Verruciform xanthoma
Verruciform xanthoma
Clinical features The verruciform xanthoma is an uncommon, asymptomatic lesion, which occurs predominantly in the oral cavity of adults in their fifth or sixth decade
568 Degenerative and metabolic diseases
and shows a male predilection (1.7 : 1).1–5 It is most often found on the premolar gingiva of the mandible or maxilla.1 At this site it usually produces a solitary, well-circumscribed, asymptomatic, erythematous or yellow–tan lesion, 3–20 mm in diameter, which may be papillomatous or ulcerated. The patients are normolipidemic. The clinical differential diagnosis includes viral warts, leukoplakia, and squamous cell carcinoma.
Verruciform xanthomata of the skin, which are extremely rare, have been described at a variety of sites including the ear, nose, lip, digits, and arm.6–13 Most cases described, however, have arisen on anogenital skin (Fig. 13.24).14–22 It may also develop as a reactive phenomenon within epidermolytic acanthoma, seborrheic keratoses, epidermal nevi (including patients with inflammatory linear verrucous epidermal nevus or with the epidermal nevus syndrome), lymphangioma circumscriptum, and has been recorded as a complication of lymphedema.9,23–32 It has been described in association with longstanding discoid lupus erythematosus, lichen sclerosus, lichen planus, complicating ulceration in epidermolysis bullosa, congenital hemidysplasia with ichthyosiform erythroderma and limb defects syndrome (CHILD syndrome) and in association with squamous cell carcinoma of the penis.33–43 Occasionally, verruciform xanthomata are multifocal.6 Such a case has been described as multiple lesions in the upper aerodigestive tract of a child with a systemic lipid storage disease.38 Multiple verruciform xanthomata have also been reported in the anogenital region several years following necrotizing fasciitis of the perineum and in the oral mucosa in a patient with chronic graft-versus-host disease.39,44 A rare case of disseminated lesions has been described on the hands, feet, and anogenital region and another with similar widespread disease that also included the oral cavity.45,46
In the skin, verruciform xanthoma usually presents as a gray or pink nodule or as a plaque with a variably warty surface. Untreated, the lesions have a long duration and behave in a benign fashion, recurrence being very uncommon after local excision.
Pathogenesis and histologic features The etiology and pathogenesis of the verruciform xanthoma are unknown. Originally, a viral infection by human papillomavirus (HPV) was suspected. Although most studies have not demonstrated definitive evidence to support this hypothesis, there are isolated reports demonstrating HPV DNA by polymerase chain reaction (PCR) in the lesions.47–50 Additionally, it has been suggested that keratinocyte necrosis may lead to the release of intracellular lipids, with resultant macrophage influx and xanthomatization.3,49,51 The inciting event leading to keratinocyte necrosis has not been identified. Immunohistochemical and electron microscopic studies give some credence to support to this latter hypothesis (see below). More recently, it has been proposed that localized lymphedema is a critical factor in some cases, as the
same types of lipid-laden macrophages are seen in other conditions associated with chronic lymphedema.31,32
Verruciform xanthoma is an exophytic lesion characterized by massive but regular acanthosis, variable papillomatosis, parakeratosis, and hyperkeratosis (Fig. 13.25).47 Neutrophils, and neutrophilic debris are frequently observed at the level of the stratum corneum. Bacterial colonies may also be evident in the parakeratotic stratum corneum. The acanthosis is associated with uniform, bulbous epidermal ridges, all of which penetrate to the same depth, giving a characteristically level lower border. The expanded ridges are associated with marked central keratinocyte necrosis and a heavy neutrophil polymorph inflammatory cell infiltrate (Fig. 13.26). There is no epithelial atypia and viral inclusions are invariably absent. The accentuated papillary dermis between the elongated epidermal ridges contains
569 Angiokeratoma corporis diffusum
Differential diagnosis Verruciform xanthoma must be distinguished from viral warts, granular cell tumor, and verrucous carcinoma:
• Viral warts: verruciform xanthoma lacks the vacuolation, clumped keratohyalin granules and tiers of parakeratosis seen in a viral wart. Inclusions are not a feature.
• In granular cell tumor the hyperplastic overlying squamous epithelium often shows an infiltrative growth pattern, in contrast to the exophytic nature of verruciform xanthoma. The granular cells are larger, often have a syncytial appearance, and typically stain positively with the PAS reaction.
• Verrucous carcinoma has both exophytic and endophytic components, the latter appearing as deeply penetrating bulbous epithelial processes. The epithelium often has a ‘watery’ appearance and xanthoma cells are not a feature.
