臨床特徵 (Clinical Features)
-
黑色棘皮病 (melanoacanthosis;口腔黑色棘皮瘤,oral melanoacanthoma) 不應與皮膚黑色棘皮瘤 (cutaneous melanoacanthoma) 混淆。
-
超過 70% 的病例發生於年輕黑人女性,且典型出現於易受外傷的部位,如頰黏膜 (buccal mucosa)、下唇、腭黏膜 (palatal mucosa) 與牙齦 (gingiva)。
-
這些斑 (macule) 表面略為粗糙,呈棕色、黑色或藍色 (Fig. 11.257)。病灶可能界線清楚或界線不清。
-
多數病灶為單發,但罕見病例為多灶性 (multifocal)。
-
僅 50% 的病例有外傷病史。
-
病灶可能在數週內快速生長至數公分大小,並於數月內完全消退。
-
口腔黑色素斑 (oral melanotic macule) 的特徵為上皮基底細胞層 (basal cell layer) 內黑色素 (melanin) 色素沉著增加,通常侷限於表皮突 (rete ridge) 尖端,黑色素細胞 (melanocyte) 無增生或僅有極輕微增生 (Fig. 11.255)。
-
固有層 (lamina propria) 內噬黑色素細胞 (melanophage) 數量增加、黑色素失禁 (melanin incontinence)、程度不一的淋巴球浸潤,以及擴張的微血管 (ectatic capillaries)。
-
可能伴隨輕度過度角化 (hyperkeratosis)、角化不全 (parakeratosis) 與棘層肥厚 (acanthosis),皆提示為反應性、發炎性病灶。
-
此類發現亦見於與界面口炎 (interface stomatitides)(如扁平苔癬,lichen planus)相關的發炎後色素過度沉著 (postinflammatory hypermelanosis) (Fig. 11.256)。
-
超微結構上,第 III 期與第 IV 期高度黑色素化的黑色素體 (melanosome) 聚集成複合體,分布於黑色素細胞、角質形成細胞 (keratinocyte) 與噬黑色素細胞內。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- 口腔黑色棘皮病 (oral melanoacanthosis) 很可能是發炎後色素過度沉著 (postinflammatory hypermelanosis) 的一種型態,由外傷引發,隨後的發炎導致樹突狀黑色素細胞 (dendritic melanocyte) 的反應性增生。
- 有輕度角化不全 (parakeratosis) 與棘層肥厚 (acanthosis),且通常有海綿水腫 (spongiosis) (Fig. 11.258)。
- 大量樹突狀黑色素細胞及其載有黑色素的突起,可見於穿插在角質形成細胞之間、貫穿整層上皮全層 (Fig. 11.259)。
