Melanoacanthosis
Melanoacanthosis
Clinical features Melanoacanthosis (oral melanoacanthoma) should not be confused with cutaneous melanoacanthoma. More than 70% of cases occur in young black females, and it typically presents in areas that are susceptible to trauma such as the buccal mucosa, lower lip, palatal mucosa, and gingiva.1–5 The macules have a slightly rough surface and are brown, black, or bluish (Fig. 11.257). The lesion may be well or poorly demarcated. Most lesions are solitary although rare cases are multifocal.6 A history of trauma is present in only 50% of cases. Lesions may grow rapidly to several centimeters in size over a few weeks, and complete resolution occurs within months.
The oral melanotic macule is characterized by increased melanin pigmentation in the basal cell layer of the epithelium, usually localized to the tips of the rete ridges with no or only minimal melanocytic hyperplasia (Fig. 11.255).1,3,9,10 There are increased numbers of melanophages in the lamina propria, melanin incontinence, variable lymphocytic infiltrate, and ectatic capillaries. There may be associated mild hyperkeratosis, parakeratosis, and acanthosis, all suggestive of a reactive, inflammatory lesion. Such findings are also seen in postinflammatory hypermelanosis associated with interface stomatitides such as lichen planus (Fig. 11.256).
Ultrastructurally, stage III and stage IV heavily melanized melanosomes are clustered in complexes within melanocytes, keratinocytes, and melanophages.9
Differential diagnosis Smoker’s melanosis exhibit the same features and is also likely to represent postinflammatory hypermelanosis.11 Cases of melanotic macules associated
Pathogenesis and histologic features It is likely that oral melanoacanthosis is a form of postinflammatory hypermelanosis, precipitated by trauma with subsequent inflammation resulting in reactive hyperplasia of dendritic melanocytes.
There is slight parakeratosis and acanthosis and, usually, spongiosis (Fig. 11.258). Numerous dendritic melanocytes and their melanin-laden processes are found insinuating between keratinocytes throughout the full thickness of the epithelium (Fig. 11.259).1–7 Such transmigration of melanocytes should not be overdiagnosed as melanoma since there is no cytological atypia. Melanophages, a mild lymphocytic infiltrate, and vascular ectasia may also be seen in the lamina propria. Sometimes, the spongiosis may be so severe as to form spongiform vesicles.8 Studies for S100 and Melan-A are positive.3,9
466 Diseases of the oral mucosa
Differential diagnosis Melanoacanthosis differs from a junctional melanocytic nevus by the absence of nesting of melanocytes at the interface. The benign cytology of the melanocytes readily distinguishes this lesion from oral melanoma, even though there is epithelial transmigration.
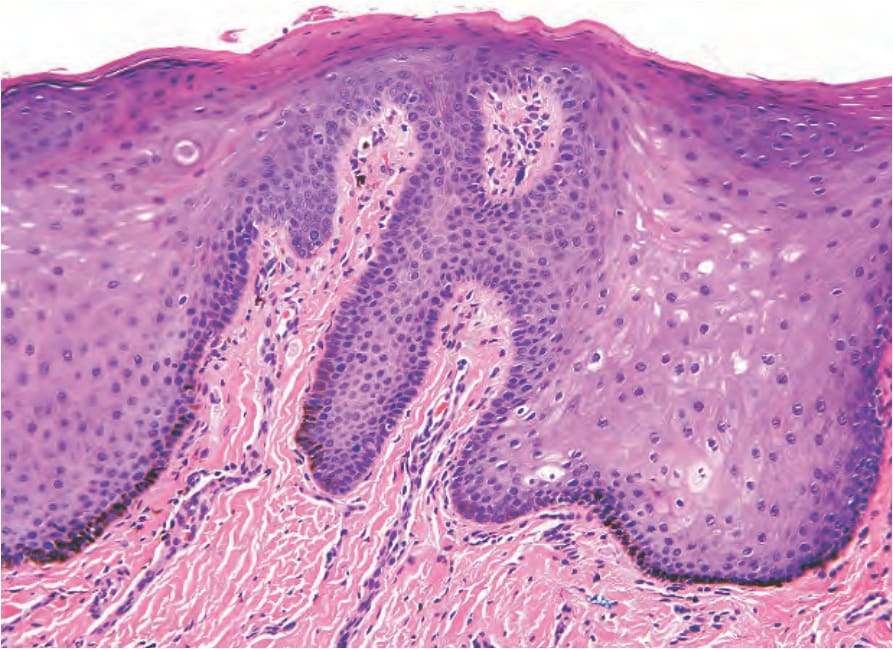
Fig. 11.255 Oral melanotic macule: there is increased melanization of the basal cells in the absence of melanocytic hyperplasia; melanophages are present in the papillary lamina propria.
