環狀肉芽腫 (Granuloma annulare)
Granuloma annulare
臨床特徵 (Clinical Features)
環狀肉芽腫 (granuloma annulare) 是一種常見、通常無症狀、病因不明的皮膚病。它可分為六種臨床亞型:
- 局限型 (localized),
- 泛發型 (generalized),
- 穿透型 (perforating),
- 皮下型 (subcutaneous),
- 丘疹型 (papular),
- 線狀型 (linear)。
不尋常的臨床變異型包括膿疱性毛囊病灶 (pustular follicular lesions) 以及以斑片 (patches) 表現者。曾有單一以接觸性皮膚炎 (contact dermatitis) 表現的病例報告。Granuloma annulare(常為廣泛散在分布之病灶)曾於 HIV 感染病人中被描述,有時甚至可能是其首發徵象。Granuloma annulare,主要為泛發型變異型(見下文),亦曾被報告與 Hodgkin 與非 Hodgkin 淋巴瘤 (lymphoma) 有關。極罕見地,曾有前葡萄膜炎 (anterior uveitis) 與並發皮膚病灶的描述。亦曾有口腔 granuloma annulare 的病例報告。
Granuloma annulare 其他已記載的關聯包括 morphea、慢性 C 型肝炎 (chronic hepatitis C) 感染、自體免疫甲狀腺炎 (autoimmune thyroiditis)、次發性副甲狀腺機能亢進 (secondary hyperparathyroidism)、sarcoidosis、Plummer disease、骨髓增生不良症候群 (myelodysplastic syndrome)、轉移性癌 (metastatic carcinoma),以及一例蜜蜂螫傷 (bee sting)。Granuloma annulare 亦曾於破傷風與白喉、B 型肝炎、結核 (BCG) 疫苗接種後,以及美塑療法 (mesotherapy) 後被描述。它亦可能在帶狀疱疹 (herpes zoster) 的瘢痕中發生。值得強調的是,大多數患此病的病人在經過不一的時間後會痊癒,長期追蹤並未發現與任何全身性疾病有一致的關聯。一項進一步的研究發現惡性腫瘤 (malignant neoplasms) 與 granuloma annulare 之間並無一致的關係。然而,有人建議,對於病灶不具典型 granuloma annulare 特徵、但顯微鏡下表現類似 granuloma annulare 的老年病人,應檢查是否有潛在的惡性腫瘤,尤其是淋巴瘤 (lymphoma)。
[註:以下兩段為原文中混入之 sarcoidosis 內容,依鐵則 1:1 鏡射原文、不刪除、不重排]
對 sarcoidosis 的診斷而言,事實上,在高達 5% 的病例中曾發現可偏光物質 (polarizable material)。
已顯示 gli-1 致癌基因 (oncogene) 不僅在 sarcoidosis,也在 granuloma annulare 與類脂質漸進性壞死 (necrobiosis lipoidica) 中,於構成肉芽腫的細胞內持續且異常地表現。此觀察提出了使用 gli-1 訊息傳遞抑制劑來治療此類肉芽腫性疾病之試驗的可能性。
內臟病灶的特徵為相同的非乾酪化肉芽腫 (noncaseating granulomata) 組織學,可能伴隨顯著的瘢痕形成,例如在肺部,晚期病例的特徵為間質性纖維化 (interstitial fibrosis),有時形成蜂窩肺 (honeycomb lung)。在肝臟,肉芽腫最常見於門脈束 (portal tracts) 或與中央靜脈 (central veins) 有關之處。脾臟病灶呈隨機分布,通常不伴隨顯著的纖維化。
[註:以下回到 granuloma annulare 內容]
Granuloma annulare 曾於使用 allopurinol、amlodipine、daclizumab、抗腫瘤壞死因子製劑 (antitumor necrosis factor agents)、thalidomide、vemurafenib、pegylated interferon alpha 與 topiramate 治療期間發生。Interferon-alpha 曾與泛發性間質性 granuloma annulare 有關。然而,最有可能的是,繼發於藥物投予的 granuloma annulare 樣疹 (granuloma annulare-like eruptions) 往往代表間質性肉芽腫性藥物疹 (interstitial granulomatous drug eruptions)。
[註:以下段落為原文混入之 sarcoidosis 鑑別診斷內容,依鐵則保留]
鑑別診斷 (Differential Diagnosis)
Sarcoidosis 必須以排除性診斷 (diagnosis of exclusion) 來看待,並必須與許多可能伴隨非乾酪化肉芽腫組織學的疾病區分,包括某些形式的結核 (tuberculosis)、類結核型麻風 (tuberculoid leprosy)、鈹中毒 (berylliosis)、真菌感染、Crohn disease,以及異物肉芽腫反應 (foreign body granulomatous reactions)。因此,在診斷 sarcoidosis 之前,使用特殊染色(包括用於分枝桿菌的 Ziehl-Neelsen 製備,以及用於真菌的過碘酸-Schiff (PAS) 與 methenamine silver 反應)是強制必要的。視臨床情境而定,亦可能需要培養以排除感染性病因。類結核型麻風的特徵為神經侵犯,此特徵在 sarcoidosis 中通常不存在。
[註:以下回到 granuloma annulare 各臨床亞型內容]
局限型 granuloma annulare (Localized granuloma annulare)
局限型變異型是最常見的類型。它通常出現於前三個十年 (first three decades),且有女性偏多的傾向 (2.25:1)。病灶由一個或數個丘疹組成,可能為膚色、紅色或紫色 (violaceous),典型上呈環狀或弧形分布,直徑 1–5 cm(圖 9.23–9.27)。約 50% 的病人為單一病灶。肢端部位 (acral sites) 最常受侵犯,尤其是指關節 (knuckles) 與手指背側。在小部分病人中,病灶同時出現於上肢與下肢,偶爾軀幹亦受侵犯。手掌病灶極為罕見。臉部侵犯似乎不常見。在一報告病例中,病灶侷限於 Becker nevus 所涉及的區域。雖然病灶可能持續存在,但約 50% 的病人可預期在發病約 2 年後消退。然而,不幸地,復發相當常見。在生命較早期發病的病人,病灶似乎較早消退。有趣的是,病灶偶爾會在切片後自發性消退。自發性消退罕見地可能導致真皮中層彈性溶解 (mid-dermal elastolysis)。罕見地,granuloma annulare 曾於家族與同卵雙胞胎 (monozygotic twins) 中被報告。曾有一病例記載病灶在曝曬陽光區域呈季節性復發。僅有單一病例報告描述皮膚 granuloma annulare 合併腹腔內 (intra-abdominal) 位置出現類似病灶。在一病例中,granuloma annulare 為成人 T 細胞白血病/淋巴瘤 (adult T-cell leukemia/lymphoma) 的首發徵象;在另一病人中與血管免疫母細胞性 T 細胞淋巴瘤 (angioimmunoblastic T-cell lymphoma) 有關;在再一位病人中,
