臨床特徵 (Clinical Features)
梅毒 (syphilis) 的發生率在 1940 年代 penicillin 問世之後急遽下降。近年來其發生率逐年上升,主要是由於 HIV 感染病例數增加所致。藥物濫用與高風險性行為也是促成因素。梅毒發生率的上升持續進行中,尤其是在 HIV 感染病人,且好發於年輕的男同性戀黑人男性。
在十六世紀,梅毒帶有高死亡率,伴隨一種慢性、毀容且使人失能的疾病。目前此疾病表現得較不具侵襲性,即使在未治療的病例亦然。它具有高度傳染性,自受感染伴侶傳染的風險估計高達 60%。罹患此疾病的機率取決於暴露次數、性行為類型,以及伴侶病灶的位置與數量。梅毒與 HIV 感染之間有密切關係,兩種疾病可同時被感染。已知像梅毒這類會引起生殖器潰瘍的疾病,會增加感染 HIV 的風險。
致病菌為 Treponema pallidum,一種對生長條件要求苛刻 (fastidious) 的螺旋體 (spirochete)。傳播主要透過性行為。一種稱為 bejel 的地方流行型 (endemic form),由相同的病原菌所引起,發生於生活在衛生條件不良環境中的兒童,並透過皮膚接種 (cutaneous inoculation) 傳播。其他地方流行型則與共用飲水器具有關,當社區中某些成員患有口腔或唇部梅毒病灶時即可能發生。
典型的初始病灶——硬性下疳 (chancre)——於暴露於病原菌後 20–30 天,在接種部位發展出來。此部位可位於肛門生殖器皮膚的任何位置,較常見於陰莖龜頭 (glans penis)(尤其是冠狀溝 coronal sulcus)、陰莖體 (shaft)、或包皮 (prepuce),或位於大陰唇 (labia majora) 或小陰唇 (labia minora)(圖 12.95–12.99)。至少有 5% 的初期硬性下疳發生於生殖器外的部位,最常見為口腔,但實際上皮膚表面幾乎任何其他部位都可能受侵犯,包括扁桃腺 (tonsils)、手指、眼瞼與乳頭(圖 12.100 與 12.101)。陰道或子宮頸的病灶可能未被察覺。硬性下疳表現為一個質地堅硬 (indurated)、穿鑿狀 (punched-out)、無痛的潰瘍。通常伴隨無痛性淋巴腺病 (painless lymphadenopathy)。此病灶於 1–5 週後消退而不留疤痕。
繼發性的皮膚病灶(syphilids,梅毒疹)具有高度傳染性,可模擬幾乎任何皮膚疾病。它們在硬性下疳出現後 6–8 週呈現。它們以隱匿方式發展(在高達 80% 的病人),出現玫瑰色、斑狀–紅斑樣 (roseolar, macular–erythematous) 的皮疹,分布於頭部、面部與頸部,隨後出現多形性丘疹性 (polymorphic papular) 疹。斑疹直徑為 5–10 mm,不會搔癢,特別好發於軀幹、腹部與四肢,尤其是手掌與足底(圖 12.102–12.107)。丘疹性病灶特徵為銅紅色 (coppery red),直徑 3–10 mm。頸部的色素減退稱為「維納斯項圈」(‘collar of venus’)。
其他描述過的表現包括:扁平濕疣 (condylomata)(位於間擦部位 intertriginous areas)、環狀 (annular)、苔癬樣 (lichenoid)、丘疹鱗屑性 (papulosquamous) 病灶(psoriasiform,乾癬樣)、弧形 (arcuate) 病灶、繖房狀 (corymbose) 棕紅色丘疹(希臘文 korymbos,意為一簇常春藤花)、大皰性 (bullous)、多形性紅斑樣 (erythema multiforme-like) 的毛囊性 (follicular) 與膿皰性 (pustular) 皮膚變異型,伴有侵蝕性潰瘍(黏膜斑 mucous patches),常為「蝸牛軌跡」(‘snail track’) 型,以及(具高度傳染性的)侵犯黏膜的扁平濕疣 (condylomata lata)(圖 12.108–12.111)。亦可見角皮症 (keratoderma)。大型肥厚性扁平濕疣稱為莓狀梅毒疹 (framboiseform syphilids)。其他描述過的變異型為痤瘡樣 (acneiform)、痘瘡樣 (varioliform),以及罕見的壞死性 (necrotic)(圖 12.112)。病灶傾向廣泛播散,且分布常呈對稱性。頭皮的丘疹性侵犯可導致非疤痕性、斑塊狀的脫髮 (alopecia)(圖 12.113)。由繼發性梅毒所引起的脫髮稱為梅毒性脫髮 (alopecia syphilitica),具有特徵性的「蟲蛀樣」(moth-eaten) 外觀。鬍鬚、眉毛與睫毛亦可能受侵犯。亦曾描述過休止期脫髮 (telogen effluvium)。
罕見的「惡性」型梅毒 (lues maligna) 表現為快速進展、丘疹膿皰性 (papulopustular) 病灶、大量潰瘍,以及蠣殼狀 (rupial) 病灶(希臘文 rhypos,意為污穢;指被骯髒、層狀結痂覆蓋的壞死性病灶,外觀類似牡蠣殼),主要侵犯面部與四肢。病人亦可表現出發燒、眼部侵犯、肌痛、淋巴腺炎與肝脾腫大。此型梅毒曾被描述與 HIV 感染相關,並以壞死性與潰瘍性病灶為特徵。
繼發性梅毒的表現通常被描述為不搔癢,但情況並非總是如此。事實上,在 Chapel 所發表的 105 名繼發性梅毒病人系列中,有 42% 抱怨搔癢。病灶消退時可能伴隨色素減退或色素增加。淋巴腺病可能廣泛分布、無痛且具橡膠樣質地,發生於 50–85% 的病人。皮膚表現常伴隨發熱 (pyrexia)、頭痛、體重減輕,以及非特異性的肌肉與關節疼痛。骨膜炎 (periostitis) 罕見發生。包括葡萄膜炎 (uveitis) 與視網膜炎 (retinitis) 在內的眼部侵犯,可於疾病的任何階段發生。未治療的梅毒病灶在 2–10 週內消退,但若經治療,則可能出現一種自限性的發熱反應,稱為 Jarisch–Herxheimer 反應,伴隨全身性症狀。
