Syphilis
Syphilis
Clinical features The incidence of syphilis fell dramatically after the introduction of penicillin in the 1940s. In recent years the incidence has been rising annually largely due to the increased number of cases of HIV infection. Drug abuse and high-risk sexual behavior are also contributory factors.1 The increase in the incidence of syphilis continues, especially in HIV-infected patients with predilection for young homosexual black males.2
In the sixteenth century, syphilis carried a high mortality associated with a chronic disfiguring and disabling disease. The disease currently appears less aggressive, even in untreated cases. It is highly infectious, with the risk of transmission from an infected partner estimated at up to 60%.3 The chance of acquiring the disease depends on the number of exposures, type of sexual practice, and the location and number of the partner’s lesions. There is a close relationship between syphilis and HIV infection, and both diseases can be acquired together.4 It is recognized that diseases such as syphilis that induce genital ulceration increase the risk of acquiring HIV infection.4
The causative organism is Treponema pallidum, a spirochete with fastidious growth requirements. Transmission is primarily sexual. An endemic form known as bejel, caused by an identical organism, occurs in children living in conditions of poor hygiene and is transmitted by cutaneous inoculation.5 Other endemic forms have been associated with shared drinking vessels when some members of the community have oral or labial syphilitic lesions.
The typical initial lesion, a chancre, develops 20–30 days after exposure to the organism at the site of inoculation. This can be anywhere on the anogenital skin, more often on the glans penis (especially the coronal sulcus), the shaft, or prepuce, or on the labia majora or minora (Figs 12.95–12.99). At least 5% of primary chancres arise at extragenital locations, most commonly oral, but virtually every other part of the skin surface may be affected
501 Infectious diseases
including the tonsils, fingers, eyelids, and nipples (Figs 12.100 and 12.101).6 Lesions in the vagina or cervix may go undetected. The chancre appears as an indurated, punched-out, painless ulcer. It is usually accompanied by painless lymphadenopathy. This resolves without scarring after 1–5 weeks.
The secondary cutaneous lesions (syphilids) are highly infectious and may mimic virtually any skin disorder. They present 6–8 weeks after the appearance of the chancre. They develop insidiously (in up to 80% of patients), with a roseolar, macular–erythematous rash, on the head, face, and neck followed by a polymorphic papular eruption. The macules measure 5–10 mm in diameter, are not pruritic, and particularly occur on the trunk, abdomen, and limbs, especially the palms and soles (Figs 12.102–12.107).7 The papular lesions are characteristically coppery red in color and 3–10 mm in diameter. Hypopigmentation of the neck is known as the ‘collar of venus’.
are acneiform, varioliform, and rarely, necrotic (Fig. 12.112). Lesions tend to be widely disseminated and often symmetrical in distribution. Papular involvement of the scalp may result in nonscarring, patchy alopecia (Fig. 12.113).17 The alopecia induced by secondary syphilis is known as alopecia syphilitica and has a characteristic, moth-eaten appearance. The beard, eyebrows, and eyelashes may also be affected. Telogen effluvium has also been described.
Other manifestations described include condylomata (in intertriginous areas), annular, lichenoid, papulosquamous lesions (psoriasiform), arcuate lesions, corymbose brownish-red papules (Gr. korymbos, clusters of ivy flowers), bullous, erythema multiforme-like follicular and pustular variants on the skin, with erosive ulcers (mucous patches), often of ‘snail track’ type, and the (highly infectious) condylomata lata affecting the mucosae (Figs 12.108–12.111).8–15 Keratoderma can also be seen.16 Large hypertrophic condylomata are known as framboiseform syphilids.6 Other variants described
Rare ‘malignant’ forms of syphilis (lues maligna) present with rapid progression, papulopustular lesions, much ulceration, and rupial lesions (Gr. rhypos, filth; necrotic lesions covered by dirty, lamellated encrustation resembling oyster shells) mainly affecting the face and limbs.18 Patients can also present with fever, eye involvement, myalgia, lymphadenitis, and hepatosplenomegaly.19 This form of syphilis has been described in association with HIV infection and is characterized by necrotic and ulcerative lesions.20
Secondary syphilis manifestations have typically been described as nonpruritic, but this is not always the case.21 Indeed, in the series of 105 patients with secondary syphilis published by Chapel, 42% complained of pruritus.22 Resolution may be accompanied by hypo- or hyperpigmentation. Lymphadenopathy, which may be widespread and is painless and rubbery, occurs in 50–85% of patients. The cutaneous manifestations are often accompanied by pyrexia, headache, weight loss, and non-specific muscle and joint
502 Diseases of the anogenital skin
aches. Periostitis can rarely occur.23 Ocular involvement including uveitis and retinitis can occur at any stage of the disease.24 Untreated lesions of syphilis resolve in 2–10 weeks, but if treated., there may be a self-limited febrile reaction known as the Jarisch–Herxheimer reaction associated with systemic symptoms.