[註:以下段落為原文混入之 sarcoidosis 鑑別診斷內容,依鐵則保留]
在各種原發性免疫缺陷症候群 (primary immunodeficiency syndromes) 中所見的部分肉芽腫,與 sarcoidosis 所見者極為相似,組織學上的區分可能不可能。一項比較 sarcoidosis 肉芽腫與原發性免疫缺陷所見肉芽腫的研究發現,前者的 CD4+/CD8+ 細胞比率遠低於後者。
唇與牙齦侵犯在組織學上可能被誤認為 Crohn disease 與肉芽腫性唇炎 (granulomatous cheilitis, Miescher)。值得注意的是,罕見情況下 Crohn disease 的口腔侵犯可能比全身性表現早數年出現。轉移性 Crohn disease (Metastatic Crohn disease) 可能難以與 sarcoidosis 區分。前者常顯示瀰漫性分布的非化膿性肉芽腫 (nonsuppurative granulomata),周圍環繞一薄層淋巴球套 (cuff of lymphocytes)。其他常見的發現包括出現大量嗜伊紅性球 (eosinophils) 與潰瘍 (ulceration),此等發現在 sarcoidosis 中不常見。
在外源性褐黃病 (exogenous ochronosis) 中所描述的肉芽腫病灶似乎與 sarcoidosis 有關。然而,類似病灶亦曾被描述為顯示類似日光性肉芽腫 (actinic granuloma) 的變化。
[註:以下回到 granuloma annulare 內容]
與皮膚邊緣區淋巴瘤 (cutaneous marginal zone lymphoma) 有關。極罕見地,肢端、局限型 granuloma annulare 可能以急性且疼痛的疹子表現。與陰莖硬化性苔癬 (penile lichen sclerosus) 的關聯極為罕見。
[註:以下段落於原文中接續泛發型內容]
可能無症狀或搔癢。如同局限型,此病為持續性,但部分病人在 4 年內消退。皮膚鬆弛症 (Anetoderma) 曾極罕見地被報告為泛發型 granuloma annulare 的併發症。曾有報告與巨細胞動脈炎 (giant cell arteritis)、胃腸道間質瘤 (gastrointestinal stromal tumor),以及其他內臟惡性腫瘤(包括卵巢癌與胃癌)有顯著關聯。在一病例中,結核性淋巴結炎 (tuberculous lymphadenitis) 為其關聯。在兩個案例中,此病為慢性骨髓單核球性白血病 (chronic myelomonocytic leukemia) 的初始表現。亦曾描述與淋巴瘤(包括 Hodgkin disease)有關。一位 B 型肝炎病人發生泛發型 granuloma annulare,並以 PCR 在皮膚病灶中偵測到病毒 DNA。另一病例以光敏感分布 (photosensitive distribution) 表現,並以瘢痕與粟粒疹 (milia) 形成而癒合。其他罕見關聯包括高脂血症 (hyperlipidemia) 與疥瘡 (scabies)。
泛發型 granuloma annulare (Generalized granuloma annulare)
泛發型病灶發生於約 15% 的 granuloma annulare 病人。如同局限型,女性發生率較高;然而,中位年齡不同,大多數病例發生於第四至第七個十年的病人,其餘出現於第一個十年。泛發型 granuloma annulare 的病人 HLA-Bw35 發生率較高。泛發型 granuloma annulare 定義為至少出現於軀幹以及上肢或下肢其一、或兩者皆有的病灶。大多數病灶為丘疹,可能呈環狀分布,但亦發生斑丘疹 (maculopapules) 與結節 (nodules)。其色調從膚色或紅色,到棕褐色、褐色或黃色不等。數目從數十個到數百個不等(圖 9.28–9.30)。曾記載單一病人有泛發性疾病並伴隨手部顯著腫脹,另一病人在多形性紅斑 (erythema multiforme) 之後發生此病。另一病例在水痘帶狀疱疹 (varicella zoster) 感染後發生。病灶
穿透型 granuloma annulare (Perforating granuloma annulare)
穿透型 granuloma annulare 的特徵為出現壞死性膠原蛋白 (necrobiotic collagen) 的經表皮排除 (transepidermal elimination)。臨床上,病灶表現為一群帶有臍狀痂皮 (umbilicated crust) 的丘疹,通常位於四肢,常為手背(圖 9.31)。
病灶出現於耳部的表現極罕見地曾被描述,泛發型變異型亦然。它可侵犯兒童與成人,且存在局限型與泛發型兩種形式。自發性消退有時在發病後數月或數年內發生。極罕見地,穿透型 granuloma annulare 在刺青 (tattooing) 後發生。
皮下(深部)granuloma annulare (Subcutaneous (deep) granuloma annulare)
皮下型變異型與兒童期假類風濕結節 (pseudorheumatoid nodule of childhood) 及深部 granuloma annulare 同義。病灶可能新發 (de novo),或與典型的皮膚丘疹相伴出現。約四分之一的病人同時有真皮 granuloma annulare 共存。它發生於兒童期,常侵犯下方的骨膜 (periosteum),並主要侵犯小腿(特別是脛骨 tibia)、足部、臀部、手部與頭部。病灶亦可能出現於陰莖或眼瞼。曾報告一極罕見病例,多個病灶侷限於一兒童的頭皮並自發性消退。另一病人以眶周骨膜下 (periorbital subperiostal) 病灶表現,另一病人的病灶為先天性。在一項 47 位病人的研究中,平均年齡為 4.3 歲。在某些情況下有外傷史。依定義,此類兒童並無類風濕性關節炎 (rheumatoid arthritis) 或風濕熱 (rheumatic fever)。此病灶
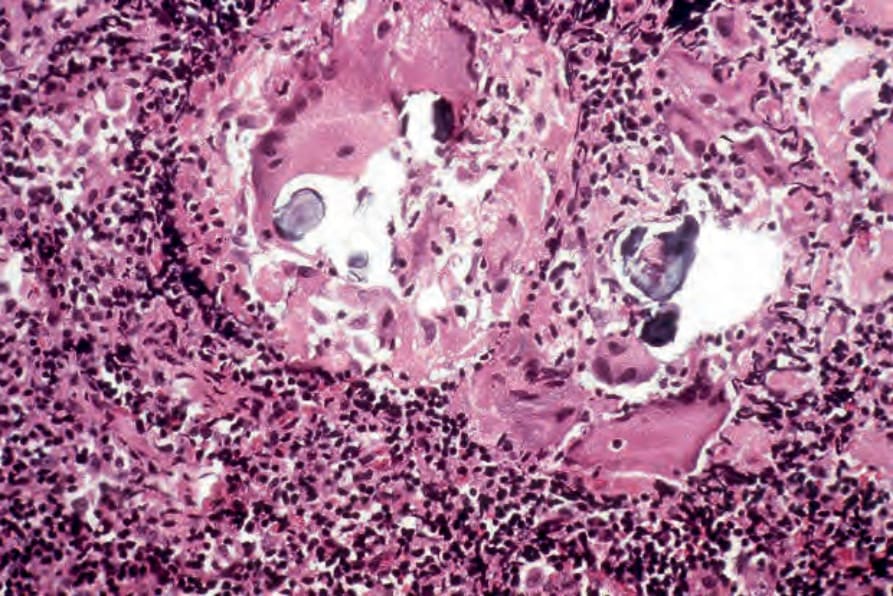
圖 9-22:Sarcoidosis:在此淋巴結切片標本中,可見破碎、層狀的 Schaumann bodies。它們極少是皮膚 sarcoidosis 的特徵。
Fig. 9.22 Sarcoidosis: in this lymph node biopsy specimen, fragmented, laminated Schaumann bodies are seen. They are very rarely a feature of cutaneous sarcoidosis.