HIV 陽性病人曾被報告出現非典型的梅毒臨床型,且初期梅毒可能出現多發性生殖器潰瘍,繼發性梅毒亦可能同時合併潰瘍。
繼發性梅毒之後接著進入潛伏期 (latent phase),此潛伏期之後可能轉變為:
- 血清陰轉 (seronegativity) 與痊癒,
- 持續性血清陽性 (persistent seropositivity) 但無進一步病灶,
- 發展為第三期 (tertiary) 病灶。這些晚期病灶主要侵犯心血管系統(主動脈瓣閉鎖不全 aortic incompetence)與中樞神經系統(脊髓癆 tabes dorsalis 與麻痺性癡呆 general paresis of the insane),但皮膚病灶則表現為結節潰瘍性 (noduloulcerative) 病灶與梅毒瘤 (gummata),後者傾向以中央壞死與化膿方式潰破。梅毒瘤可在初次感染後長達 15 年才出現。它們是無痛、常潰瘍的堅實皮下結節,好發於頭皮、面部、胸部與腿部(圖 12.114)。結節潰瘍性晚期梅毒病灶表現為表淺結節,向周邊擴展並於中央癒合,形成潰瘍性的匍行性 (serpiginous) 斑塊。第三期梅毒的病灶可見於內臟器官,臨床上可能模擬癌症。
受感染母親所生的嬰兒可能有廣泛的病灶,反映出全身性感染(先天性梅毒 congenital syphilis)。此疾病的發生主要與缺乏產前篩檢有關。這些表現包括許多器官的纖維化,並以骨骼與肺部所見的發炎性變化最為顯著。有時亦可見水皰性皮膚病灶以及牙齒與骨骼的發育不良。先天性梅毒的後期變化典型上為前額隆突 (frontal bossing)、上頜骨短小 (short maxilla)、高拱形齶 (high arched palate)、慢性間質性角膜炎 (chronic interstitial keratitis)、缺刻狀的 (Hutchinson) 門齒 (notched Hutchinson incisors)、桑椹狀臼齒 (Mulberry molars)、第八對腦神經 (VIII cranial nerve) 耳聾,以及鞍鼻 (saddle nose)。其他表現包括無痛性水關節病 (painless hydroarthrosis)、鼻中隔與齶部穿孔,以及如同成人晚期疾病所見的心血管與神經學變化。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
T. pallidum 是一種細長、捲曲的微生物,長 6–16 µm,能夠進行波動式、開瓶器狀 (corkscrew-like) 的運動。在來自初期硬性下疳的檢體中,以暗視野照明 (dark-field illumination) 可輕易觀察到這些微生物,但亦可在培養基中培養生長。那些通常無致病性、以共生菌 (commensals) 形式生活於牙齦周圍的螺旋體,雖然仍被稱為 Treponema,但其實相當不同,最主要的差別在於它們具有右旋螺旋 (right-handed spiral),與 T. pallidum 及其他致病性螺旋體的左旋螺旋 (left-handed spiral) 相反。
T. pallidum 會產生一層非抗原性的黏液被膜 (nonantigenic mucin coat),這在早期感染時可能具有保護作用。此黏液成分可能因宿主發炎細胞所產生的某種成分而增加。一種透明質酸酶 (hyaluronidase) 與 T. pallidum 的表面相關聯,可能促進其在組織中的播散。
螺旋體首次經由黏膜或擦傷皮膚接種後,此微生物即在初期硬性下疳於接種部位發展出來之前已散布至全身,而在接種部位又可再次鑑別出大量螺旋體。
硬性下疳在組織學上的特徵為:初期的表皮增生 (epidermal hyperplasia),伴隨真皮內強烈的淋巴組織球性 (lymphohistiocytic) 與嗜中性球 (neutrophil) 浸潤(圖 12.115–12.117)。可見漿細胞 (plasma cells),但在丘疹性與丘疹鱗屑性的繼發性病灶中數量可能更多(見下文)。其上覆蓋的上皮發生潰瘍,鄰近的表皮常顯示假上皮瘤樣增生 (pseudoepitheliomatous hyperplasia) 並有嗜中性球浸潤。初期病灶的硬結 (induration) 是由於大量的黏液樣物質 (mucoid substance) 所致。血管內皮細胞腫脹常很明顯。可藉由對取自初期病灶的抹片進行暗視野檢查 (dark-field examination) 來顯示這些微生物。銀染色 (silver stain)(如 Warthin-Starry),特別是免疫組織化學 (immunohistochemistry),亦有助於在組織切片中顯示這些微生物。以電子顯微鏡觀察,螺旋體常見於巨噬細胞 (macrophages)、內皮細胞 (endothelial cells)、漿細胞,以及小血管附近的細胞間隙中。硬性下疳的消退,雖然看似與對進一步感染的免疫力以及抗體的出現同時發生,卻無法阻止 treponeme 的廣泛播散與增殖。這導致其在繼發期 (secondary phase) 復發,這是一個尚未被理解的矛盾現象。
繼發性病灶顯示多變的外觀,某種程度上取決於其臨床型態(圖 12.118–12.124)。純粹的斑狀病灶並不具特異性,顯示相當稀疏的血管周圍淋巴組織球性浸潤,漿細胞甚少(若有的話)。表皮正常。當病灶發展出丘疹型態時,則出現表淺與深部的血管周圍浸潤,浸潤亦可能呈帶狀 (bandlike) 分布。皮下組織的侵犯罕見。漁細胞變得較多,且可見角化不全 (parakeratosis)、棘層肥厚 (acanthosis)、海綿水腫 (spongiosis) 與細胞外滲 (exocytosis)。具有腫脹內皮細胞的厚壁血管是特徵性表現。在毛囊與汗腺周圍常見明顯的浸潤。