occur up to 15 years after the initial infection. They are painless, frequently ulcerated, firm subcutaneous nodules that show a predilection for the scalp, face, chest, and legs (Fig. 12.114).28 Noduloulcerative late syphilitic lesions present as superficial nodules that extend peripherally and heal centrally to form ulcerated serpiginous plaques. Lesions of tertiary syphilis can be seen in internal organs and may clinically mimic cancer.29
Atypical clinical forms of syphilis have been reported in HIV-positive patients,25,26 and multiple genital ulcers may occur in primary syphilis as well as concomitant ulcer with secondary syphilis.27
Secondary syphilis is followed by a latent phase, which may precede a change to:
• seronegativity and cure,
• persistent seropositivity without further lesions,
• development of tertiary lesions. These late lesions involve mainly the cardiovascular (aortic incompetence) and central nervous system (tabes dorsalis and general paresis of the insane), but cutaneous lesions are seen as noduloulcerative lesions and gummata that tend to break down with central necrosis and suppuration. Gummata may
Infants born to infected mothers may have widespread lesions reflecting a systemic infection (congenital syphilis). Development of the disease is mainly associated with lack of antenatal screening. These include fibrosis in many organs, with inflammatory changes seen particularly in bones and lungs. Vesicular skin lesions and maldevelopment of teeth and bone are also sometimes evident. Later changes of congenital syphilis are classically frontal bossing, a short maxilla, a high arched palate, chronic interstitial keratitis, notched (Hutchinson) incisors, Mulberry molars, VIII cranial nerve deafness, and saddle nose.30 Other manifestations include painless hydroarthrosis, perforation of the nasal septum and palate, and cardiovascular and neurological changes, as seen in late-stage adult disease.
Pathogenesis and histologic features T. pallidum is a slender, coiled organism, 6–16 µm long, capable of an undulating, corkscrew-like motion. The organisms are readily visualized in
503 Infectious diseases
A
B
material from a primary chancre with dark-field illumination, but can also be grown in culture. The usually nonpathogenic spirochetes, which live as commensals around the gingiva, although still termed Treponema, are quite different, not least in that they have a right-handed spiral in contrast to the left-handed spiral of T. pallidum and other pathogenic spirochetes.
T. pallidum produces a nonantigenic mucin coat, which may be protective in early infections. This mucoid element may be increased by a component produced by host inflammatory cells. A hyaluronidase is associated with the surface of T. pallidum and may facilitate dissemination in tissues.31
After the first inoculation of the spirochete through mucosa or abraded skin, the organism becomes systemically distributed before the primary chancre develops at the site of inoculation and numerous spirochetes can again be identified.
The chancre is characterized histologically by initial epidermal hyperplasia with an intense lymphohistiocytic and neutrophil infiltrate in the dermis (Figs 12.115–12.117). Plasma cells are present, but may be more numerous in papular and papulosquamous secondary lesions (see below). The overlying epithelium becomes ulcerated, and the adjacent epidermis often shows pseudoepitheliomatous hyperplasia and infiltration by neutrophils. The induration of the primary lesion is due to a large amount of mucoid
504 Diseases of the anogenital skin
substance. Vascular endothelial cell swelling is often prominent. The organisms can be demonstrated by dark-field examination of a smear taken from the primary lesion. A silver stain such as Warthin-Starry and particularly immunohistochemistry are also useful in demonstrating the organisms in tissue sections. By electron microscopy, the spirochetes are often found in macrophages, endothelial cells, plasma cells, and in the intercellular space close to small blood vessels.32 Resolution of the chancre, while appearing to coincide with immunity to further infection and demonstration of antibodies, nevertheless does not impede the widespread dissemination and proliferation of the treponeme. This leads to its recrudescence in the secondary phase, a paradox that is not understood.