圖 9-23:局限型 granuloma annulare:指關節上典型的環狀病灶。拉撐皮膚可顯露出半透明的串珠狀邊緣 (translucent beaded margin)。承蒙 R.A. Marsden, MD, St George’s Hospital, London, UK 提供。
Fig. 9.23 Localized granuloma annulare: a typical annular lesion over the knuckle. Stretching of the skin reveals a translucent beaded margin. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 9-24:局限型 granuloma annulare:在此病人中,足部出現多個病灶。取自已故 N.P. Smith, MD, the Institute of Dermatology, London, UK 的收藏。
Fig. 9.24 Localized granuloma annulare: in this patient, multiple lesions are present on the feet. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 9-25:局限型 granuloma annulare:此手臂病灶顯示特徵性的串珠狀邊緣 (beaded margin)。取自已故 N.P. Smith, MD, the Institute of Dermatology, London, UK 的收藏。
Fig. 9.25 Localized granuloma annulare: this arm lesion shows a characteristic beaded margin. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 9-26:局限型 granuloma annulare:環狀病灶之近觀。承蒙 the Institute of Dermatology, London, UK 提供。
Fig. 9.26 Localized granuloma annulare: close-up view of annular lesions. By courtesy of the Institute of Dermatology, London, UK.

圖 9-27:局限型 granuloma annulare:在此病人中,踝部有一大斑塊,並隱約可見中央清除 (central clearing)。承蒙 the Institute of Dermatology, London, UK 提供。
Fig. 9.27 Localized granuloma annulare: in this patient, there is a large plaque on the ankle with a hint of central clearing. By courtesy of the Institute of Dermatology, London, UK.
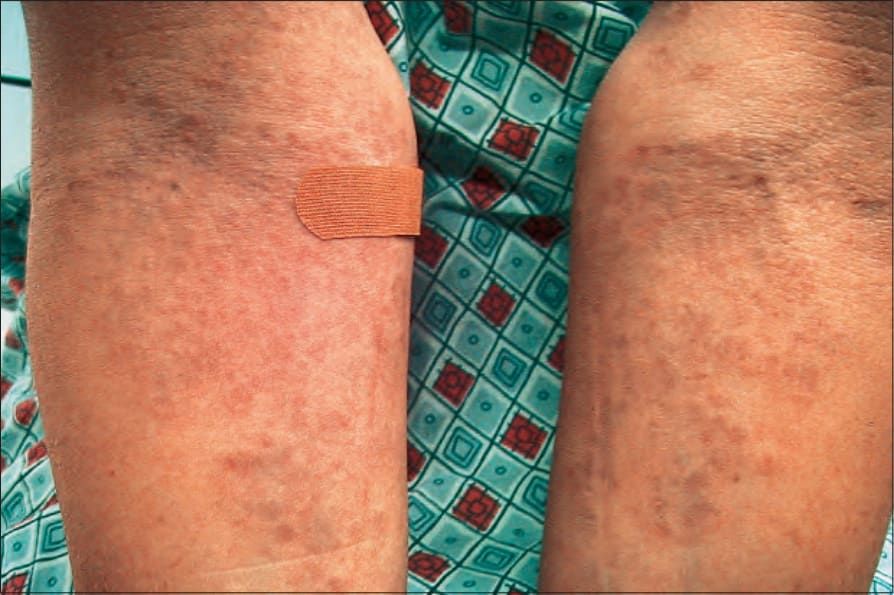
圖 9-28:泛發型 granuloma annulare:此病人手臂上出現無數丘疹。承蒙 J. Williams, MD, Brigham and Women’s Hospital, Boston, USA 提供。
Fig. 9.28 Generalized granuloma annulare: innumerable papules are present on this patient’s arms. By courtesy of J. Williams, MD, Brigham and Women’s Hospital, Boston, USA.
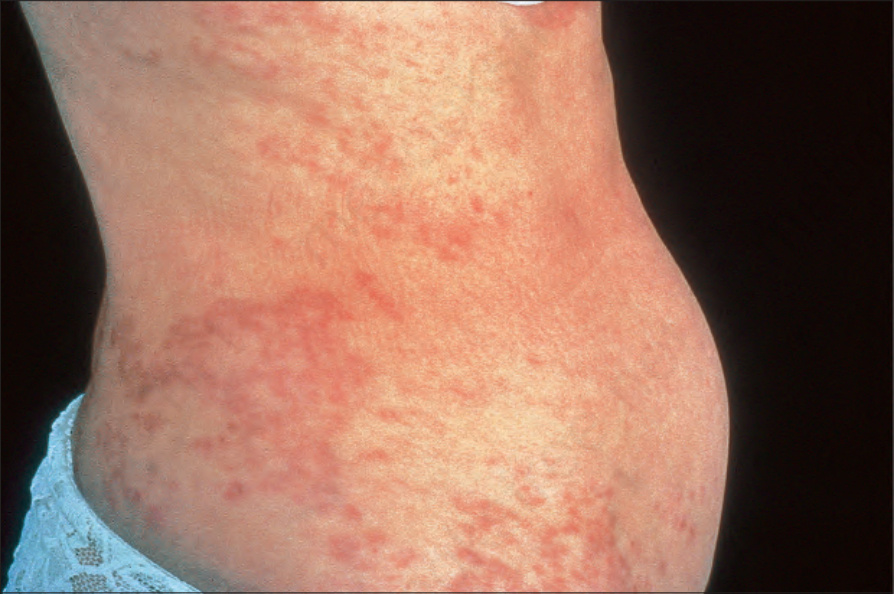
圖 9-29:泛發型 granuloma annulare:有廣泛的丘疹與斑塊。承蒙 the Institute of Dermatology, London, UK 提供。
Fig. 9.29 Generalized granuloma annulare: there are widespread papules and plaques. By courtesy of the Institute of Dermatology, London, UK.

