Rheumatoid nodule
Rheumatoid nodule
Clinical features Rheumatoid nodules are subcutaneous lesions that develop at sites of trauma or at pressure points in approximately 30% of adults with rheumatoid arthritis.1–4 They are most commonly found on the extensor aspect of the forearms and elbows (particularly the olecranon process), the feet, knees, knuckles, buttocks, scalp, and back (Figs 9.67 and 9.68).5 They have also been described involving a wide variety of other sites, including the abdominal wall, heart (pericardium, myocardium, and valves), larynx, lungs, pleura, splenic capsule, peritoneum, mesenterium, eye, bridge of nose, pinna, ischial tuberosity, thyrohyoid membrane, Achilles tendon, oral mucosa, leptomeninges, lymph nodes, vagina, breast, and conjunctiva.6–14
327 Elastolytic granulomata
Differential diagnosis In some cases of deep granuloma annulare, the histologic changes are similar to rheumatoid nodule. Deep granuloma annulare (‘pseudorheumatoid nodule’) tends to have more mucin deposition and less fibrin than typical rheumatoid nodules.37 Therefore, the latter are referred to as ‘red’ granulomas and the former as ‘blue’ granulomas.38 However, some rheumatoid nodules do contain mucin. Clinicopathological and serological correlation is advised before establishing a definitive diagnosis.
Compared to rheumatoid fever nodule, rheumatoid arthritis nodules tend to be better circumscribed and surrounded by a well-defined palisade of histiocytes. In addition, the fine fibrinoid strands that form the center of a rheumatic fever nodule contrast with the more dense sheetlike areas of necrobiosis and fibrin deposition in the rheumatoid arthritis nodule.
and IL-10.32 Although massive central necrosis is predominant, apoptosis has been demonstrated throughout the nodule.34
Patients combining the features of severe rheumatoid arthritis with palisading granulomata accompanied by a neutrophilic infiltrate and leukocytoclastic vasculitis have been described.18 These lesions are discussed under the rubric of palisaded neutrophilic and granulomatous dermatitis with vasculitis. In short, lesions showing these features may be associated with a number of systemic diseases, including rheumatoid arthritis.
Although epithelioid sarcoma, with its associated geographic necrosis, may bear a superficial resemblance at low power to rheumatoid nodule, the degree of nuclear atypia and pleomorphism in the former should allow easy distinction between these conditions (Fig. 9.72). However, in difficult cases, expression of keratin and epithelial membrane antigen and loss of INI-1 expression in epithelioid sarcoma should assist in the differential diagnosis.39
Rheumatoid nodules are typically located in the subcutaneous fat or soft tissues although they may extend into the deeper reticular dermis. This is in contrast to the more superficial location of both granuloma annulare and necrobiosis lipoidica. They are multinodular and associated with very extensive necrobiosis (Figs 9.69 and 9.70). Fibrin deposition is often seen in the center of the nodule.35 Immunoglobulin, lipid, glycosaminoglycans, and nucleoproteins may also be present. Old lesions are sometimes associated with cyst formation due to liquefactive degeneration of the contents of the nodules. A well-developed palisade of histiocytes and occasional giant cells characteristically surrounds necrobiotic foci and fibrinoid material (Fig. 9.71). Asteroid inclusions are not a feature. The outer layer is composed of vascular granulation tissue, and in older lesions marked fibrosis is a frequent accompaniment. An inflammatory cell infiltrate of lymphocytes, plasma cells, and eosinophils is often present. Leukocytoclastic vasculitis has occasionally been reported to affect the blood vessels in and around early nodules. A rare case with perforation of the epidermis has been documented.36

Fig. 9.67 Rheumatoid nodules: lesions on the knuckles are commonly seen in rheumatoid arthritis. By courtesy of Dr J.C. Pascual, MD, Alicante, Spain.
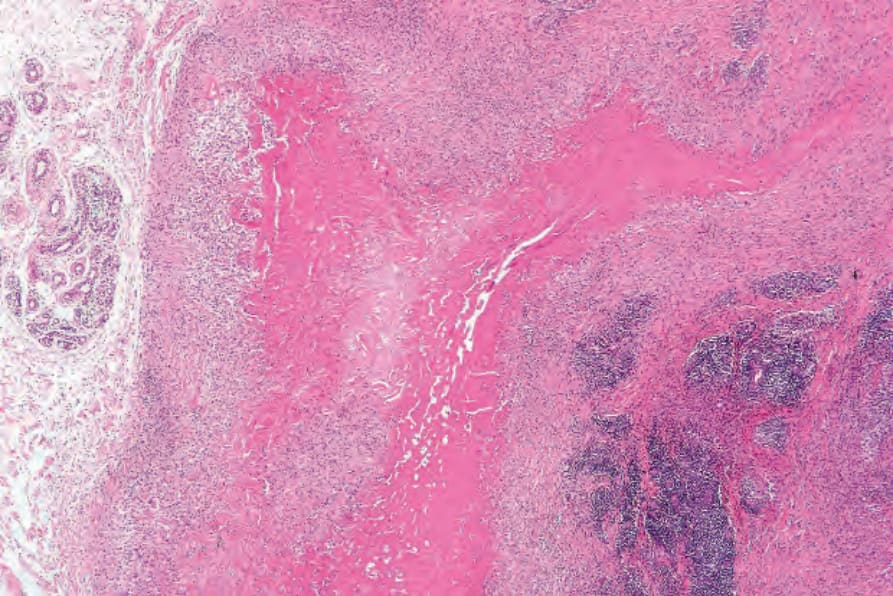
Fig. 9.69 Rheumatoid nodule: there is massive necrobiosis with adjacent scarring and a dense lymphocytic infiltrate. Rheumatoid nodules characteristically occur in the soft tissues.