- 此類黑色素細胞的遷移 (transmigration) 不應被過度診斷為黑色素瘤 (melanoma),因為並無細胞學異型性 (cytological atypia)。
- 固有層 (lamina propria) 內亦可見噬黑色素細胞、輕度淋巴球浸潤及血管擴張 (vascular ectasia)。
- 有時海綿水腫可能嚴重到形成海綿狀水泡 (spongiform vesicle)。
- S100 與 Melan-A 的檢查呈陽性。
鑑別診斷 (Differential Diagnosis)
- 吸菸者黑色素沉著 (smoker’s melanosis) 表現出相同的特徵,亦可能代表發炎後色素過度沉著 (postinflammatory hypermelanosis)。與⋯⋯相關的黑色素斑病例
- 黑色棘皮病 (melanoacanthosis) 與交界型黑色素細胞痣 (junctional melanocytic nevus) 的區別在於,前者在界面處缺乏黑色素細胞成巢 (nesting)。
- 黑色素細胞的良性細胞學特徵,使本病灶易於與口腔黑色素瘤 (oral melanoma) 區分,即使存在上皮內遷移 (epithelial transmigration)。
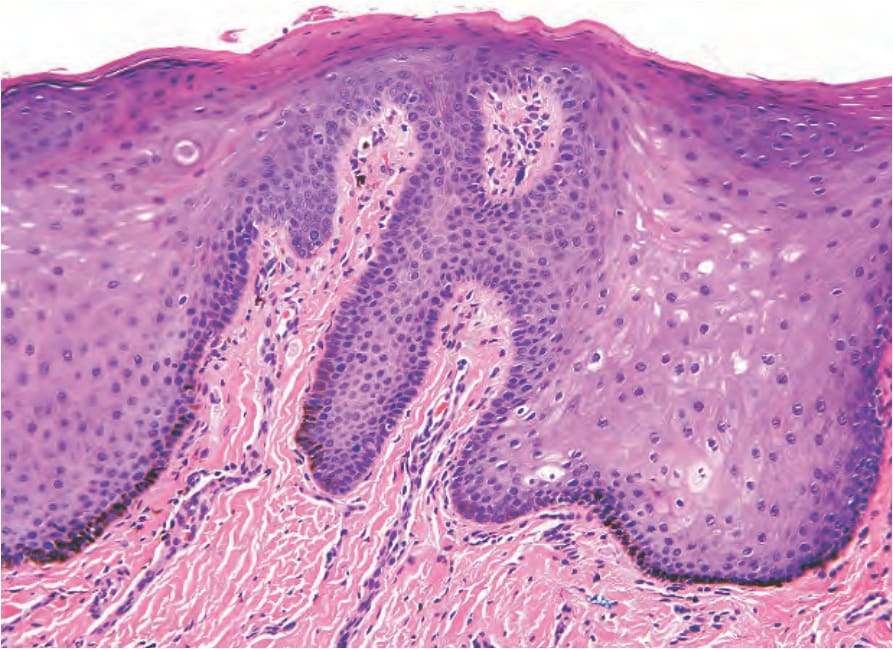
圖 11-255:口腔黑色素斑 (oral melanotic macule):基底細胞黑色素化增加而無黑色素細胞增生 (melanocytic hyperplasia);乳頭固有層 (papillary lamina propria) 內可見噬黑色素細胞 (melanophage)。
Fig. 11.255 Oral melanotic macule: there is increased melanization of the basal cells in the absence of melanocytic hyperplasia; melanophages are present in the papillary lamina propria.
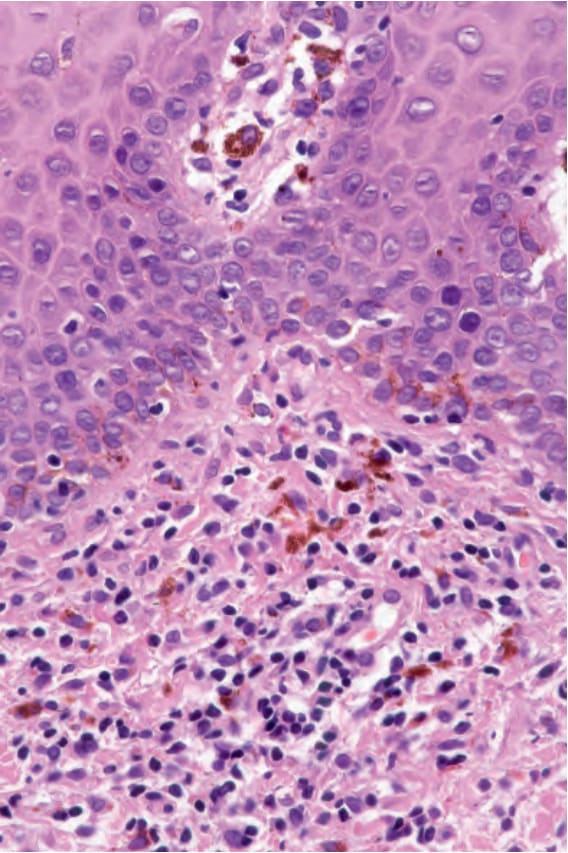
圖 11-256:發炎後色素過度沉著 (post-inflammatory hypermelanosis):基底細胞黑色素化增加、血管擴張 (vascular ectasia)、慢性發炎,固有層 (lamina propria) 內有許多噬黑色素細胞 (melanophage)。
Fig. 11.256 Post-inflammatory hypermelanosis: there is increased melanization of the basal cells, vascular ectasia, chronic inflammation, and many melanophages in the lamina propria.