圖 9-30:泛發型 granuloma annulare:在此病人中,出現許多環狀病灶。取自已故 N.P. Smith, MD, the Institute of Dermatology, London, UK 的收藏。
Fig. 9.30 Generalized granuloma annulare: in this patient, numerous annular lesions are present. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 9-31:穿透型 granuloma annulare:四肢最常受侵犯。可見壞死碎屑 (necrotic debris) 與痂皮。取自已故 N.P. Smith, MD, the Institute of Dermatology, London, UK 的收藏。
Fig. 9.31 Perforating granuloma annulare: the extremities are most often affected. Necrotic debris and crust can be seen. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 9-33:丘疹型 granuloma annulare:出現許多細小、有鱗屑的丘疹。承蒙 the Institute of Dermatology, London, UK 提供。
Fig. 9.33 Papular granuloma annulare: numerous small, scaly papules are present. By courtesy of the Institute of Dermatology, London, UK.
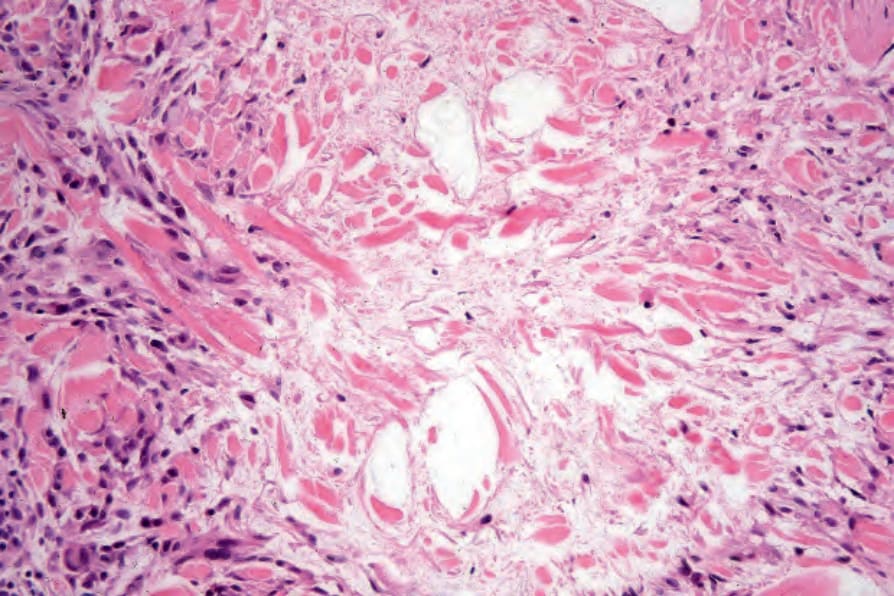
圖 9-36:局限型 granuloma annulare:膠原蛋白破碎,部分呈顆粒狀。注意周邊組織球柵欄狀排列 (peripheral palisade of histiocytes)、偶見的淋巴球與纖維母細胞 (fibroblasts)。
Fig. 9.36 Localized granuloma annulare: the collagen is fragmented and in part granular. Note the peripheral palisade of histiocytes, occasional lymphocytes, and fibroblasts.
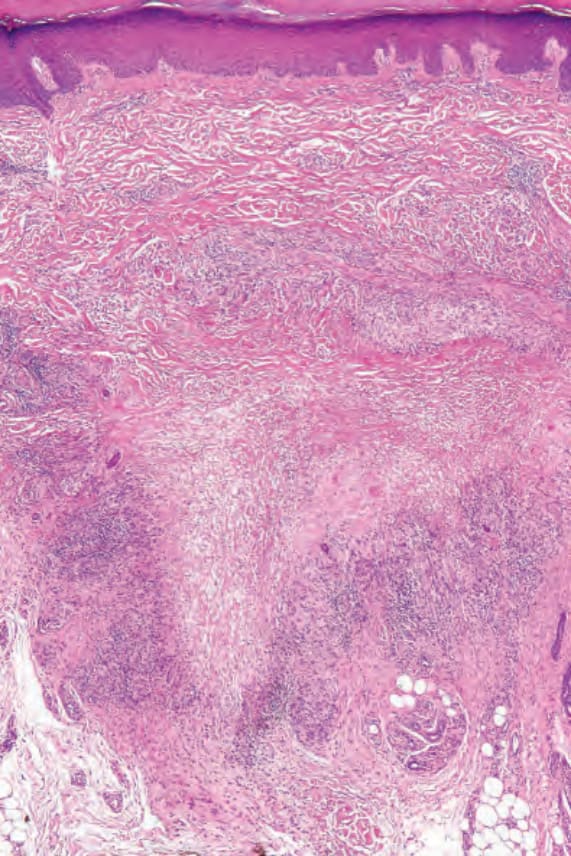
圖 9-37:局限型 granuloma annulare:此病灶取自手掌,為不常受侵犯的部位。在深部網狀真皮 (deep reticular dermis) 中有一界線清晰的壞死性壞死 (necrobiosis) 病灶。
Fig. 9.37 Localized granuloma annulare: this lesion is from the palm of the hand, an uncommonly affected site. There is a sharply delineated focus of necrobiosis in the deep reticular dermis.
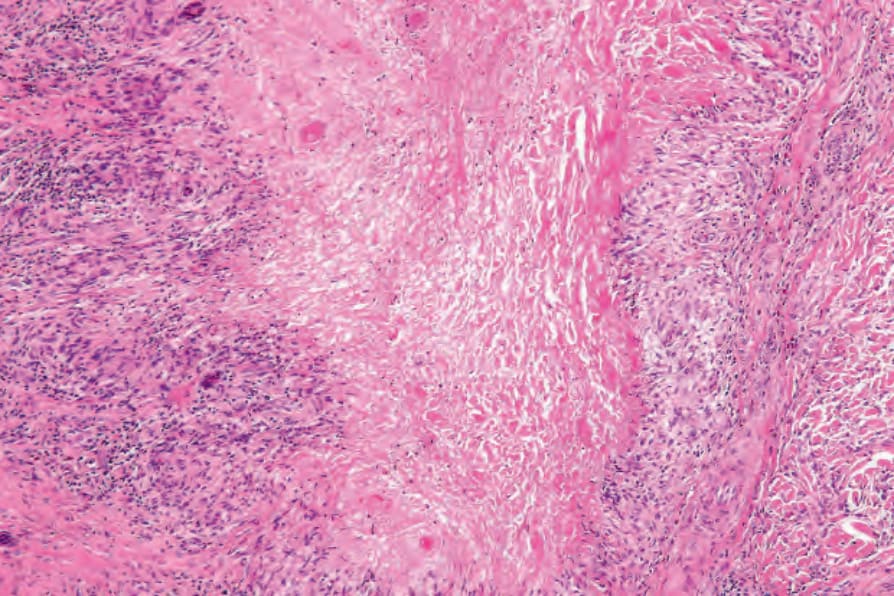
圖 9-38:局限型 granuloma annulare:壞死 (necrobiosis) 進展,表現為嗜伊紅性顆粒狀碎屑 (eosinophilic granular debris)。組織球柵欄 (histiocytic palisade) 已明確形成。
Fig. 9.38 Localized granuloma annulare: the necrobiosis is advanced, presenting as eosinophilic granular debris. The histiocytic palisade is well established.
