疣狀黃瘤 (Verruciform Xanthoma)
臨床特徵 (Clinical Features)
- 疣狀黃瘤 (verruciform xanthoma) 是一種不常見、無症狀的病灶,主要發生於成人的口腔,好發於第五或第六十年(fifth or sixth decade),且有男性偏好 (male predilection)(1.7 : 1)。
- 它最常見於下頜骨 (mandible) 或上頜骨 (maxilla) 的前磨牙區牙齦 (premolar gingiva)。在此部位通常產生單一、邊界清楚、無症狀的紅斑性或黃褐色 (yellow–tan) 病灶,直徑 3–20 mm,可能呈乳頭瘤狀 (papillomatous) 或潰瘍。患者血脂正常 (normolipidemic)。臨床鑑別診斷包括病毒疣 (viral warts)、白斑症 (leukoplakia) 與鱗狀細胞癌 (squamous cell carcinoma)。
- 皮膚的疣狀黃瘤極為罕見,曾於多種部位被描述,包括耳、鼻、唇、指(趾)及手臂。然而,多數已描述的病例發生於肛門生殖器 (anogenital) 皮膚 (Fig. 13.24)。它也可能在表皮鬆解性棘皮瘤 (epidermolytic acanthoma)、脂漏性角化症 (seborrheic keratoses)、表皮母斑 (epidermal nevi)(包括患有發炎性線狀疣狀表皮母斑(inflammatory linear verrucous epidermal nevus)或表皮母斑症候群(epidermal nevus syndrome)的患者)、局限性淋巴管瘤 (lymphangioma circumscriptum) 內以反應性現象 (reactive phenomenon) 發展,並曾被記載為淋巴水腫 (lymphedema) 的併發症。
- 它曾被描述與長期的盤狀紅斑性狼瘡 (discoid lupus erythematosus)、硬化性苔癬 (lichen sclerosus)、扁平苔癬 (lichen planus)、表皮鬆解性水疱症 (epidermolysis bullosa) 併發潰瘍、先天性半身發育不良伴魚鱗癬樣紅皮症與肢體缺陷症候群 (congenital hemidysplasia with ichthyosiform erythroderma and limb defects syndrome, CHILD syndrome) 相關聯,並與陰莖鱗狀細胞癌 (squamous cell carcinoma of the penis) 相關聯。
- 偶爾,疣狀黃瘤呈多病灶 (multifocal)。曾有此類病例被描述為一名患有全身性脂質儲積病 (systemic lipid storage disease) 的兒童其上呼吸消化道 (upper aerodigestive tract) 的多發性病灶。多發性疣狀黃瘤也曾報導於會陰部壞死性筋膜炎 (necrotizing fasciitis of the perineum) 數年後的肛門生殖器區域,以及一名慢性移植物對抗宿主病 (chronic graft-versus-host disease) 患者的口腔黏膜。曾有一罕見的播散性病灶 (disseminated lesions) 病例被描述於手、足及肛門生殖器區域,另有一例具相似的廣泛性疾病且亦侵犯口腔。