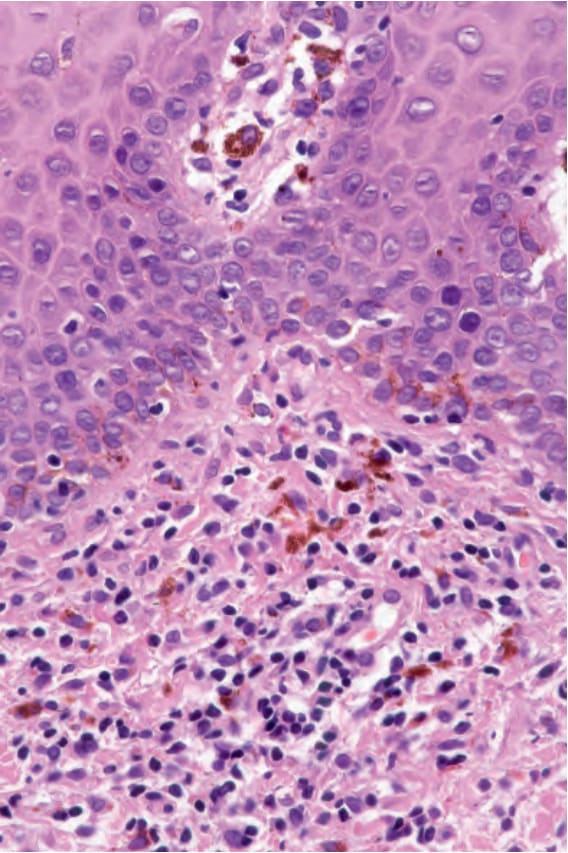
Fig. 11.256 Post-inflammatory hypermelanosis: there is increased melanization of the basal cells, vascular ectasia, chronic inflammation, and many melanophages in the lamina propria.
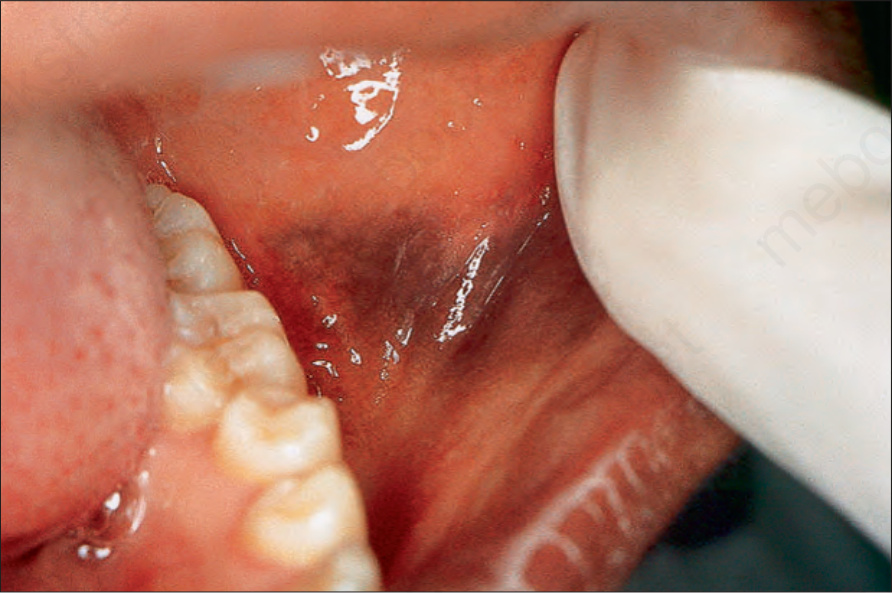
Fig. 11.257 Melanoacanthosis: there is a blue-black macule on the buccal mucosa that enlarged rapidly over a few weeks.
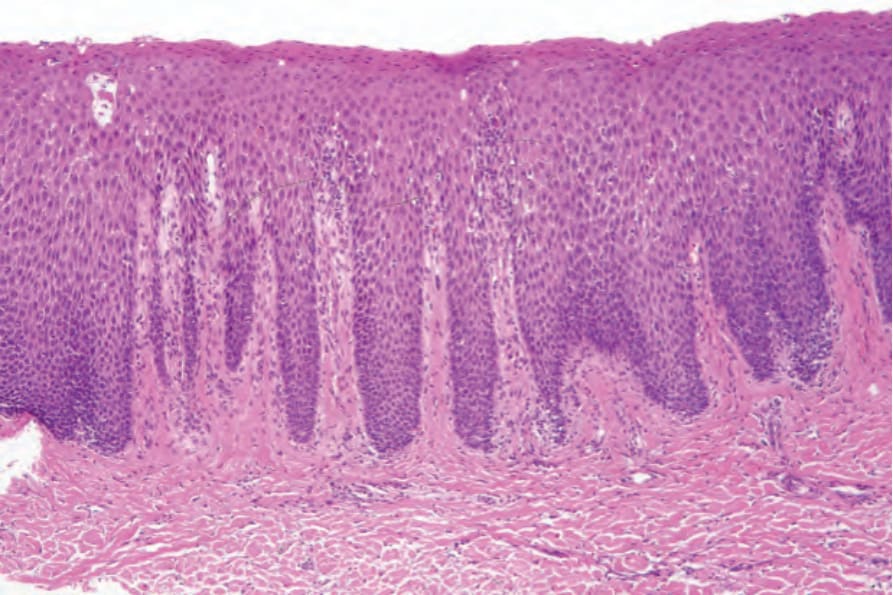
Fig. 11.258 Melanoacanthosis: there is parakeratosis, acanthosis, spongiosis, and melanocytic hyperplasia involving the full thickness of the epithelium.