Secondary lesions show variable appearances depending to some extent on the clinical morphology (Figs 12.118–12.124).33–36 Purely macular lesions are not distinctive and show a rather sparse perivascular lymphohistiocytic infiltrate with few, if any, plasma cells. The epidermis is normal. As the lesions develop a papular morphology, superficial and deep perivascular infiltrates develop, which may also adopt a bandlike distribution. Involvement of the subcutis is rare. Plasma cells become more numerous, and parakeratosis, acanthosis, spongiosis, and exocytosis may be evident. Thick-walled blood vessels with swollen endothelial cells are characteristic. A prominent infiltrate is often present around hair follicles and sweat glands. Early

Fig. 12.100 Primary syphilis: oral chancres are most often located on the lip. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

Fig. 12.101 Primary syphilis: a chancre is present at the edge of the anal ostium. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
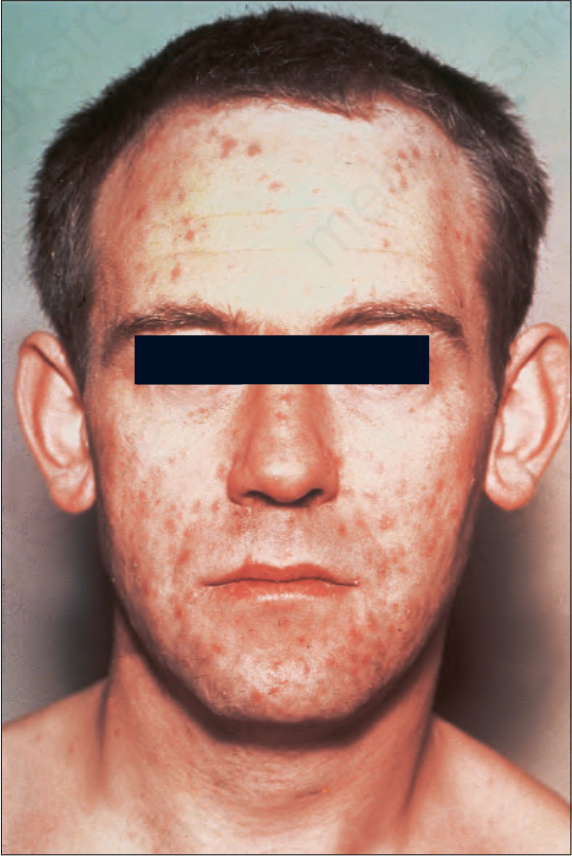
Fig. 12.102 Secondary syphilis: the face is commonly affected. Note the numerous papules. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

Fig. 12.103 Secondary syphilis: this patient shows a widespread hyperpigmented maculopapular eruption. By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.

Fig. 12.104 Secondary syphilis: note the widespread papules and nodules many of which have a hypertrophic appearance. By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.

Fig. 12.105 Secondary syphilis: the palms are almost invariably affected. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.106 (A, B) Secondary syphilis: erythematous and scaly papules involving the palms and soles are present in this patient with secondary syphilis. (A) By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK; (B) by courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

Fig. 12.107 Secondary syphilis: in this patient, typical copper penny macules with surrounding annular scale (Biette collarette) contrast with confluent exfoliation on the palms. By courtesy of the Institute of Dermatology, London, UK.
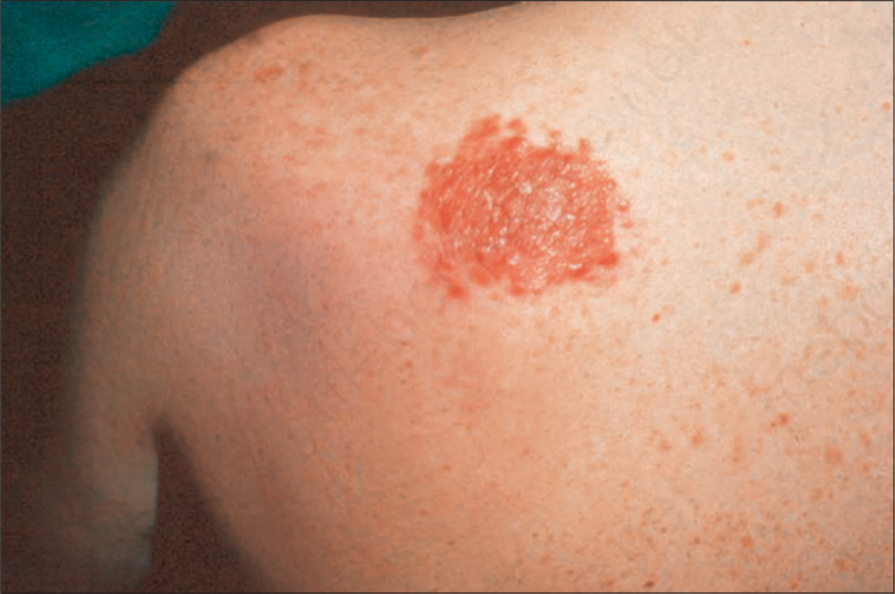
Fig. 12.108 Secondary syphilis: this is a typical corymbose eruption. Note the circumscribed, confluent, erythematous scaly papules. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.109 Secondary syphilis: pustular lesions, as seen on this patient’s face, are a rare manifestation. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.