圖 12.100:初期梅毒 (primary syphilis):口腔硬性下疳 (chancre) 最常位於唇部。By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
Fig. 12.100 Primary syphilis: oral chancres are most often located on the lip. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

圖 12.101:初期梅毒 (primary syphilis):硬性下疳 (chancre) 出現於肛門口 (anal ostium) 邊緣。By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
Fig. 12.101 Primary syphilis: a chancre is present at the edge of the anal ostium. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
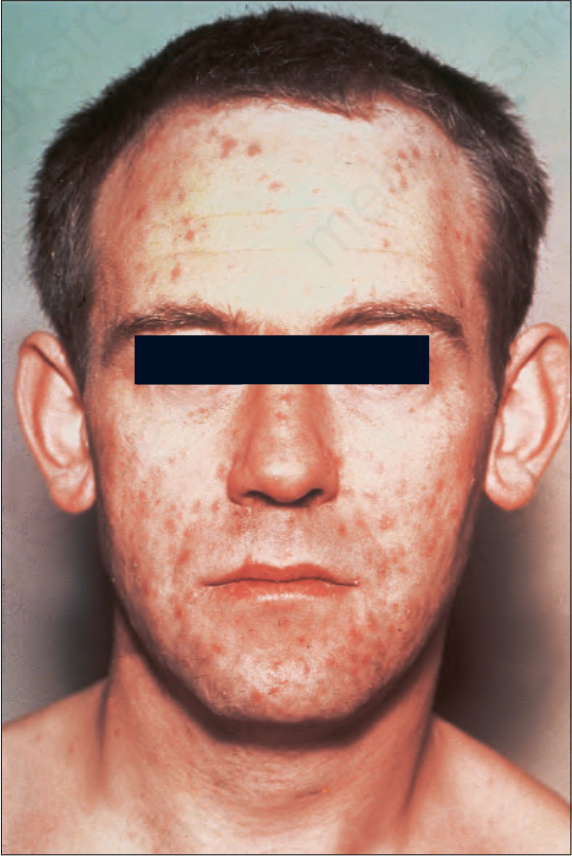
圖 12.102:繼發性梅毒 (secondary syphilis):面部常受侵犯。注意眾多的丘疹 (papules)。By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
Fig. 12.102 Secondary syphilis: the face is commonly affected. Note the numerous papules. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

圖 12.103:繼發性梅毒 (secondary syphilis):此病人顯示廣泛的色素增加性斑丘疹 (hyperpigmented maculopapular eruption)。By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.
Fig. 12.103 Secondary syphilis: this patient shows a widespread hyperpigmented maculopapular eruption. By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.

圖 12.104:繼發性梅毒 (secondary syphilis):注意廣泛的丘疹與結節,其中許多具肥厚性 (hypertrophic) 外觀。By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.
Fig. 12.104 Secondary syphilis: note the widespread papules and nodules many of which have a hypertrophic appearance. By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.

圖 12.105:繼發性梅毒 (secondary syphilis):手掌幾乎無一例外地受侵犯。By courtesy of the Institute of Dermatology, London, UK.
Fig. 12.105 Secondary syphilis: the palms are almost invariably affected. By courtesy of the Institute of Dermatology, London, UK.

圖 12.106:(A, B) 繼發性梅毒 (secondary syphilis):此繼發性梅毒病人出現侵犯手掌與足底的紅斑性鱗屑性丘疹 (erythematous and scaly papules)。(A) By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK;(B) by courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
Fig. 12.106 (A, B) Secondary syphilis: erythematous and scaly papules involving the palms and soles are present in this patient with secondary syphilis. (A) By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK; (B) by courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

圖 12.107:繼發性梅毒 (secondary syphilis):此病人典型的銅幣狀斑疹 (copper penny macules) 伴有周圍的環狀鱗屑 (Biette collarette),與手掌上的融合性脫屑 (confluent exfoliation) 形成對比。By courtesy of the Institute of Dermatology, London, UK.
Fig. 12.107 Secondary syphilis: in this patient, typical copper penny macules with surrounding annular scale (Biette collarette) contrast with confluent exfoliation on the palms. By courtesy of the Institute of Dermatology, London, UK.
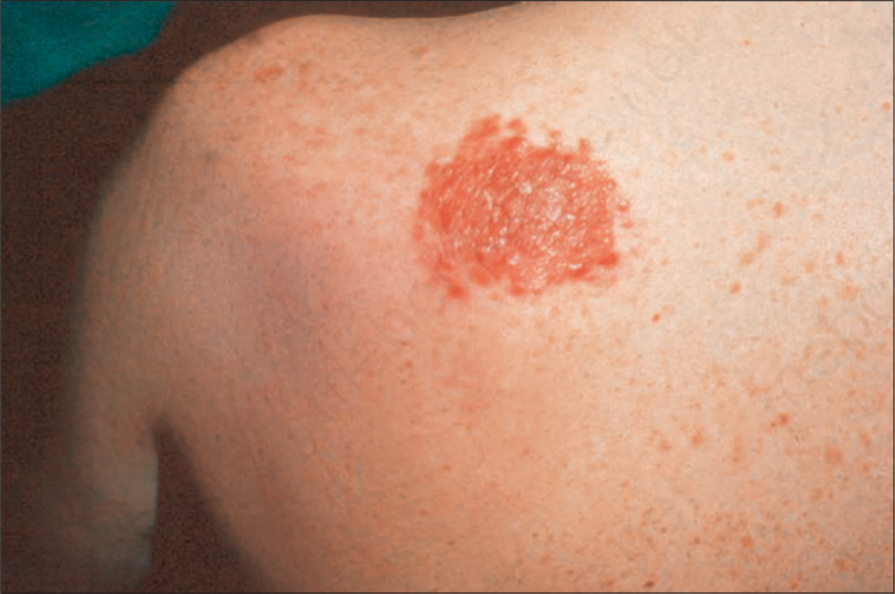
圖 12.108:繼發性梅毒 (secondary syphilis):這是典型的繖房狀 (corymbose) 疹。注意界限分明、融合性的紅斑性鱗屑性丘疹。By courtesy of the Institute of Dermatology, London, UK.
Fig. 12.108 Secondary syphilis: this is a typical corymbose eruption. Note the circumscribed, confluent, erythematous scaly papules. By courtesy of the Institute of Dermatology, London, UK.

