臨床特徵 (Clinical Features)
- 類風濕結節 (rheumatoid nodule) 為皮下病灶,發生於外傷部位或受壓點,約見於 30% 的類風濕性關節炎 (rheumatoid arthritis) 成人病人。
- 最常見於前臂與肘部 (尤其是鷹嘴突 olecranon process) 的伸側、足部、膝部、指關節 (knuckles)、臀部、頭皮與背部 (圖 9.67 與 9.68)。
- 亦曾描述侵犯多種其他部位,包括腹壁、心臟 (心包膜、心肌與瓣膜)、喉部、肺、胸膜、脾被膜 (splenic capsule)、腹膜、腸繫膜 (mesenterium)、眼、鼻樑、耳廓 (pinna)、坐骨結節 (ischial tuberosity)、甲狀舌骨膜 (thyrohyoid membrane)、跟腱 (Achilles tendon)、口腔黏膜、軟腦膜 (leptomeninges)、淋巴結、陰道、乳房與結膜。
組織病理特徵 (Histopathology)
- 類風濕結節 (rheumatoid nodule) 通常位於皮下脂肪或軟組織內,但可延伸至較深層的網狀真皮 (reticular dermis)。此與 granuloma annulare 及 necrobiosis lipoidica 兩者較表淺的位置形成對比。
- 病灶呈多結節性,伴有非常廣泛的壞死性膠原變性 (necrobiosis) (圖 9.69 與 9.70)。結節中央常見纖維蛋白 (fibrin) 沉積。亦可能出現免疫球蛋白、脂質、糖胺聚醣 (glycosaminoglycans) 與核蛋白 (nucleoproteins)。
- 陳舊性病灶有時因結節內容物之液化變性 (liquefactive degeneration) 而伴隨囊腫形成。
- 壞死性膠原變性病灶與纖維素樣物質 (fibrinoid material) 周圍特徵性地圍繞著發育良好的組織球柵欄狀排列 (palisade of histiocytes) 與偶見的巨細胞 (圖 9.71)。星狀包涵體 (asteroid inclusions) 並非其特徵。
- 外層由富含血管的肉芽組織 (vascular granulation tissue) 組成,陳舊性病灶常伴有明顯纖維化。常見由淋巴球、漿細胞與嗜酸性球組成的發炎細胞浸潤。早期結節內及其周圍的血管偶有報告受白血球破裂性血管炎 (leukocytoclastic vasculitis) 影響。曾有罕見病例記載伴有表皮穿孔。
致病機轉/分子 (Pathogenesis / Molecular)
- ⋯⋯與 IL-10。雖然以大範圍中央壞死為主,但整個結節內皆可見細胞凋亡 (apoptosis)。

圖 9.67:類風濕結節 (rheumatoid nodules):指關節 (knuckles) 上的病灶常見於類風濕性關節炎 (rheumatoid arthritis)。承蒙 Dr J.C. Pascual, MD, Alicante, Spain 提供。
Fig. 9.67 Rheumatoid nodules: lesions on the knuckles are commonly seen in rheumatoid arthritis. By courtesy of Dr J.C. Pascual, MD, Alicante, Spain.
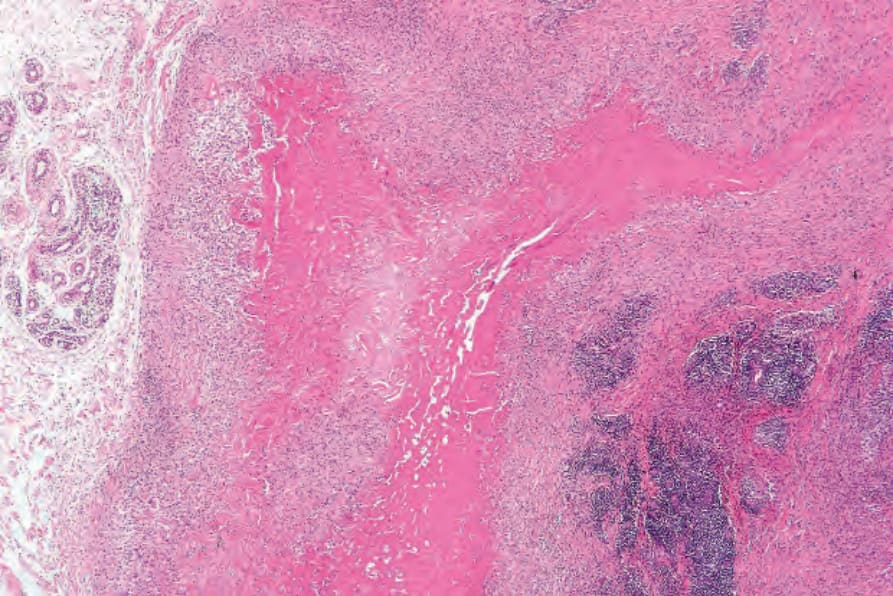
圖 9.69:類風濕結節 (rheumatoid nodule):可見大範圍壞死性膠原變性 (necrobiosis),鄰近處有瘢痕形成與緻密的淋巴球浸潤。類風濕結節特徵性地發生於軟組織。
Fig. 9.69 Rheumatoid nodule: there is massive necrobiosis with adjacent scarring and a dense lymphocytic infiltrate. Rheumatoid nodules characteristically occur in the soft tissues.