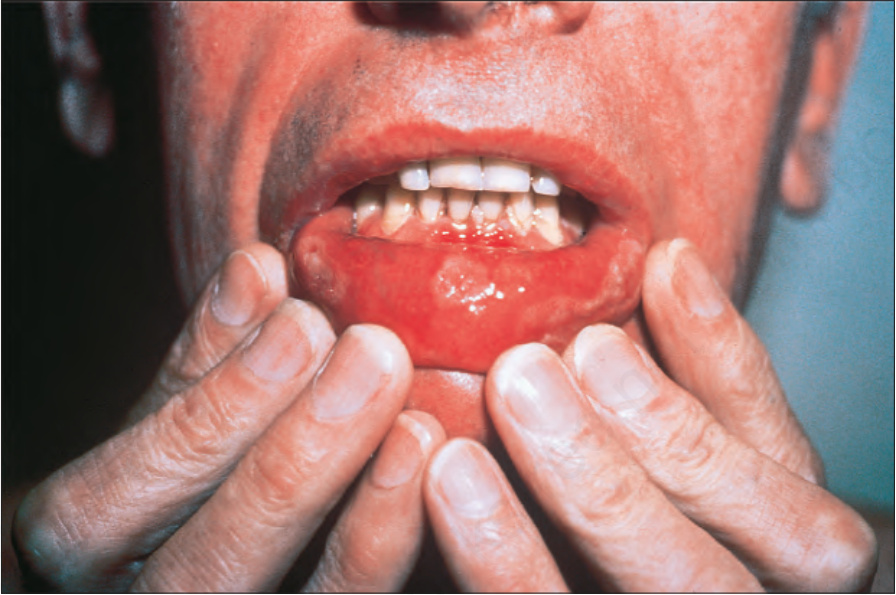
Fig. 12.110 Secondary syphilis: note the symmetrically distributed ‘snail track’ ulcers. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

Fig. 12.111 Secondary syphilis: early perianal condylomata lata. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

Fig. 12.112 Secondary syphilis: in this patient, the lesions greatly resemble pityriasis lichenoides. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
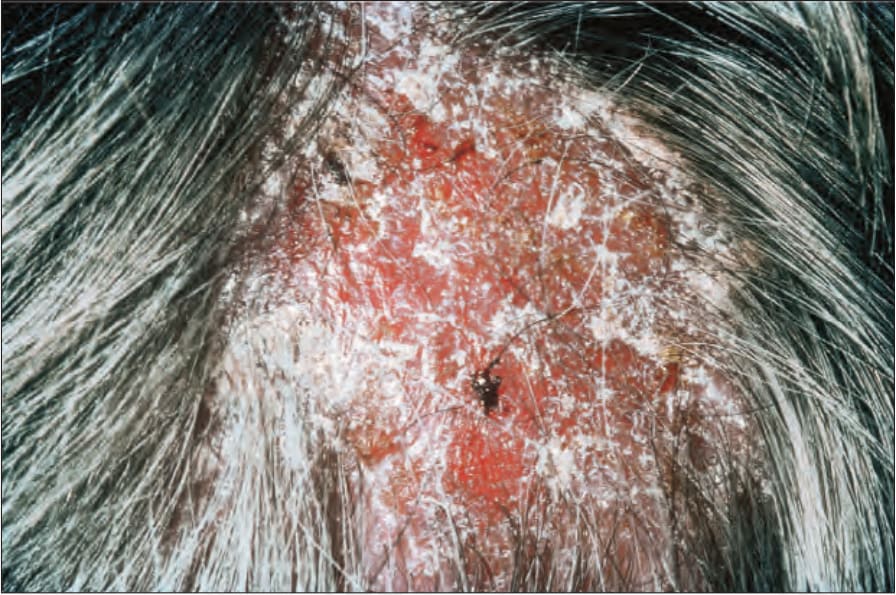
Fig. 12.113 Secondary syphilis: scalp involvement is not uncommon. Note the scaling and hair loss. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.

Fig. 12.114 Syphilis: the presence of gummatous cutaneous lesions as seen in this elderly male is now a very rare manifestation. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.
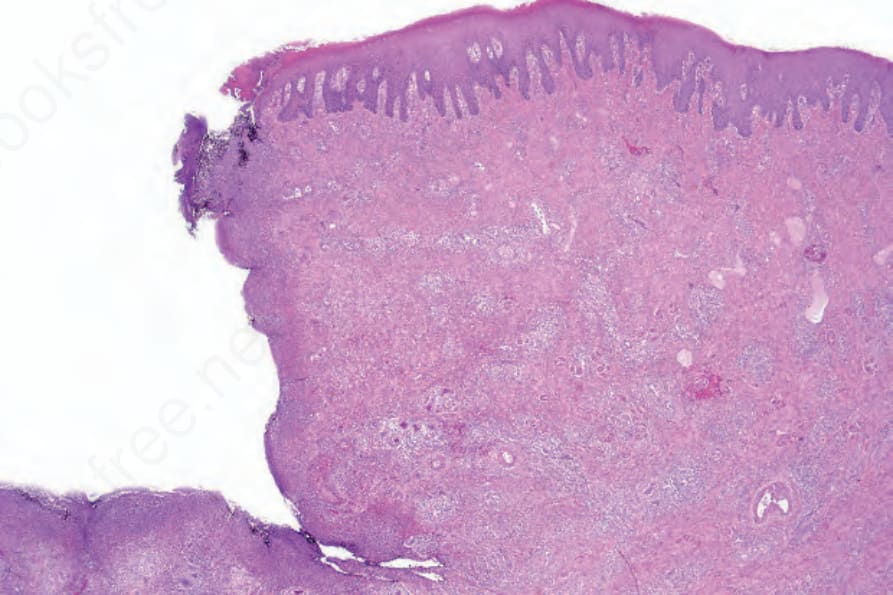
Fig. 12.115 Primary syphilis: biopsy from a chancre on the penis. Note the typical punchedout appearance.