圖 12.109:繼發性梅毒 (secondary syphilis):如此病人面部所見的膿皰性病灶 (pustular lesions) 是一種罕見的表現。By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
Fig. 12.109 Secondary syphilis: pustular lesions, as seen on this patient’s face, are a rare manifestation. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
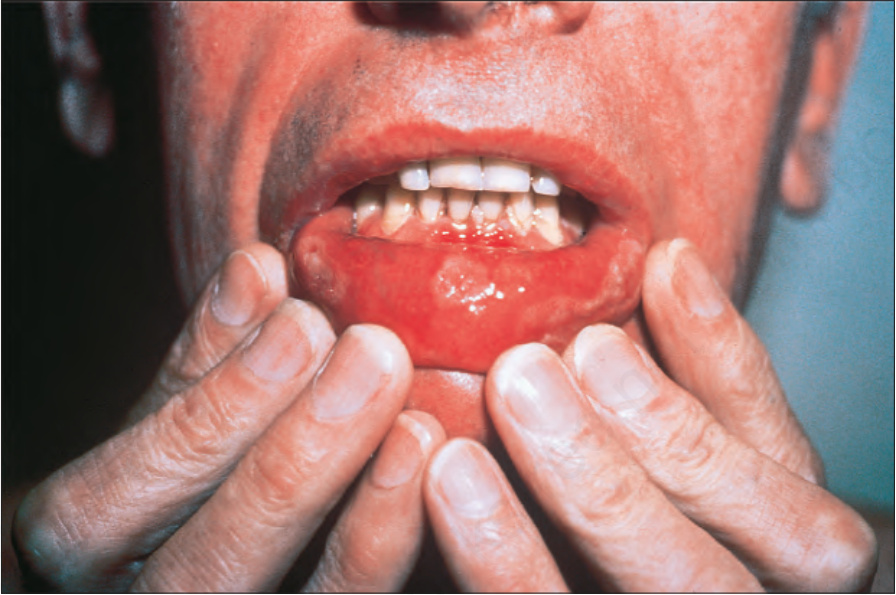
圖 12.110:繼發性梅毒 (secondary syphilis):注意對稱分布的「蝸牛軌跡」(‘snail track’) 潰瘍。By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
Fig. 12.110 Secondary syphilis: note the symmetrically distributed ‘snail track’ ulcers. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

圖 12.111:繼發性梅毒 (secondary syphilis):早期的肛周扁平濕疣 (perianal condylomata lata)。By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
Fig. 12.111 Secondary syphilis: early perianal condylomata lata. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

圖 12.112:繼發性梅毒 (secondary syphilis):此病人的病灶極為類似 pityriasis lichenoides。By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Fig. 12.112 Secondary syphilis: in this patient, the lesions greatly resemble pityriasis lichenoides. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
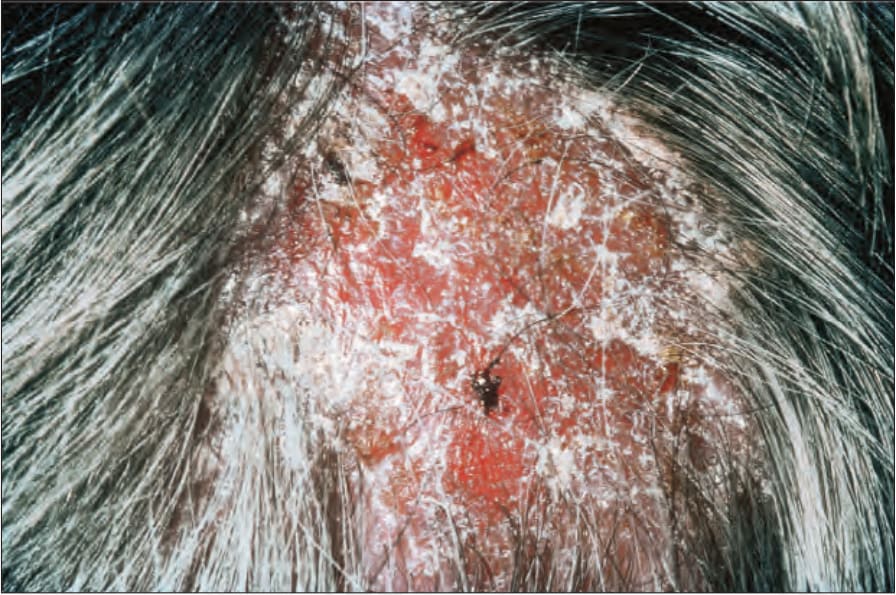
圖 12.113:繼發性梅毒 (secondary syphilis):頭皮侵犯並不少見。注意鱗屑與脫髮。By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.
Fig. 12.113 Secondary syphilis: scalp involvement is not uncommon. Note the scaling and hair loss. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.