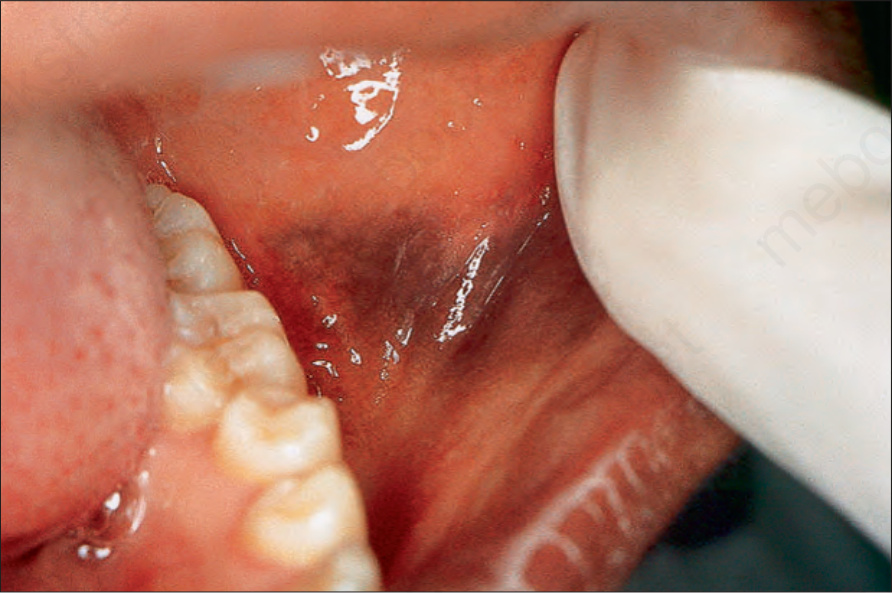
圖 11-257:黑色棘皮病 (melanoacanthosis):頰黏膜 (buccal mucosa) 上有一藍黑色斑,於數週內快速增大。
Fig. 11.257 Melanoacanthosis: there is a blue-black macule on the buccal mucosa that enlarged rapidly over a few weeks.
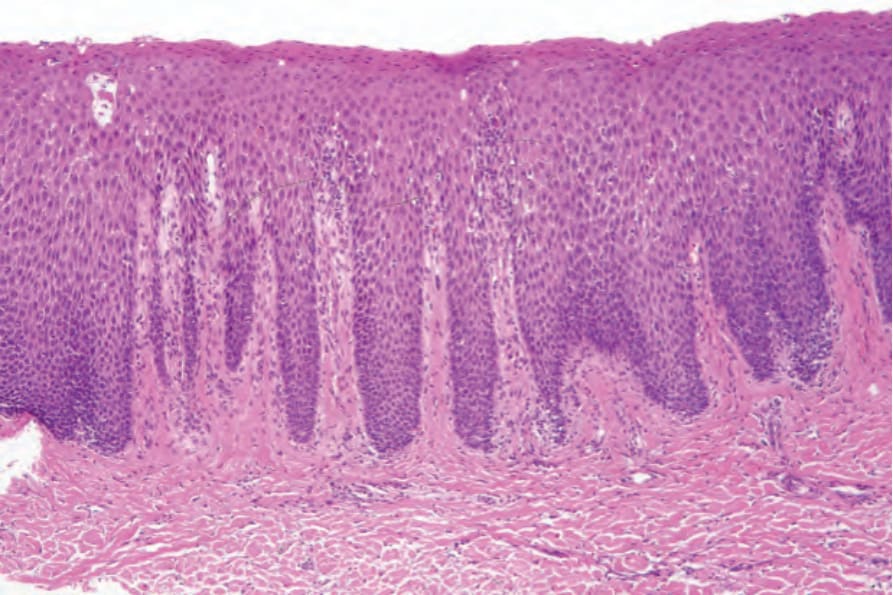
圖 11-258:黑色棘皮病 (melanoacanthosis):可見角化不全 (parakeratosis)、棘層肥厚 (acanthosis)、海綿水腫 (spongiosis),以及波及上皮全層的黑色素細胞增生 (melanocytic hyperplasia)。
Fig. 11.258 Melanoacanthosis: there is parakeratosis, acanthosis, spongiosis, and melanocytic hyperplasia involving the full thickness of the epithelium.