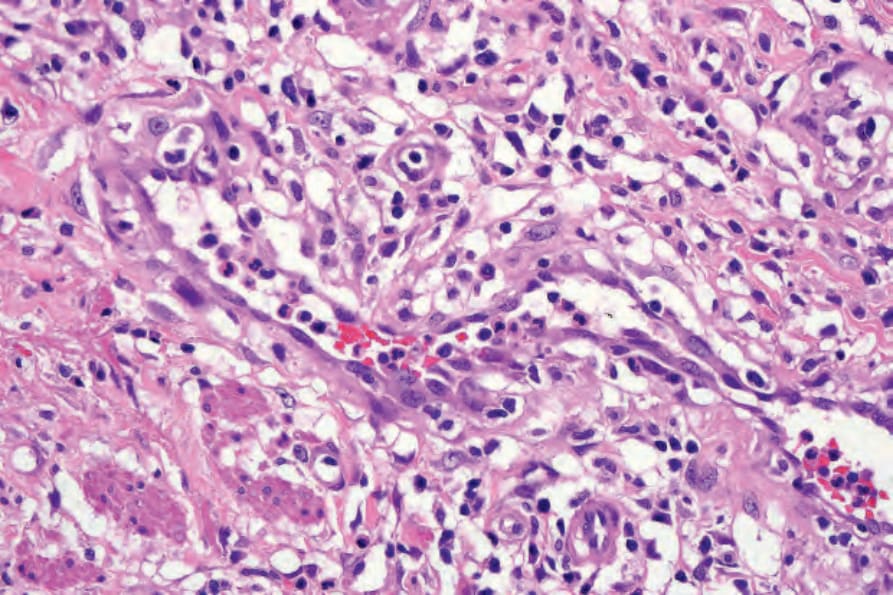
Fig. 12.116 Primary syphilis: note the marked endothelial swelling.
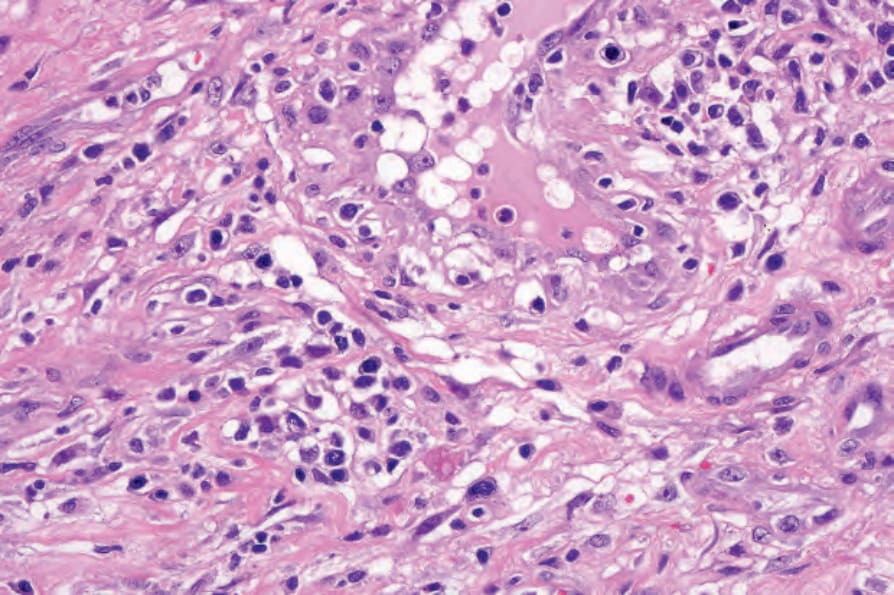
Fig. 12.117 Primary syphilis: the infiltrate consists of lymphocytes, histiocytes, and conspicuous plasma cells.