圖 12.114:梅毒 (syphilis):如此年長男性所見的梅毒瘤性皮膚病灶 (gummatous cutaneous lesions),目前是一種非常罕見的表現。By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.
Fig. 12.114 Syphilis: the presence of gummatous cutaneous lesions as seen in this elderly male is now a very rare manifestation. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.
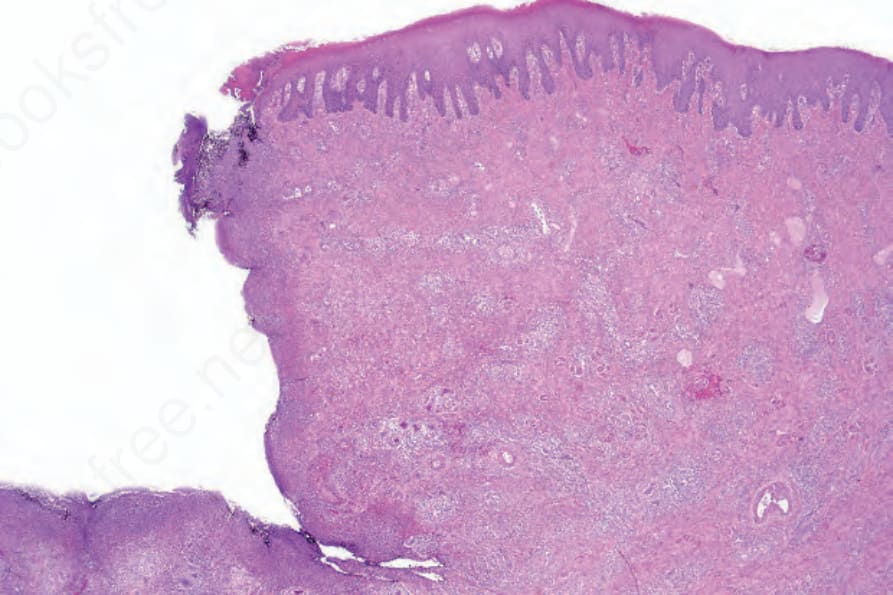
圖 12.115:初期梅毒 (primary syphilis):取自陰莖硬性下疳 (chancre) 的切片。注意典型的穿鑿狀 (punched-out) 外觀。
Fig. 12.115 Primary syphilis: biopsy from a chancre on the penis. Note the typical punchedout appearance.
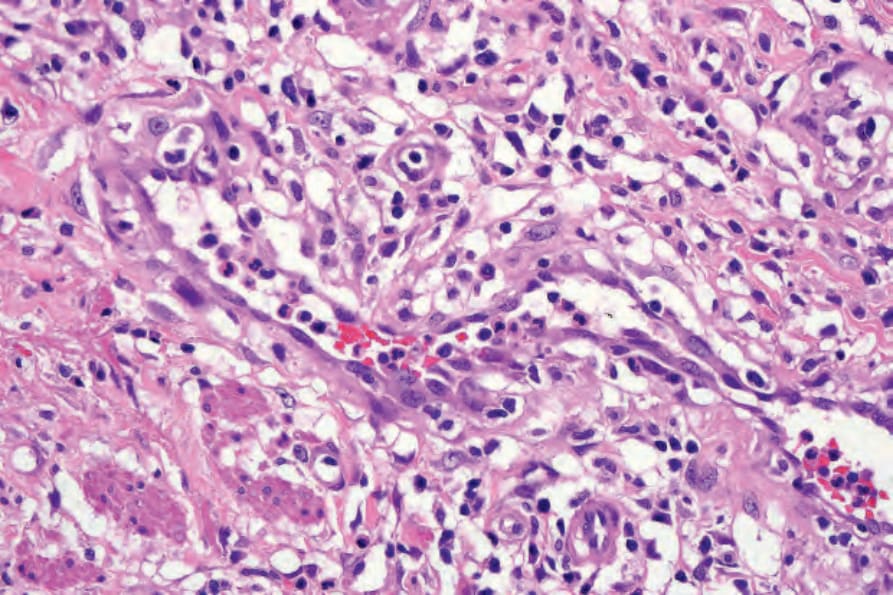
圖 12.116:初期梅毒 (primary syphilis):注意顯著的內皮腫脹 (endothelial swelling)。
Fig. 12.116 Primary syphilis: note the marked endothelial swelling.
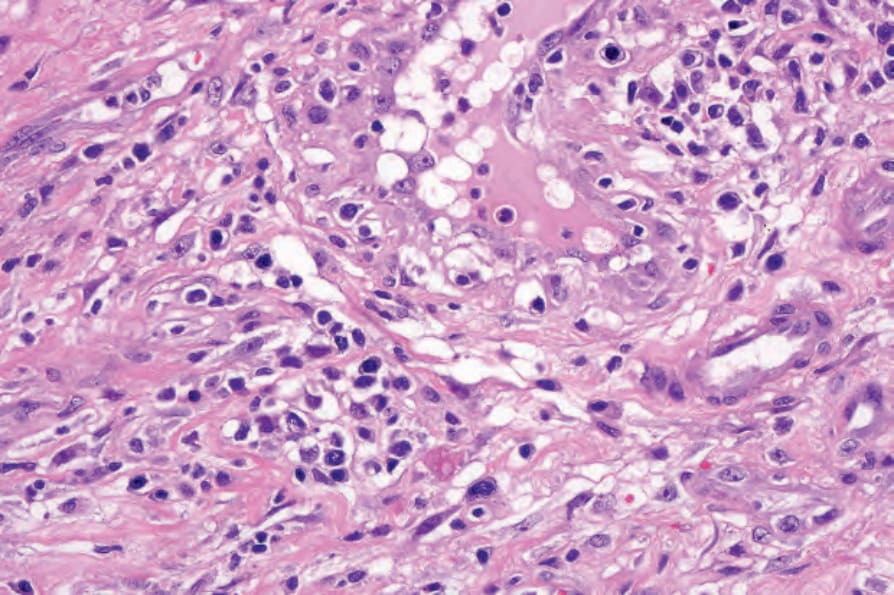
圖 12.117:初期梅毒 (primary syphilis):浸潤由淋巴球 (lymphocytes)、組織球 (histiocytes) 與顯著的漿細胞 (plasma cells) 組成。
Fig. 12.117 Primary syphilis: the infiltrate consists of lymphocytes, histiocytes, and conspicuous plasma cells.
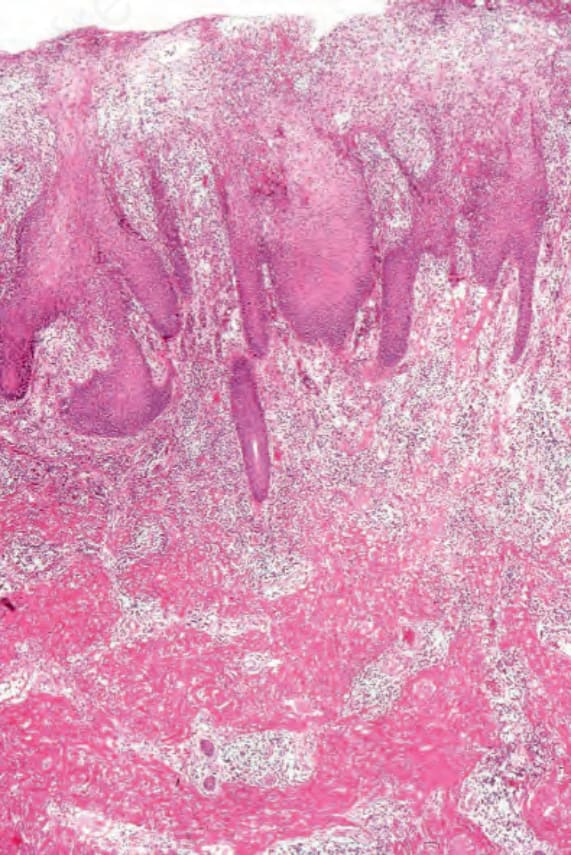