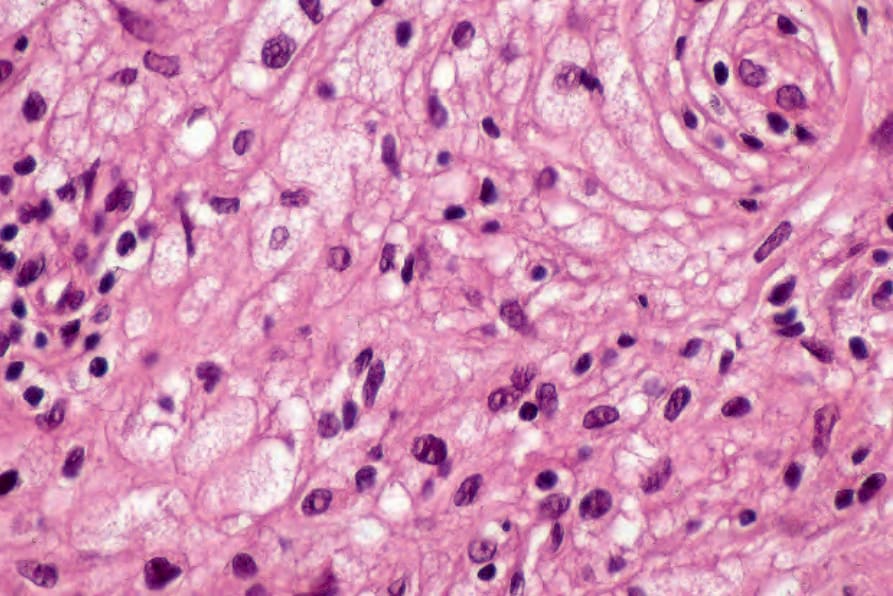
Fig. 13.23 Planar xanthoma: in addition to xanthoma cells, there are scattered lymphocytes.

Fig. 13.24 Verruciform xanthoma: in this unusual gross example, there are numerous warty and polypoid lesions showing extensive involvement of the vulva, perineum, and thighs. A viral etiology was initially suspected clinically.
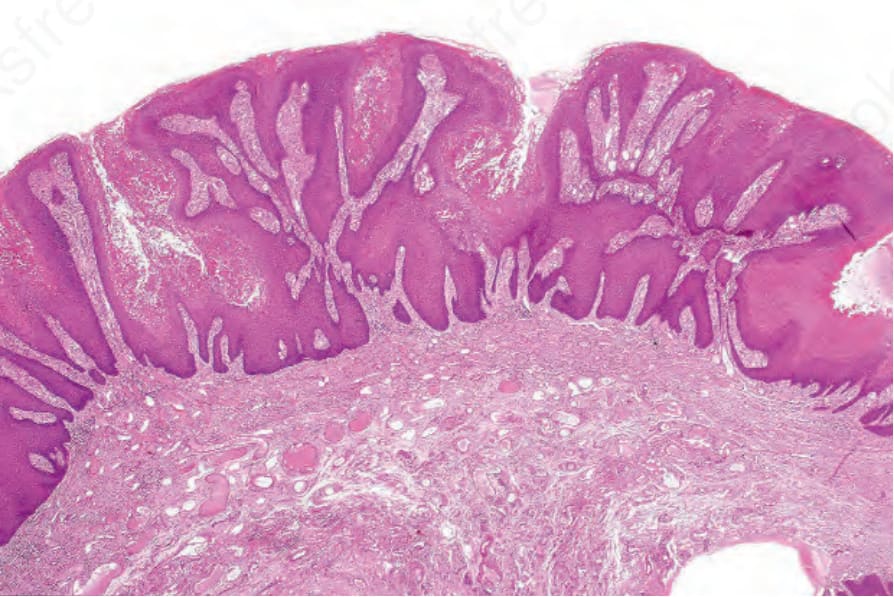
Fig. 13.25 Verruciform xanthoma: there is marked acanthosis, hyperkeratosis, and a level lower border.
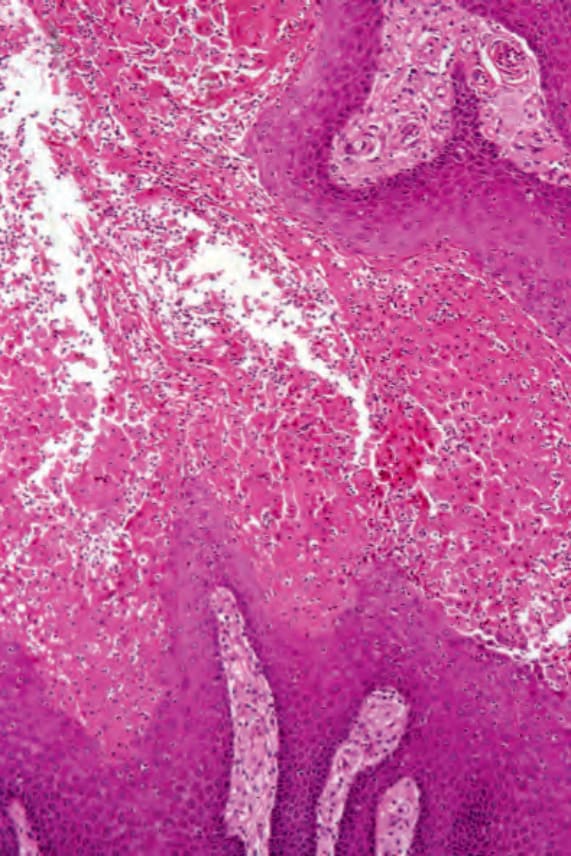
Fig. 13.26 Verruciform xanthoma: there is extensive keratinocyte necrosis associated with a polymorph infiltrate.