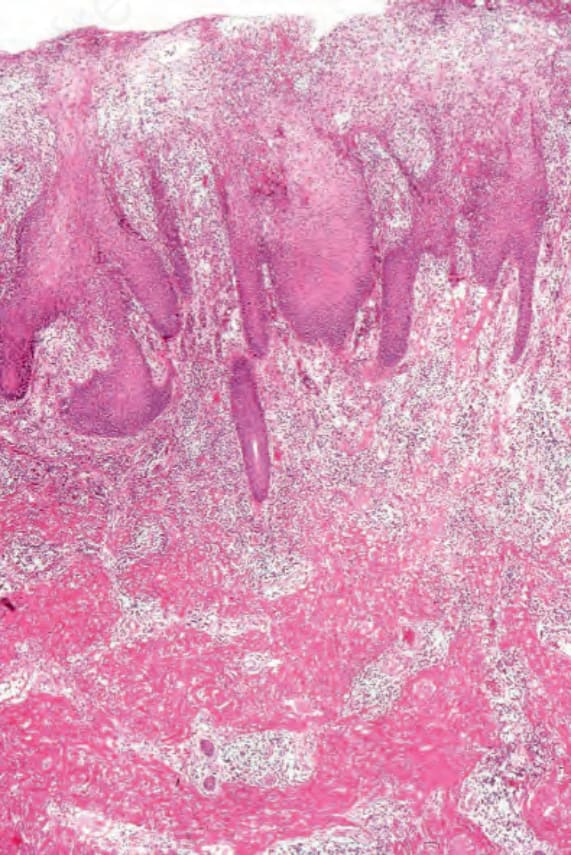
Fig. 12.118 Secondary syphilis: there is very marked hyperkeratosis and parakeratosis. The epidermis shows psoriasiform hyperplasia. A dense inflammatory cell infiltrate is present in the lamina propria. This specimen comes from a condyloma lata.
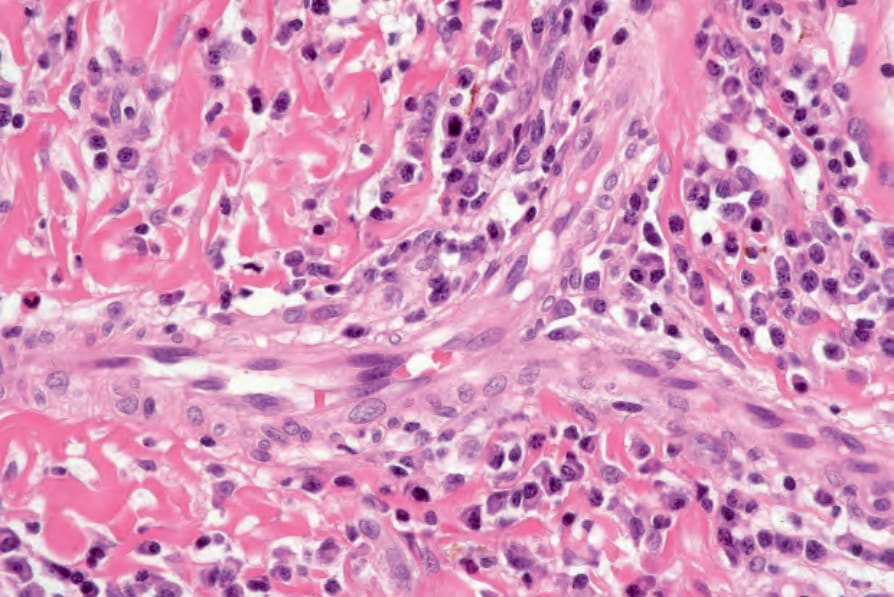
Fig. 12.119 Secondary syphilis: the infiltrate contains large numbers of plasma cells. This specimen comes from a condyloma lata.
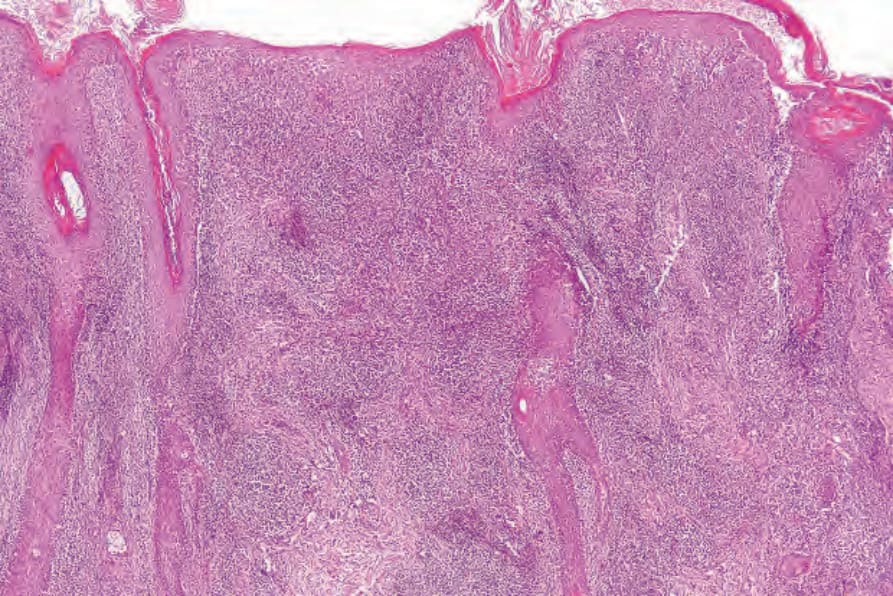
Fig. 12.120 Secondary syphilis: in this example, there is hyperkeratosis, irregular acanthosis and a very dense dermal infiltrate.