圖 12.118:繼發性梅毒 (secondary syphilis):有非常顯著的角化過度 (hyperkeratosis) 與角化不全 (parakeratosis)。表皮顯示乾癬樣增生 (psoriasiform hyperplasia)。固有層 (lamina propria) 中可見緻密的發炎細胞浸潤。此檢體取自一個扁平濕疣 (condyloma lata)。
Fig. 12.118 Secondary syphilis: there is very marked hyperkeratosis and parakeratosis. The epidermis shows psoriasiform hyperplasia. A dense inflammatory cell infiltrate is present in the lamina propria. This specimen comes from a condyloma lata.
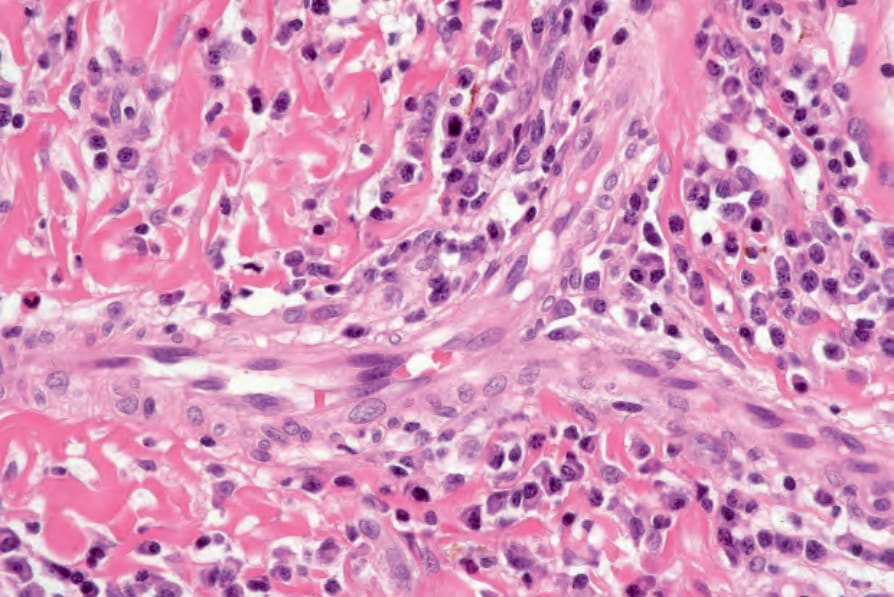
圖 12.119:繼發性梅毒 (secondary syphilis):浸潤含有大量漿細胞 (plasma cells)。此檢體取自一個扁平濕疣 (condyloma lata)。
Fig. 12.119 Secondary syphilis: the infiltrate contains large numbers of plasma cells. This specimen comes from a condyloma lata.
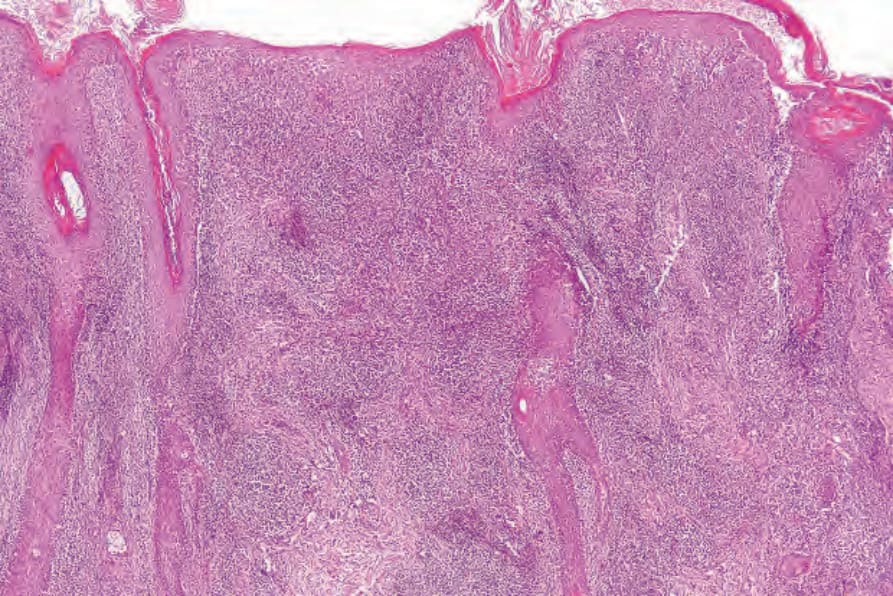
圖 12.120:繼發性梅毒 (secondary syphilis):此例中有角化過度 (hyperkeratosis)、不規則棘層肥厚 (irregular acanthosis) 與非常緻密的真皮浸潤。
Fig. 12.120 Secondary syphilis: in this example, there is hyperkeratosis, irregular acanthosis and a very dense dermal infiltrate.
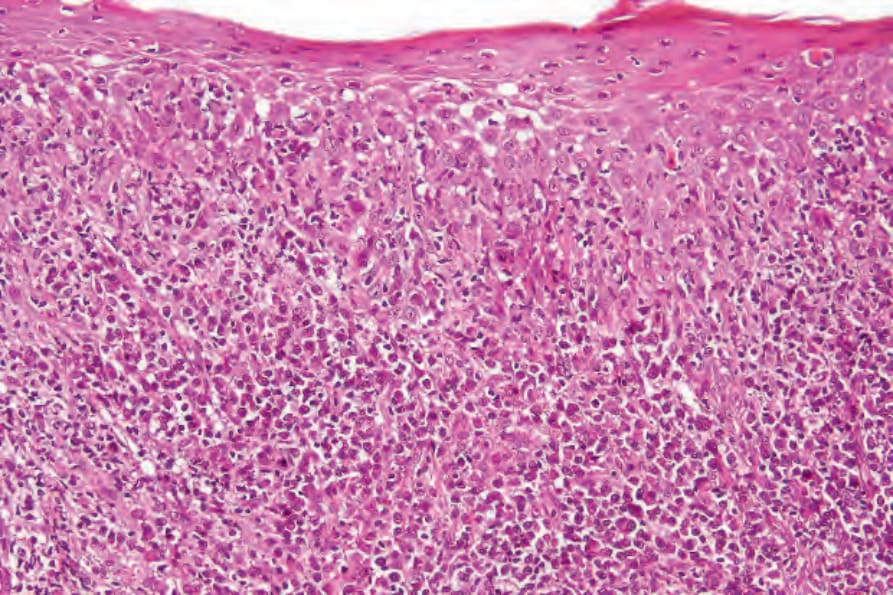
圖 12.121:繼發性梅毒 (secondary syphilis):可見明顯的海綿水腫 (spongiosis)。
Fig. 12.121 Secondary syphilis: spongiosis is evident.