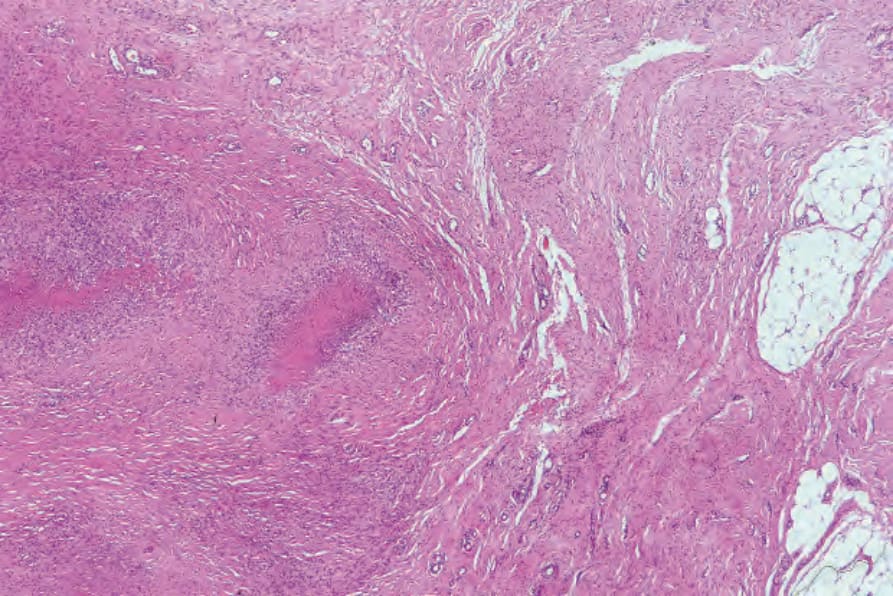
Fig. 9.70 Rheumatoid nodule: in this example, tendon can be seen on the right side of the field.
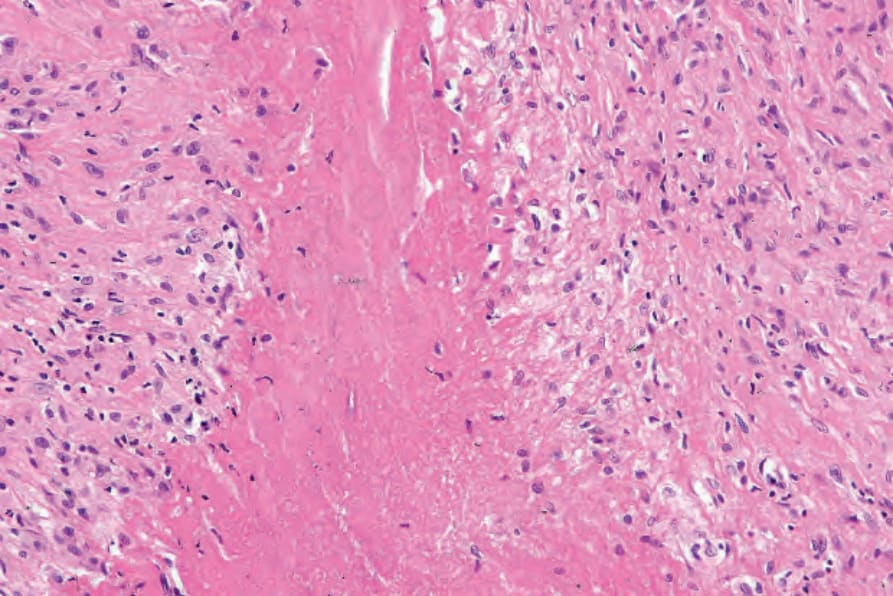
Fig. 9.71 Rheumatoid nodule: the necrobiotic connective tissue is surrounded by a welldeveloped histiocytic palisade.
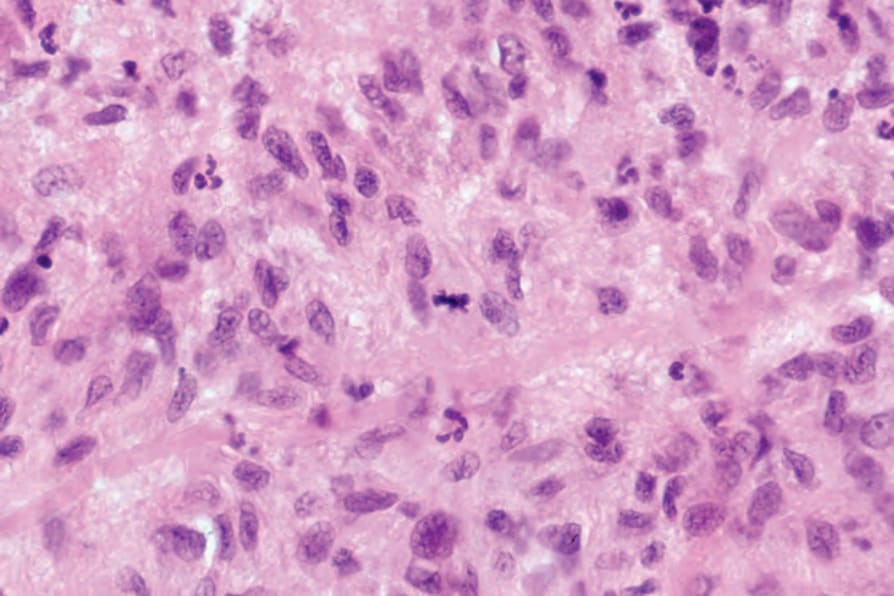
Fig. 9.72 Rheumatoid nodule: the palisading histiocytes may sometimes show mitotic figures which may lead the unwary to consider epithelioid sarcoma.