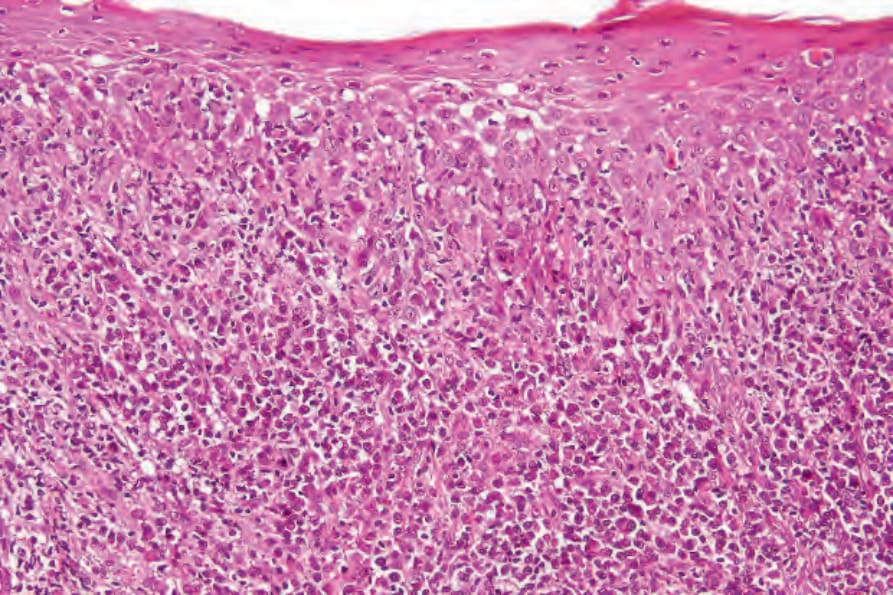
Fig. 12.121 Secondary syphilis: spongiosis is evident.

Fig. 12.95 Primary chancre: the chancre is a painless ulcer with an indurated edge. The base is yellow and harbors large numbers of spirochetes. By courtesy of F. Lim, MD, King’s College Hospital, London, UK.

Fig. 12.96 Primary syphilis: painless lymphadenopathy is often present. By courtesy of C. Furlonge, MD, Port of Spain, Trinidad.

Fig. 12.97 Primary syphilis: in this patient, the chancre has a punched-out appearance. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.98 Primary syphilis: a typical chancre is present on the left labium majus. By courtesy of R.N. Thin, MD, St Thomas’ Hospital, London, UK.

Fig. 12.99 Primary syphilis: typical ‘kissing ulcers’ are present within the vestibule. By courtesy of D. Barlowe, MD, St Thomas’ Hospital, London, UK.
lesions showing perivascular neutrophils and a heavy neutrophilic infiltrate mimicking Sweet syndrome has been reported.37 Psoriasiform syphilids show parakeratosis and acanthosis with extended (psoriasiform) epidermal ridges. The inflammatory cell infiltrate is both perivascular and superficial, and bandlike in distribution. Spongiform pustulation and neutrophil exocytosis may be evident, and focal cell hydropic degeneration can sometimes be present.8,36 Keratinocyte necrosis may occasionally be seen. Leukocytoclastic vasculitis is very rare.38 A recent study reported the most frequent histologic features to be psoriasiform hyperplasia with slender elongated rete ridges, plasma cells, and endothelial cell swelling.39
Erythrocyte extravasation may be a feature of both papular and papulosquamous variants. A granulomatous element has been described in both papular and papulosquamous eruptions, but this is not a constant feature.36 In addition to a dense dermal infiltrate, large numbers of plasma cells and occasional giant cells are seen in corymbose syphilis. The number of organisms in secondary syphilis varies. Traditionally, they have been identified by
505 Infectious diseases
an impressive number of CD30-positive atypical T cells.51 The granulomata can mimic those of sarcoid and may rarely have a palisaded distribution resembling granuloma annulare.48,52 The rupial and condylomatous forms are characterized by marked epidermal hyperplasia, spongiosis, and a neutrophil infiltrate. The dermis contains a very heavy inflammatory cell infiltrate including numerous plasma cells. Vascular changes are marked.