圖 12.95:初期硬性下疳 (primary chancre):硬性下疳是一個無痛性潰瘍,邊緣質地堅硬 (indurated)。其基底呈黃色並藏有大量螺旋體 (spirochetes)。By courtesy of F. Lim, MD, King’s College Hospital, London, UK.
Fig. 12.95 Primary chancre: the chancre is a painless ulcer with an indurated edge. The base is yellow and harbors large numbers of spirochetes. By courtesy of F. Lim, MD, King’s College Hospital, London, UK.

圖 12.96:初期梅毒 (primary syphilis):常出現無痛性淋巴腺病 (painless lymphadenopathy)。By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.
Fig. 12.96 Primary syphilis: painless lymphadenopathy is often present. By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.

圖 12.97:初期梅毒 (primary syphilis):此病人的硬性下疳 (chancre) 具有穿鑿狀 (punched-out) 外觀。By courtesy of the Institute of Dermatology, London, UK.
Fig. 12.97 Primary syphilis: in this patient, the chancre has a punched-out appearance. By courtesy of the Institute of Dermatology, London, UK.

圖 12.98:初期梅毒 (primary syphilis):左側大陰唇 (left labium majus) 出現典型的硬性下疳 (chancre)。By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
Fig. 12.98 Primary syphilis: a typical chancre is present on the left labium majus. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