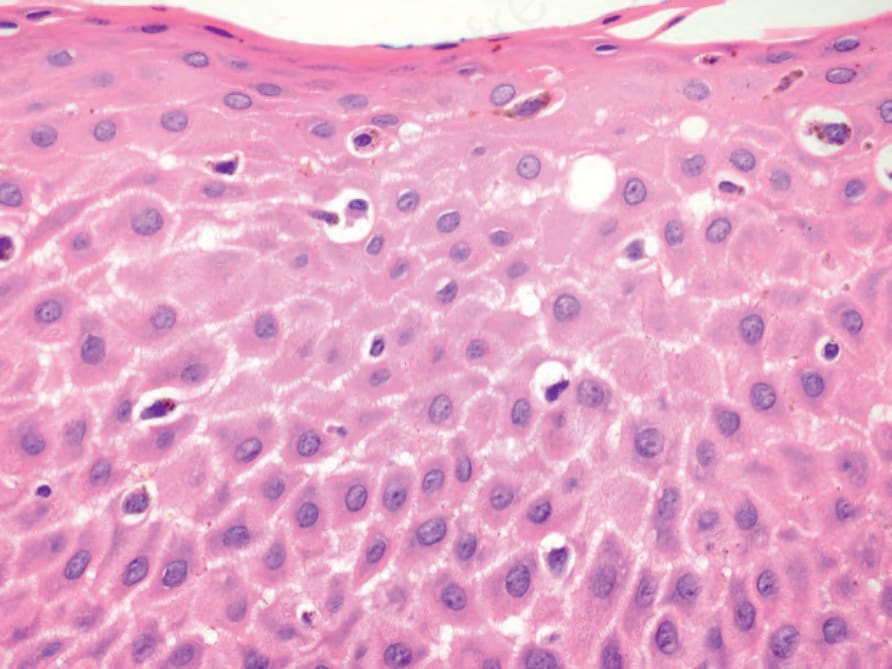
圖 11-259:黑色棘皮病 (melanoacanthosis):良性樹突狀黑色素細胞 (benign dendritic melanocytes) 遍布於上皮全層。
Fig. 11.259 Melanoacanthosis: benign dendritic melanocytes are present throughout the full thickness of the epithelium.
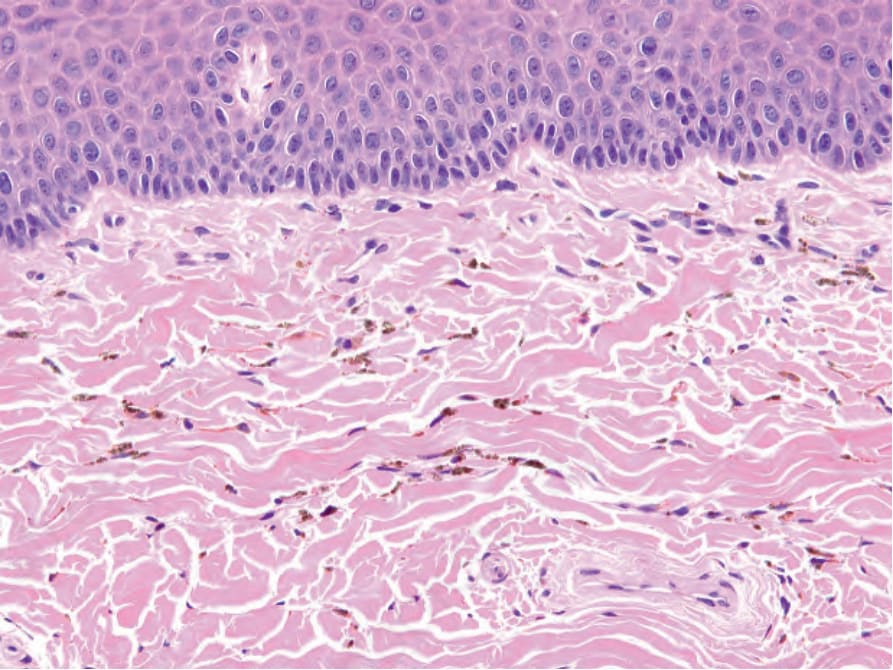
圖 11-260:Imatinib 引起的色素沉著 (imatinib-induced pigmentation):可見沿結締組織纖維排列的小型、球形、棕色色素顆粒。
Fig. 11.260 Imatinib-induced pigmentation: there are small, spherical, brown pigment granules disposed along connective tissue fibers.