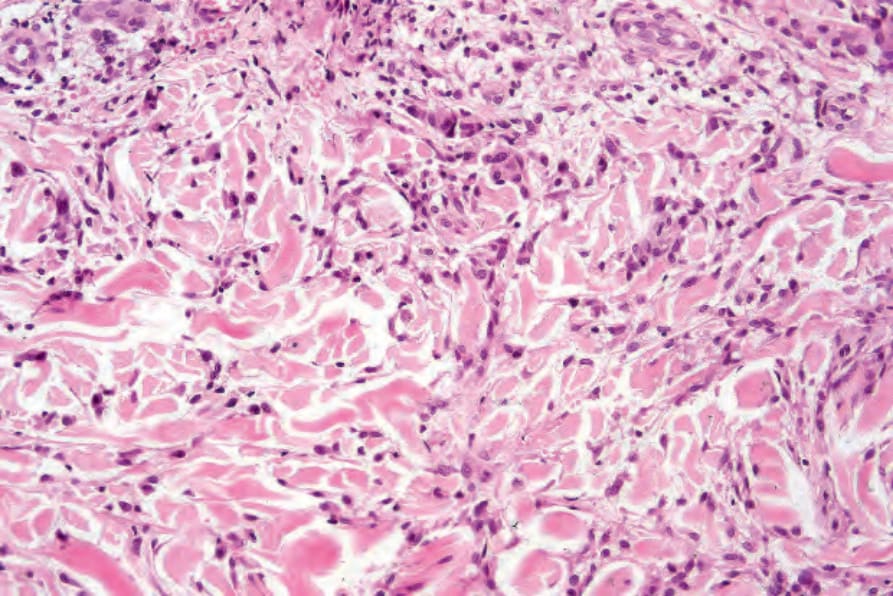
圖 9-44:瀰漫型 granuloma annulare:高倍視野顯示緻密的間質性組織球浸潤 (interstitial histiocytic infiltrate)。
Fig. 9.44 Diffuse granuloma annulare: higher-power view showing the dense interstitial histiocytic infiltrate.
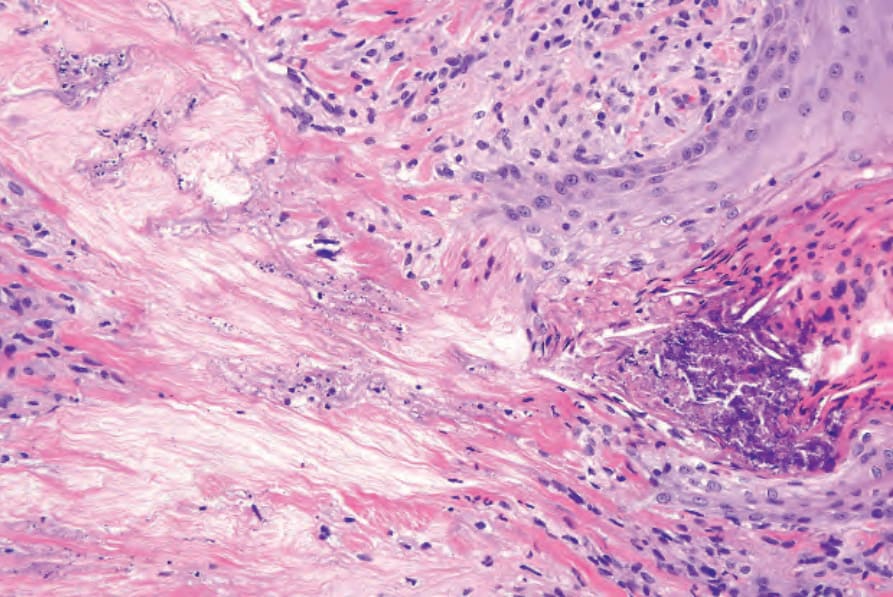
圖 9-47:穿透型 granuloma annulare:近觀顯示真皮穿孔 (dermal perforation) 與膠原性碎屑的經表皮排除 (transepidermal elimination of collagenous debris)。在一項研究中,66% 的切片中出現嗜伊紅性球,其中 14% 顯示每高倍視野超過 10 個嗜伊紅性球。漿細胞 (Plasma cells) 罕見,這在與 necrobiosis lipoidica 的鑑別診斷上有用(見下文)。嗜中性球 (Neutrophils) 是罕見的發現,當其出現時,特別是合併血管炎 (vasculitis) 變化時,很可能與全身性疾病有關。罕見地,可能遇到伴隨顯著淋巴球浸潤而類似淋巴瘤者。
Fig. 9.47 Perforating granuloma annulare: close-up view showing the dermal perforation and transepidermal elimination of collagenous debris. encountered.127 In one study, eosinophils were present in 66% of biopsies, of which 14% showed more than 10 eosinophils per high-power field.126 Plasma cells are rare, and this is useful in the differential diagnosis with necrobiosis lipoidica (see below). Neutrophils are a rare finding and when present, particularly in association with changes of vasculitis, it is likely that there is an association with systemic disease.128 Rarely, an associated prominent lymphocytic infiltrate mimicking a lymphoma may be encountered.129
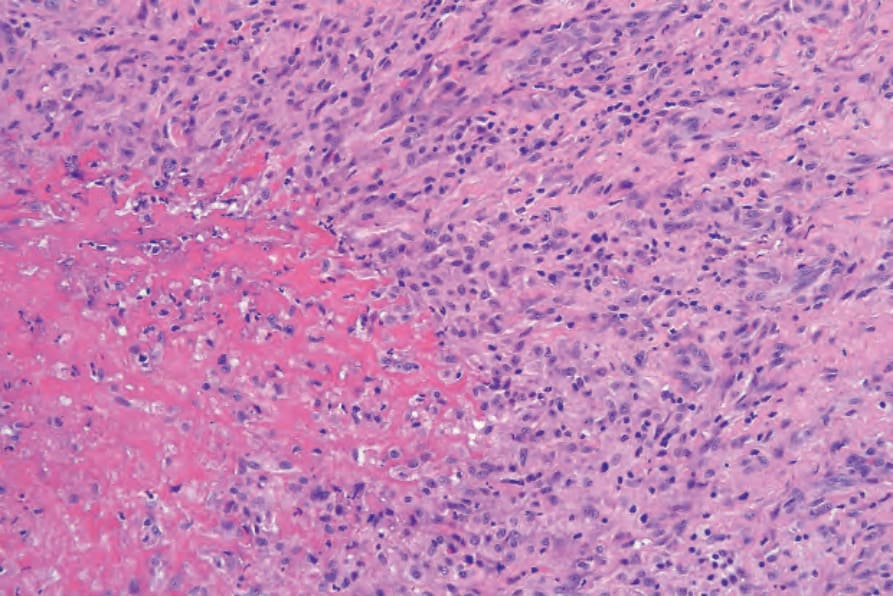
圖 9-49:皮下型 granuloma annulare:注意強烈嗜伊紅性的壞死 (necrobiosis) 與周圍纖維化。
Fig. 9.49 Subcutaneous granuloma annulare: note the intensely eosinophilic necrobiosis and surrounding fibrosis.