- 在皮膚上,疣狀黃瘤通常表現為灰色或粉紅色結節,或表現為表面程度不一呈疣狀 (warty) 的斑塊。若未治療,病灶持續時間長且呈良性病程,局部切除後極少復發。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- 疣狀黃瘤的病因 (etiology) 與致病機轉 (pathogenesis) 不明。最初曾懷疑為人類乳突瘤病毒 (human papillomavirus, HPV) 的病毒感染。雖然多數研究未能證實支持此假說的確切證據,但有零星報告以聚合酶連鎖反應 (polymerase chain reaction, PCR) 在病灶中證實 HPV DNA。此外,有人提出角質形成細胞壞死 (keratinocyte necrosis) 可能導致細胞內脂質釋放,隨之引起巨噬細胞 (macrophage) 浸潤與黃瘤化 (xanthomatization)。導致角質形成細胞壞死的誘發事件尚未被確認。免疫組化與電子顯微鏡研究為後者此一假說提供了一些佐證(見下文)。較近期則有人提出,局部淋巴水腫 (localized lymphedema) 在某些病例中是關鍵因素,因為在其他與慢性淋巴水腫相關的疾病中也可見到相同類型的脂質充填巨噬細胞 (lipid-laden macrophages)。
- 疣狀黃瘤是一種外生性 (exophytic) 病灶,特徵為大量但規則的棘層肥厚 (acanthosis)、程度不一的乳頭瘤病 (papillomatosis)、角化不全 (parakeratosis) 與角化過度 (hyperkeratosis) (Fig. 13.25)。常於角質層 (stratum corneum) 處觀察到嗜中性球 (neutrophils) 與嗜中性球碎屑。角化不全的角質層內也可能明顯可見細菌菌落 (bacterial colonies)。棘層肥厚伴有均勻、球狀的表皮突 (epidermal ridges),且全部延伸至相同深度,形成具特徵性的平整下緣 (level lower border)。擴大的表皮突伴有明顯的中央角質形成細胞壞死,以及濃密的嗜中性多形核 (neutrophil polymorph) 發炎細胞浸潤 (Fig. 13.26)。無上皮非典型性 (epithelial atypia),且病毒包涵體 (viral inclusions) 一律缺如。延長的表皮突之間突顯的真皮乳頭 (papillary dermis) 內含有
鑑別診斷 (Differential Diagnosis)
疣狀黃瘤必須與病毒疣 (viral warts)、顆粒細胞瘤 (granular cell tumor) 及疣狀癌 (verrucous carcinoma) 區分:
- 病毒疣 (Viral warts):疣狀黃瘤缺乏病毒疣中所見的空泡化 (vacuolation)、團塊狀角質透明顆粒 (clumped keratohyalin granules) 及層狀的角化不全 (tiers of parakeratosis)。包涵體 (inclusions) 不是其特徵。
- 在顆粒細胞瘤 (granular cell tumor) 中,其上方增生的鱗狀上皮常呈浸潤性生長型態 (infiltrative growth pattern),與疣狀黃瘤的外生性 (exophytic) 性質形成對比。顆粒細胞較大,常具合胞體外觀 (syncytial appearance),且典型地呈 PAS 反應陽性。
- 疣狀癌 (Verrucous carcinoma) 兼具外生性 (exophytic) 與內生性 (endophytic) 成分,後者表現為深入穿透的球狀上皮突起 (bulbous epithelial processes)。其上皮常呈「水樣 (watery)」外觀,且黃瘤細胞 (xanthoma cells) 不是其特徵。
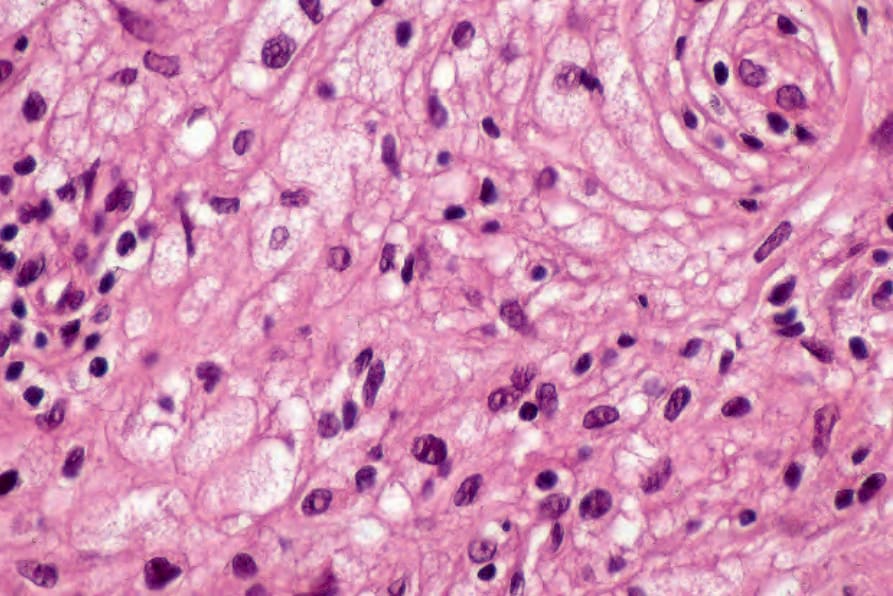
圖 13-23:平面黃瘤 (planar xanthoma):除黃瘤細胞 (xanthoma cells) 外,尚有散在的淋巴球 (lymphocytes)。
Fig. 13.23 Planar xanthoma: in addition to xanthoma cells, there are scattered lymphocytes.