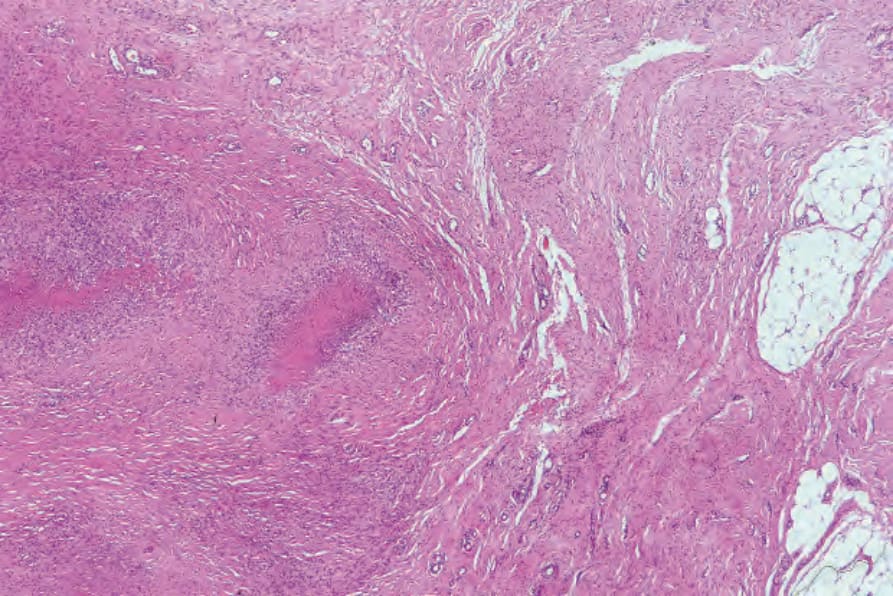
圖 9.70:類風濕結節 (rheumatoid nodule):本例中可在視野右側見到肌腱 (tendon)。
Fig. 9.70 Rheumatoid nodule: in this example, tendon can be seen on the right side of the field.
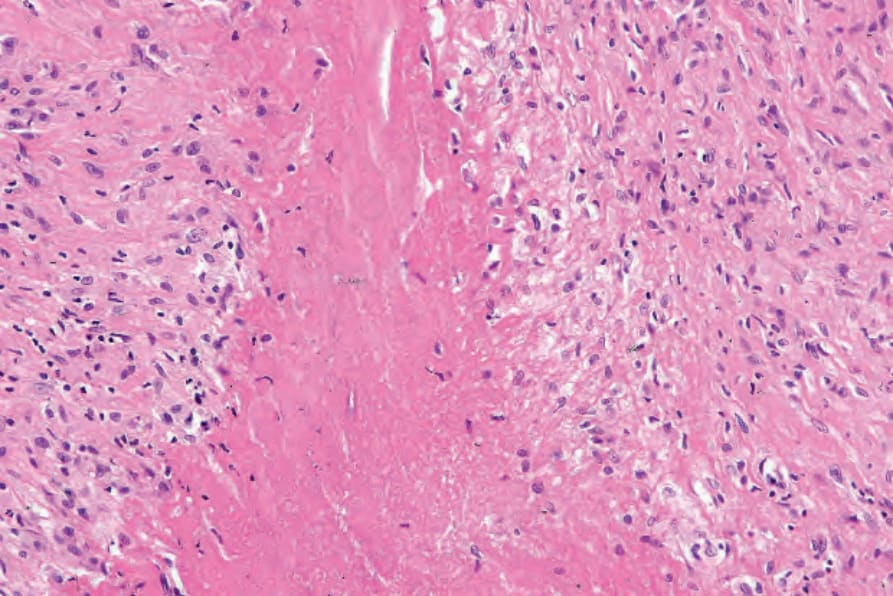
圖 9.71:類風濕結節 (rheumatoid nodule):壞死性膠原變性的結締組織 (necrobiotic connective tissue) 周圍圍繞著發育良好的組織球柵欄狀排列 (histiocytic palisade)。
Fig. 9.71 Rheumatoid nodule: the necrobiotic connective tissue is surrounded by a welldeveloped histiocytic palisade.