圖 12.99:初期梅毒 (primary syphilis):前庭 (vestibule) 內出現典型的「對吻性潰瘍」(‘kissing ulcers’)。By courtesy of D. Barlowe, MD, St Thomas’ Hospital, London, UK.
Fig. 12.99 Primary syphilis: typical ‘kissing ulcers’ are present within the vestibule. By courtesy of D. Barlowe, MD, St Thomas’ Hospital, London, UK.
曾有報告指出,早期病灶顯示血管周圍嗜中性球與大量嗜中性球浸潤,模擬 Sweet syndrome。乾癬樣梅毒疹 (psoriasiform syphilids) 顯示角化不全與棘層肥厚,伴有延長的(乾癬樣)表皮突 (epidermal ridges)。發炎細胞浸潤同時呈血管周圍與表淺分布,且呈帶狀 (bandlike) 分布。可見海綿狀膿皰化 (spongiform pustulation) 與嗜中性球外滲 (neutrophil exocytosis),有時亦可見局部細胞水腫性變性 (hydropic degeneration)。偶可見角質細胞壞死 (keratinocyte necrosis)。白血球碎裂性血管炎 (leukocytoclastic vasculitis) 非常罕見。近期一項研究報告,最常見的組織學特徵為乾癬樣增生 (psoriasiform hyperplasia) 伴有細長延長的表皮突 (rete ridges)、漿細胞,以及內皮細胞腫脹。
紅血球外滲 (erythrocyte extravasation) 可能是丘疹性與丘疹鱗屑性變異型兩者的特徵。在丘疹性與丘疹鱗屑性疹中都曾描述過肉芽腫性 (granulomatous) 成分,但這並非恆定的特徵。除了緻密的真皮浸潤之外,在繖房狀梅毒 (corymbose syphilis) 中可見大量漿細胞與偶見的巨細胞 (giant cells)。繼發性梅毒中微生物的數量不等。傳統上,它們是藉由銀染色 (silver stains)(主要為 Warthin-Starry)來鑑別的。然而,後者方法耗時且難以判讀。這些微生物亦可藉由 PCR 鑑別,且有一種針對 T. pallidum 的多株抗體 (polyclonal antibody) 可供免疫組織化學使用(圖 12.125)。在梅毒的診斷上,PCR 與免疫組織化學都比組織化學 (histochemistry) 具有更高的特異性。在初期梅毒,微生物同時見於表皮內與血管周圍;而在繼發性梅毒,微生物主要見於表皮內,這顯示這些模式可作為區分梅毒兩個階段的輔助依據。亦曾藉由反射式共軛焦顯微鏡 (reflectance confocal microscopy) 在活體 (in vivo) 的表皮中鑑別出此細菌。在一例惡性梅毒 (malignant syphilis) 中,病灶中發現的微生物數量出乎意料地非常少。在一例梅毒性脫髮 (alopecia syphilitica) 中曾於毛囊內顯示出螺旋體。
繼發性梅毒的結節型變異型可能伴隨肉芽腫性 (granulomatous) 或假淋巴瘤性 (pseudolymphomatous) 的組織學表現。某些病灶可含有數量可觀的 CD30 陽性非典型 T 細胞。這些肉芽腫可模擬類肉瘤病 (sarcoid) 的肉芽腫,且罕見情況下可呈柵欄狀 (palisaded) 分布,類似環狀肉芽腫 (granuloma annulare)。蠣殼狀 (rupial) 與濕疣狀 (condylomatous) 型則以顯著的表皮增生、海綿水腫,以及嗜中性球浸潤為特徵。真皮中含有非常緻密的發炎細胞浸潤,包括大量漿細胞。血管變化顯著。
晚期繼發性病灶 (late secondary lesions) 以組織球性肉芽腫 (histiocytic granulomata) 為典型表現。這些肉芽腫界限不清,且通常不含多核巨細胞 (multinucleated giant cells)。它們可藉由周邊大量的漿細胞與小血管腫脹的內皮 (swollen endothelia) 與結核病 (tuberculosis) 區分。曾有一例晚期潛伏梅毒 (late latent syphilis) 報告顯示真皮中有明顯的黏蛋白 (dermal mucin),模擬結締組織疾病 (connective tissue disease)。
梅毒瘤 (gummata) 的特徵為類似乾酪樣壞死 (caseation) 的中央壞死,但可見殘餘細胞輪廓 (residual cell outlines) 的隱約跡象(圖 12.126)。壞死周圍環繞著淋巴組織球性與漿細胞浸潤,並伴有纖維化。螺旋體非常稀少,使用銀染色非常難以找到。常見動脈內膜炎 (endarteritis)。
結節潰瘍性病灶 (noduloulcerative lesions) 為肉芽腫性,且典型上無顯著的壞死。據稱漿細胞不明顯,因此可能造成相當大的診斷困難。
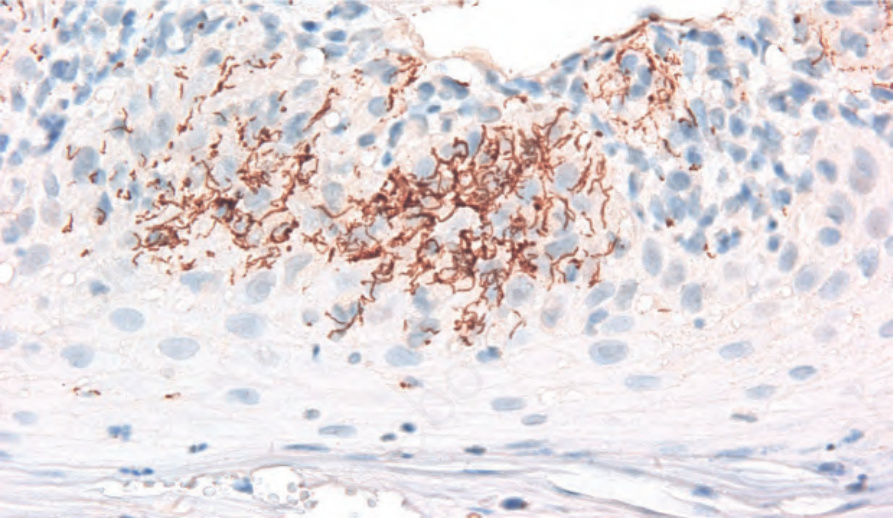
圖 12.125:繼發性梅毒 (secondary syphilis):在一名繼發性梅毒病人,以免疫組織化學 (immunohistochemistry) 可在表皮內見到大量螺旋體 (spirochetes)。
Fig. 12.125 Secondary syphilis: numerous spirochetes are seen by immunohistochemistry within the epidermis in a patient with secondary syphilis.
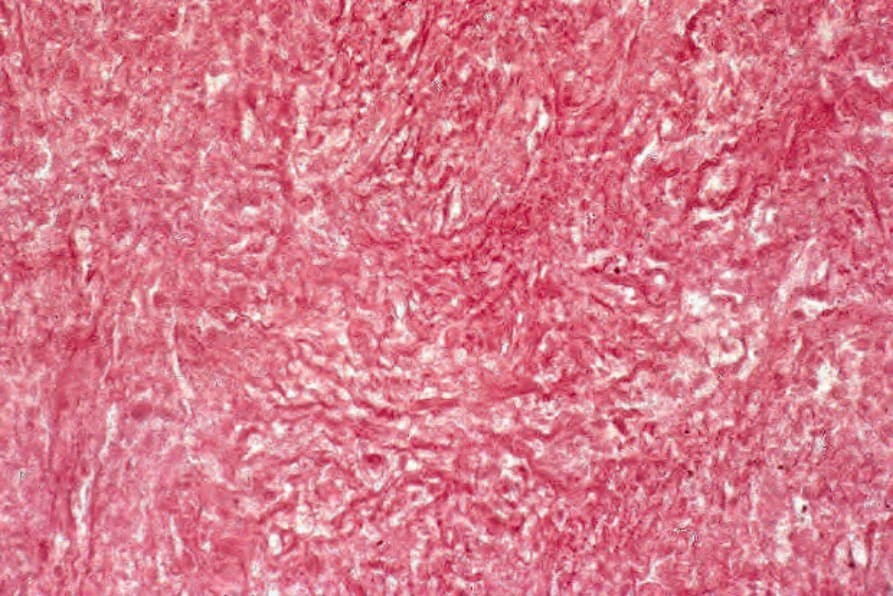
圖 12.126:梅毒瘤 (gumma):高倍視野顯示細胞與結締組織的幽靈狀輪廓 (ghost outlines)。
Fig. 12.126 Gumma: high-power view reveals ghost outlines of cells and connective tissue.