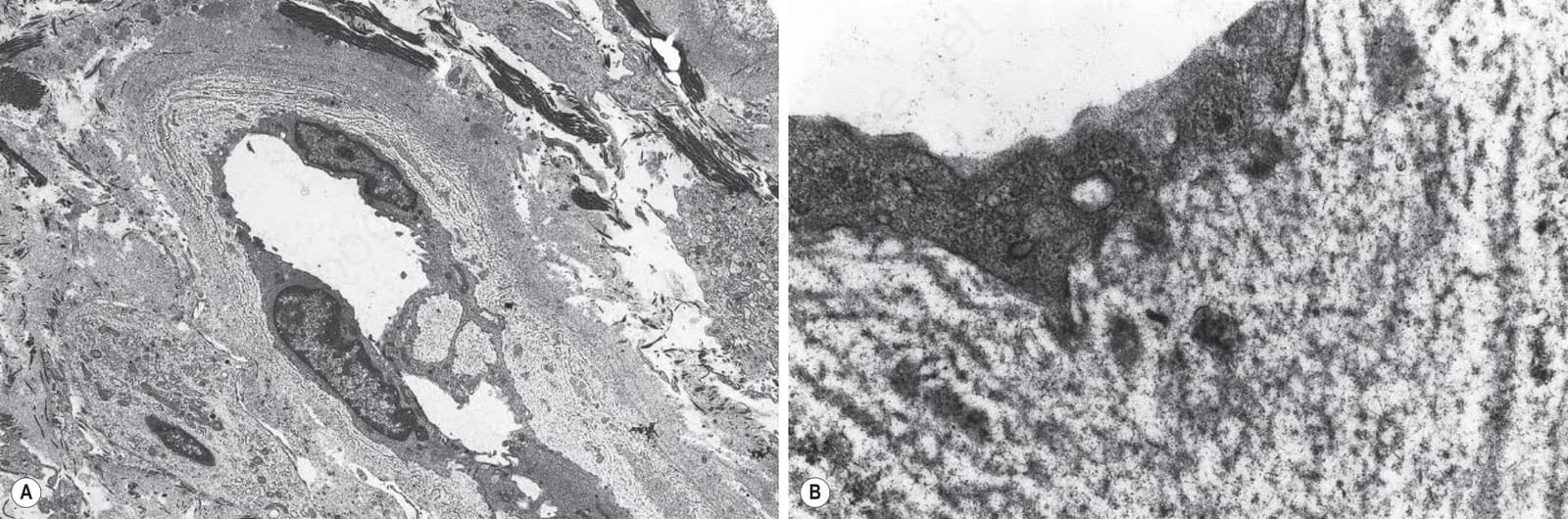
Fig. 13.129 (A, B) Pseudoporphyria: note the striking basement membrane duplication.

Fig. 13.130 Gout: massive deposit on the dorsal aspect of the hand.