the use of silver stains, mainly Warthin-Starry. However, the latter method is time consuming and difficult to interpret. The organisms can also be identified by PCR, and a polyclonal antibody against T. pallidum is available for immunohistochemistry (Fig. 12.125).40–43 Both PCR and immunohistochemistry are much more specific than histochemistry in the diagnosis of syphilis.42–44 In primary syphilis, the organisms are found both within the epidermis and around blood vessels, whereas in secondary syphilis organisms are mainly found within the epidermis, suggesting that these patterns can be used as an aid in distinction between the two stages of syphilis.43 The bacteria have also been identified in vivo in the epidermis by the use of reflectance confocal microscopy.45 In a case of malignant syphilis, a surprisingly very low number of organisms was found in the lesions.46 Spirochetes have been demonstrated within hair follicles in a case of alopecia syphilitica.47
The nodular variants of secondary syphilis may be associated with granulomatous or pseudolymphomatous histology.48–50 Some lesions can contain
Late secondary lesions are typified by histiocytic granulomata. These are not well circumscribed and do not usually include multinucleated giant cells. They can be distinguished from tuberculosis by the presence of numerous plasma cells peripherally and the swollen endothelia of small blood vessels. A case of late latent syphilis with prominent dermal mucin mimicking a connective tissue disease has been reported.53
Gummata are characterized by central necrosis similar to caseation, but with a visible suggestion of residual cell outlines (Fig. 12.126). The necrosis is surrounded by a lymphohistiocytic and plasma cell infiltrate with fibrosis. Spirochetes are very scanty and very difficult to find with the use of silver stains. Endarteritis is often evident.
Noduloulcerative lesions are granulomatous, and typically there is no significant necrosis. Plasma cells are said to be inconspicuous, which may therefore cause considerable diagnostic difficulty.54
506 Diseases of the anogenital skin
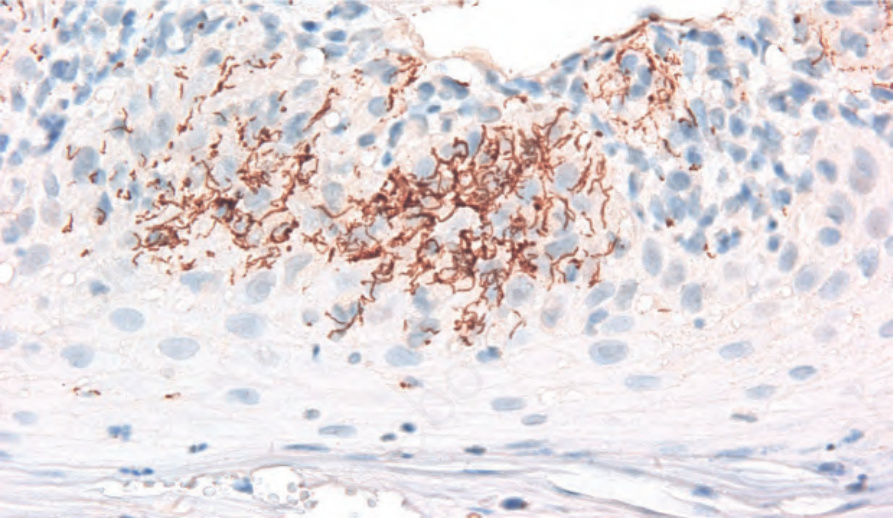
Fig. 12.125 Secondary syphilis: numerous spirochetes are seen by immunohistochemistry within the epidermis in a patient with secondary syphilis.
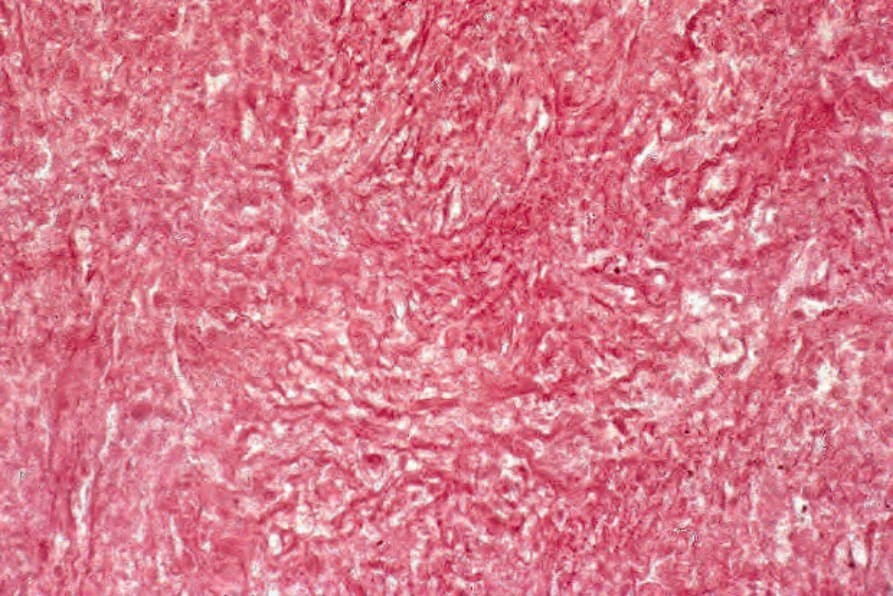
Fig. 12.126 Gumma: high-power view reveals ghost outlines of cells and connective tissue.