圖 13-24:疣狀黃瘤 (verruciform xanthoma):在此不尋常的大體 (gross) 範例中,有眾多疣狀與息肉狀 (polypoid) 病灶,廣泛侵犯外陰 (vulva)、會陰 (perineum) 與大腿。臨床上最初曾懷疑為病毒病因 (viral etiology)。
Fig. 13.24 Verruciform xanthoma: in this unusual gross example, there are numerous warty and polypoid lesions showing extensive involvement of the vulva, perineum, and thighs. A viral etiology was initially suspected clinically.
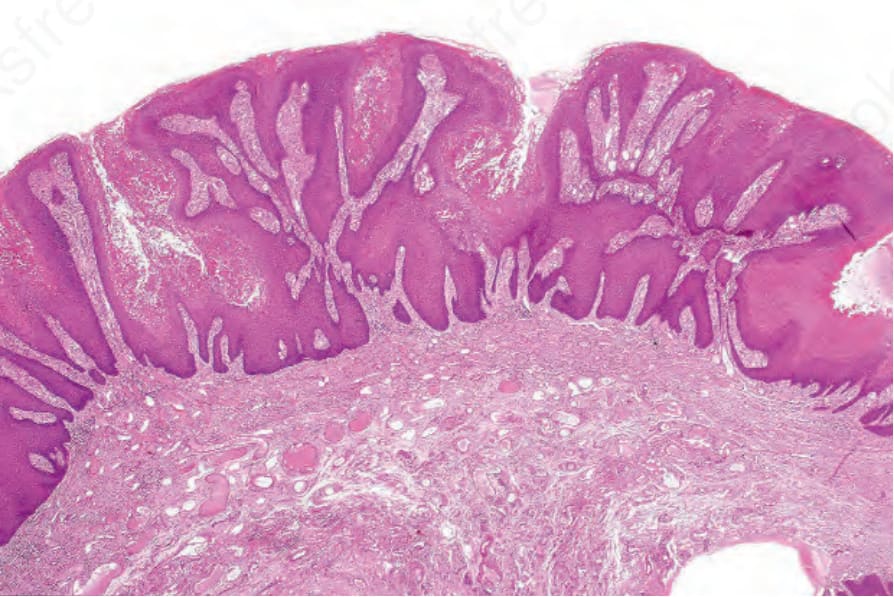
圖 13-25:疣狀黃瘤 (verruciform xanthoma):有明顯的棘層肥厚 (acanthosis)、角化過度 (hyperkeratosis) 與平整的下緣 (level lower border)。
Fig. 13.25 Verruciform xanthoma: there is marked acanthosis, hyperkeratosis, and a level lower border.
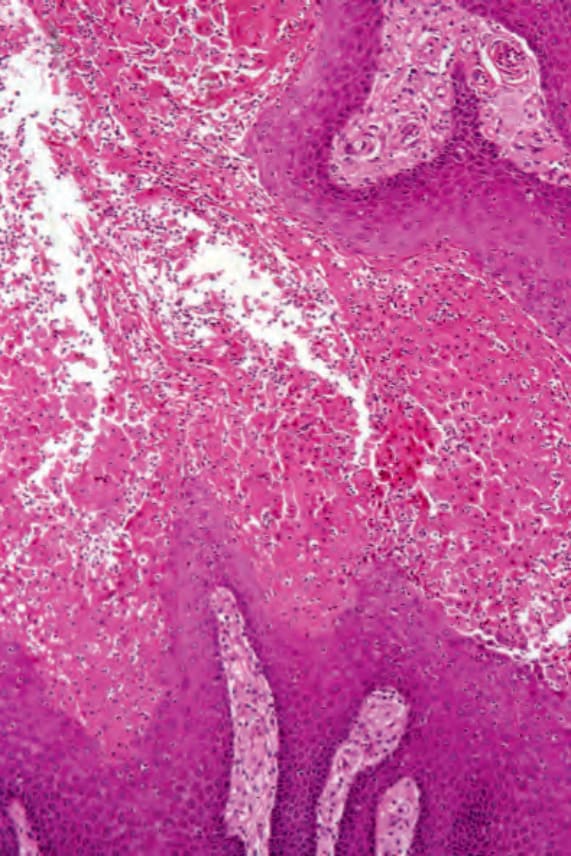
圖 13-26:疣狀黃瘤 (verruciform xanthoma):有廣泛的角質形成細胞壞死 (keratinocyte necrosis),伴隨多形核 (polymorph) 浸潤。
Fig. 13.26 Verruciform xanthoma: there is extensive keratinocyte necrosis associated with a polymorph infiltrate.