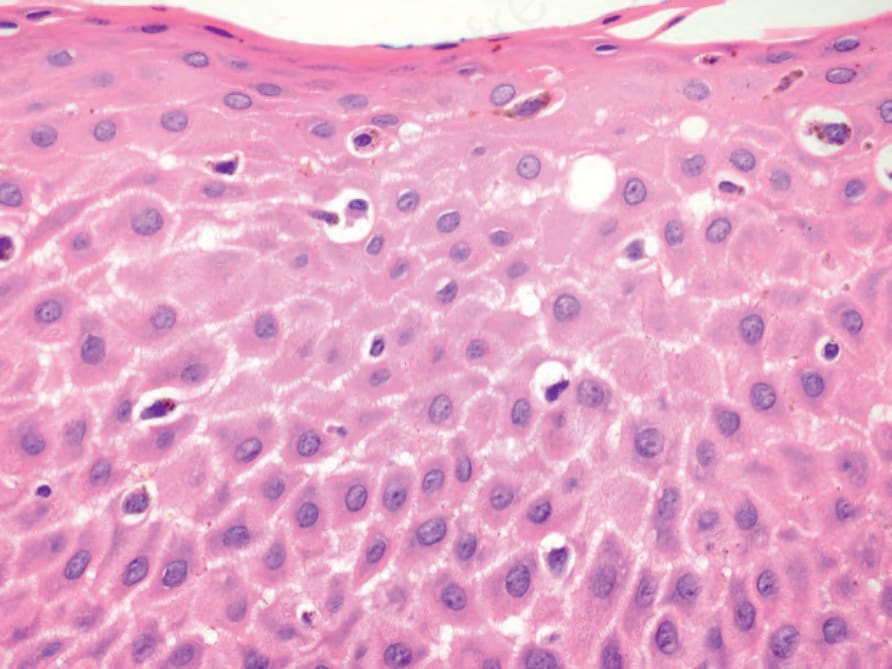
Fig. 11.259 Melanoacanthosis: benign dendritic melanocytes are present throughout the full thickness of the epithelium.
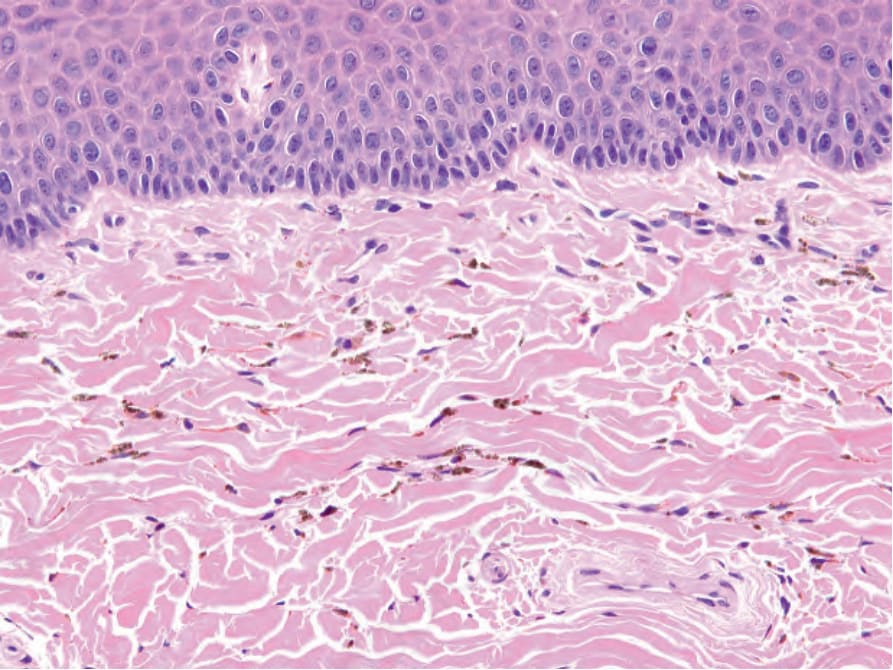
Fig. 11.260 Imatinib-induced pigmentation: there are small, spherical, brown pigment granules disposed along connective tissue fibers.