通常在數年後消退。然而,19% 的病人出現復發。
丘疹型 granuloma annulare (Papular granuloma annulare)
丘疹型 granuloma annulare 表現為膚色或色素減退、直徑 1–3 mm 的丘疹,位於手部背側,通常見於男性兒童。可能出現手掌與足底的侵犯,罕見地病灶會疼痛。偶有病灶可能呈臍狀 (umbilicated) 或泛發性(圖 9.32 與 9.33)。
線狀型 granuloma annulare (Linear granuloma annulare)
線狀型變異型非常罕見,可能呈雙側分布。罕見地,它可能沿 Blaschko lines 分布。此變異型與被描述為柵欄狀嗜中性球與肉芽腫性皮膚炎 (palisading neutrophilic and granulomatous dermatitis) 的疾病有重疊,且某些情況下可能即為同一疾病。
致病機轉與組織學特徵 (Pathogenesis and histologic features)
Granuloma annulare 的病因不明。原本認為它代表一種結核疹 (tuberculid) 的概念早已被否定。雖然它曾被報告於先前帶狀疱疹感染與尋常疣 (verruca vulgaris) 的部位,但感染性致病機轉不太可能存在。在數例 granuloma annulare 病人的切片中,曾以聚焦漂浮顯微術 (focus-floating microscopy) 證實 Borrelia,提出此微生物在某些病例中可能扮演致病角色的可能性。然而,一項以 PCR 為基礎的研究發現 granuloma annulare 與 Borrelia 感染之間並無關聯。目前可能的致病機轉種類繁多,其中多數有一定依據,但無一能令人滿意地闡明 granuloma annulare 病灶發生的精確機制。特別受歡迎的是免疫複合體血管炎過程 (immune complex vasculitic process) 與細胞媒介的延遲型過敏反應 (cell-mediated delayed hypersensitivity reaction)。支持前者的證據是,以直接免疫螢光 (direct immunofluorescence) 在某些病人的血管壁中偵測到免疫反應物 (immunoreactants)(IgM 與補體)。亦曾記錄到循環免疫複合體 (circulating immune complexes) 濃度升高。組織學可能顯示提示血管炎過程的特徵,包括內皮腫脹 (endothelial swelling)、血管壁增厚(由於 PAS 陽性物質的沉積)、血管阻塞與壞死(圖 9.34)。當然,後述所有變化都可能是發炎過程的結果,而非其原因。一項對 35 位病人 38 件切片進行連續切片 (serial sections) 的研究,在任何病例中均未發現血管炎過程的證據。
支持細胞媒介延遲型過敏反應的有:
- 在電子顯微鏡檢查中於 granuloma annulare 病灶內發現活化的 T 淋巴球,
- 浸潤中以 T 輔助誘導細胞 (T-helper inducer cells) 為主,
- 浸潤在組織病理上與已知由延遲型過敏致病的疾病(包括 sarcoidosis 與結核)相似。
有人提出,表現 interferon-gamma 的 Th1 淋巴球誘發延遲型過敏反應,導致巨噬細胞 (macrophages) 成為侵略性效應細胞,表現腫瘤壞死因子-alpha (tumor necrosis factor-alpha) 與基質金屬蛋白酶 (matrix metalloproteinases)。若腫瘤壞死因子 alpha 在此病的誘發中扮演角色,則阻斷此細胞激素的製劑可能對治療此病有用。雖然部分病人對這些製劑有反應,但其他病人則無,原因尚不清楚。具有泛發型 granuloma annulare 與 8.1 祖先單倍型 (8.1 ancestral haplotype)(一種導致腫瘤壞死因子 alpha 生成增加的基因型)的同卵雙胞胎,對 adalimumab 反應良好。
Granuloma annulare 病人可能有血清移動抑制因子 (serum migration inhibition factor) 活性升高。亦曾報告嗜中性球移動缺陷 (Defective neutrophil migration)。其他提出的致病機轉包括以巨噬細胞溶酶體水解酶 (macrophage lysosomal hydrolytic enzymes) 造成膠原蛋白損傷為起始事件,或膠原蛋白的原發性疾患導致過敏性或非過敏性組織反應。糖尿病 (diabetes mellitus) 與 HLA-B8 發生率增加亦可能具有致病意義(與 necrobiosis lipoidica 比較)。在一項對一群有多發性 granuloma annulare 病灶的兒科病人的研究中,發現他們的血清胰島素值顯著低於對照組,並顯示輕度葡萄糖耐受不良 (glucose tolerance) 損害。然而,這些兒童常有糖尿病家族史。
雖然有報告指出泛發型 granuloma 與陽光有關,但此關聯似乎意義可疑。
已顯示膠質瘤相關致癌基因同源物 gli-1 (glioma-associated oncogene homologue gli-1),一種屬於 gli 超家族脊椎動物鋅指轉錄因子基因 (zinc finger transcription factor genes) 的成員,在包括 granuloma annulare 在內的多種肉芽腫性疾病中高度表現。此在 granuloma annulare 致病機轉中的相關性尚不清楚,但它提出了在治療肉芽腫性非感染性疾病中使用 gli-1 訊息傳遞抑制劑的可能性。