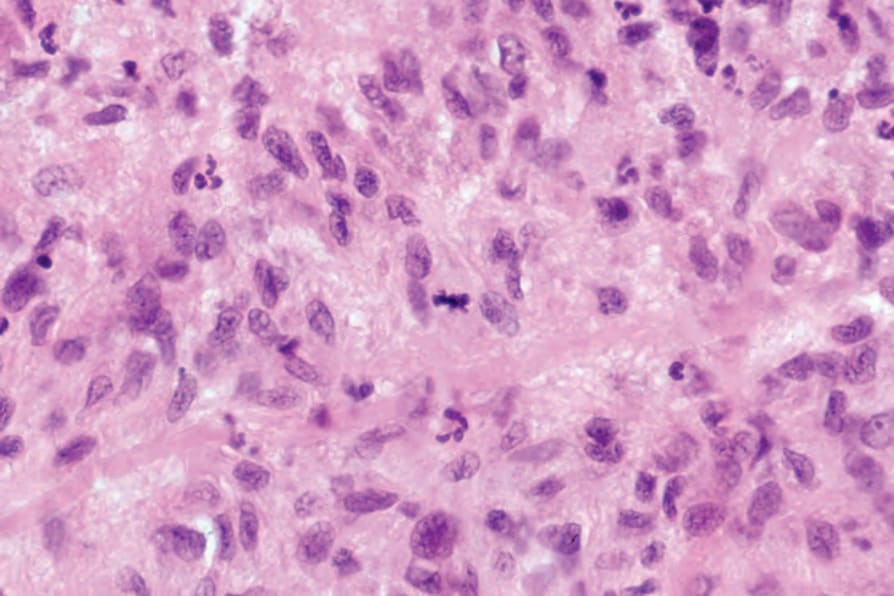
圖 9.72:類風濕結節 (rheumatoid nodule):柵欄狀排列的組織球 (palisading histiocytes) 有時可顯現有絲分裂象 (mitotic figures),可能使不慎者誤判為上皮樣肉瘤 (epithelioid sarcoma)。
Fig. 9.72 Rheumatoid nodule: the palisading histiocytes may sometimes show mitotic figures which may lead the unwary to consider epithelioid sarcoma.
鑑別診斷 (Differential Diagnosis)
- 在某些深部 granuloma annulare 的病例中,組織學變化與類風濕結節 (rheumatoid nodule) 相似。深部 granuloma annulare (「假類風濕結節」pseudorheumatoid nodule) 傾向於有較多黏液素 (mucin) 沉積,而纖維蛋白 (fibrin) 較典型類風濕結節為少。因此,後者被稱為「紅色」肉芽腫,而前者被稱為「藍色」肉芽腫。然而,部分類風濕結節確實含有黏液素 (mucin)。在確立明確診斷之前,建議進行臨床病理與血清學的相互對照。
- 與風濕熱結節 (rheumatic fever nodule) 相比,類風濕性關節炎 (rheumatoid arthritis) 結節傾向於界限較清楚,並由界線分明的組織球柵欄狀排列 (palisade of histiocytes) 所圍繞。此外,構成風濕熱結節中央的細小纖維素樣條索 (fibrinoid strands),與類風濕性關節炎結節中較緻密、片狀的壞死性膠原變性 (necrobiosis) 與纖維蛋白沉積區域形成對比。
- 曾有報告描述兼具嚴重類風濕性關節炎 (rheumatoid arthritis) 與柵欄狀肉芽腫 (palisading granulomata) 特徵、並伴有嗜中性球浸潤與白血球破裂性血管炎 (leukocytoclastic vasculitis) 的病人。這些病灶歸於「伴血管炎之柵欄狀嗜中性球與肉芽腫性皮膚炎 (palisaded neutrophilic and granulomatous dermatitis with vasculitis)」此名目下討論。簡言之,呈現這些特徵的病灶可能與多種全身性疾病相關,包括類風濕性關節炎。
- 雖然上皮樣肉瘤 (epithelioid sarcoma) 及其伴隨的地圖樣壞死 (geographic necrosis) 在低倍下可能與類風濕結節 (rheumatoid nodule) 有表淺的相似之處,但前者的核異型性 (nuclear atypia) 與多形性 (pleomorphism) 程度應能讓這兩種病況容易區分 (圖 9.72)。然而,在困難的病例中,上皮樣肉瘤中 keratin 與上皮膜抗原 (epithelial membrane antigen) 的表現,以及 INI-1 表現的喪失,應有助於鑑別診斷。