granuloma annulare 中所見最具特徵性的組織學病灶為柵欄狀肉芽腫 (palisading granuloma)(圖 9.35–9.38)。它由退化(壞死性 necrobiotic)膠原蛋白的中央核心構成,周圍環繞常呈放射狀排列的淋巴球、組織球與纖維母細胞浸潤。彈性組織 (Elastic tissue) 在這些病灶內可能缺失,在肉芽腫周邊可有巨細胞 (giant cells) 對彈性纖維的吞噬作用(圖 9.39)。然而,彈性纖維的改變並非恆定的發現。日光性彈性變性 (Solar elastosis) 不是 granuloma annulare 的特徵。在某些病灶中,由於存在酸性黏多醣 (acid mucopolysaccharides),改變的膠原蛋白呈現某種程度的嗜鹼性外觀,但更常見的是由於纖維蛋白沉積 (fibrin deposition) 而呈嗜伊紅性(圖 9.40)。硫酸肝素 (Heparin sulfate) 是 granuloma annulare 黏蛋白 (mucin) 的重要成分,但不是其他伴隨黏蛋白沉積的皮膚疾病的成分(圖 9.41)。
偶爾,病灶中央會出現稀疏的核破裂碎屑 (karyorrhectic debris),有時壞死性病灶含有脂質滴 (lipid droplets)。然而更常見的是,膠原性退化並未組織成結節狀模式,而是以隨機模式影響孤立的纖維,此外觀常在低倍檢查下最易觀察(圖 9.42)。在此所謂瀰漫型或間質型 (diffuse or interstitial form) 的 granuloma annulare 中,受影響的纖維(腫脹且強烈嗜伊紅性)與外觀正常的纖維交替出現,
呈現出相當紊亂的外觀(圖 9.43 與 9.44)。壞死 (Necrobiosis) 極微或缺失。特徵性地,膠原纖維被黏蛋白分隔,後者在 pH 2.5 下以 Alcian blue 染色呈陽性。組織球常見浸潤於受影響纖維周圍與纖維之間,此特徵在膠原蛋白變化不明顯的早期病例中可能是有助於診斷的線索,因此應鼓勵檢查額外的切片以偵測更典型的特徵(圖 9.45)。
granuloma annulare 幾乎不可避免的特徵是出現血管周圍慢性發炎細胞浸潤 (perivascular chronic inflammatory cell infiltrate),既在病灶內,也在鄰近組織中。在某些病例中可見伴有巨細胞的成形良好之類肉狀肉芽腫 (sarcoidal granulomata)。在某些病例中可遇到顯著數量的嗜伊紅性球,
[註:以下段落於原文中接續皮下型組織學內容]
常常存在。後者似乎在此變異型中比在普通 granuloma annulare 中更常見。周圍組織的纖維化可能很明顯。在高達 25% 的皮下型 granuloma annulare 病例中,真皮中可見典型 granuloma annulare 的變化。
雖然與 Borrelia 感染的關係尚有爭議,但有人提出 granuloma annulare 中假玫瑰花環 (pseudorosettes) 的形成可能提示此微生物的感染。
在穿透型 granuloma annulare 中,壞死性碎屑緊鄰表皮,可見被表皮吞噬而形成穿透通道 (perforating channel),壞死物質藉此被擠出至表面(圖 9.46 與 9.47)。若進行連續切片,常可顯示穿孔通過毛囊 (hair follicle) 發生。
皮下病灶比表淺病灶大得多(圖 9.48 與 9.49),且常由多個結節組成。通常有大量壞死 (massive necrobiosis) 與豐富的黏蛋白;偶爾可見脂質滴。然而,黏蛋白可能極微或不明顯,若有纖維蛋白沉積,則無法與類風濕結節 (rheumatoid nodule) 區分。一圈緻密的淋巴球、組織球與纖維母細胞環繞壞死性中央。多核巨細胞 (Multinucleate giant cells) 常見,嗜伊紅性球
丘疹型與線狀型變異型顯示與典型 granuloma annulare 所述相似的組織學特徵。
鑑別診斷 (Differential Diagnosis)
Granuloma annulare 必須與 necrobiosis lipoidica、類風濕結節 (rheumatoid nodule)、日光性肉芽腫 (actinic granuloma),以及多形性肉芽腫 (granuloma multiforme) 區分。鑑別要點摘錄於表 9.1。
已報告 adipophilin 表現的模式在 granuloma annulare、necrobiosis lipoidica 與 sarcoidosis 的組織學區分上有用。在 granuloma annulare,adipophilin 染色模式相對於浸潤中的組織球,同時為細胞內與細胞外。在 necrobiosis lipoidica,染色模式傾向於在異常膠原蛋白區域內完全為細胞外,而在 sarcoidosis,染色模式通常完全為組織球內的細胞內。
偶爾,granuloma annulare 可能顯示類上皮細胞肉芽腫 (epithelioid cell granulomas) 而類似 sarcoidosis。然而,背景中黏蛋白的存在

圖 9-32:丘疹型 granuloma annulare:此病人的背部與肩部出現廣泛的丘疹。承蒙 the Institute of Dermatology, London, UK 提供。
Fig. 9.32 Papular granuloma annulare: widespread papules are present on this patient’s back and shoulders. By courtesy of the Institute of Dermatology, London, UK.
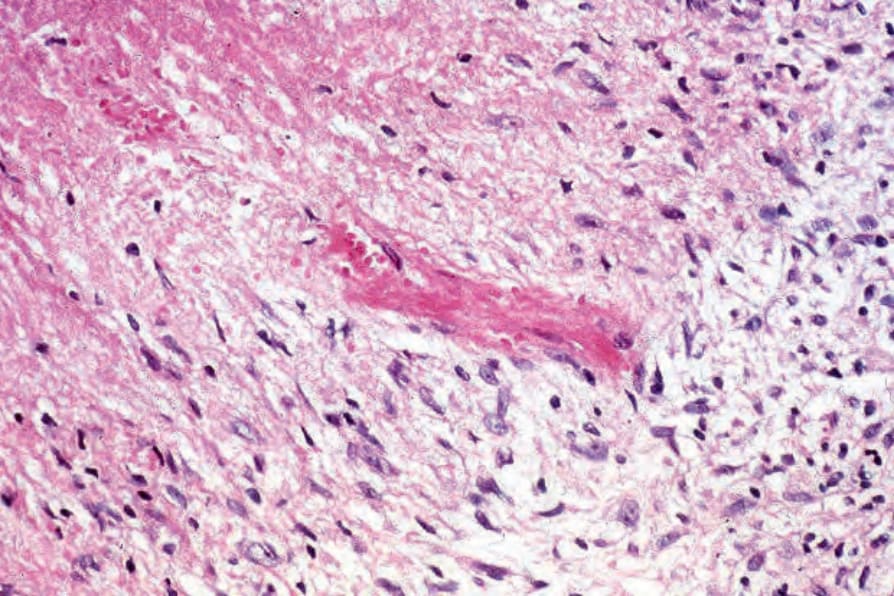
圖 9-34:Granuloma annulare:透過壞死性病灶邊緣的視野。在中央,一小血管顯示纖維素樣壞死 (fibrinoid necrosis) 並阻塞。這是不常見的發現。
Fig. 9.34 Granuloma annulare: view through the edge of a necrobiotic focus. In the center, a small blood vessel shows fibrinoid necrosis with occlusion. This is an uncommon finding.
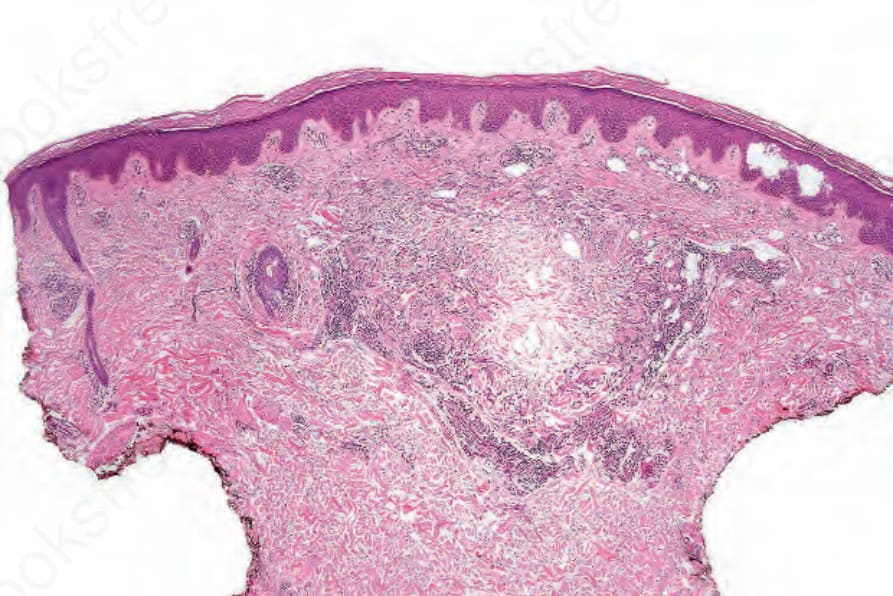
圖 9-35:局限型 granuloma annulare:界線清晰的柵欄狀肉芽腫 (palisading granuloma) 的特徵性外觀,由壞死性中央 (necrobiotic center) 周圍環繞細胞浸潤所構成。
Fig. 9.35 Localized granuloma annulare: the characteristic appearance of a wellcircumscribed palisading granuloma consisting of a necrobiotic center surrounded by a cellular infiltrate.
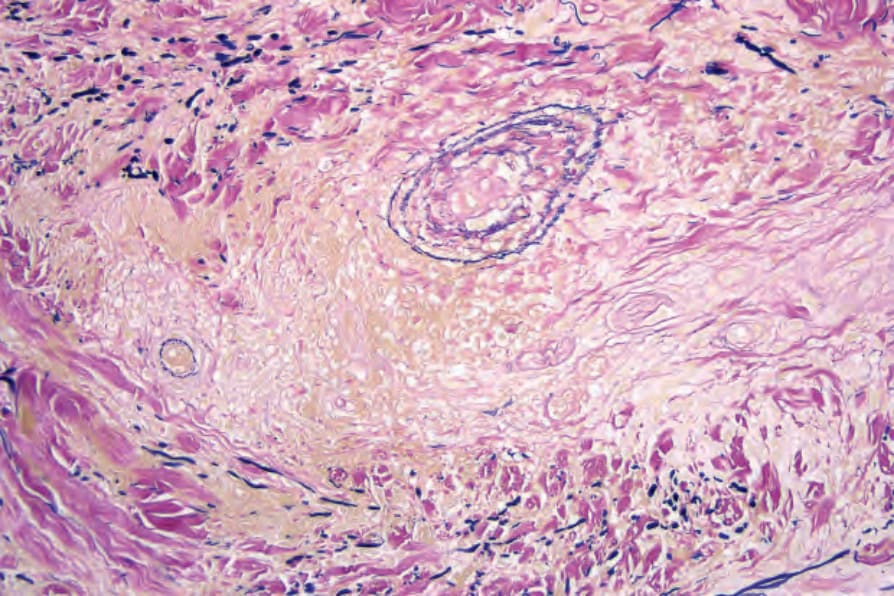
圖 9-39:局限型 granuloma annulare:肉芽腫內有彈性組織的喪失。Elastic-van Gieson 染色。
Fig. 9.39 Localized granuloma annulare: there is loss of elastic tissue within the granuloma. Elastic-van Gieson.
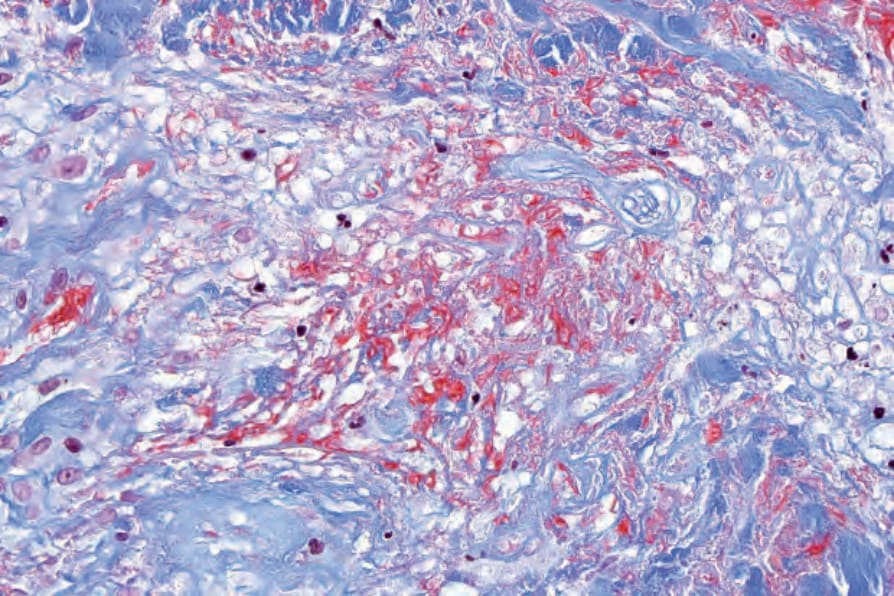
圖 9-40:局限型 granuloma annulare:肉芽腫中央的紅色染色物質為纖維蛋白 (fibrin)。Martius scarlet blue 染色。
Fig. 9.40 Localized granuloma annulare: the red-staining material in the center of the granuloma is fibrin. Martius scarlet blue.
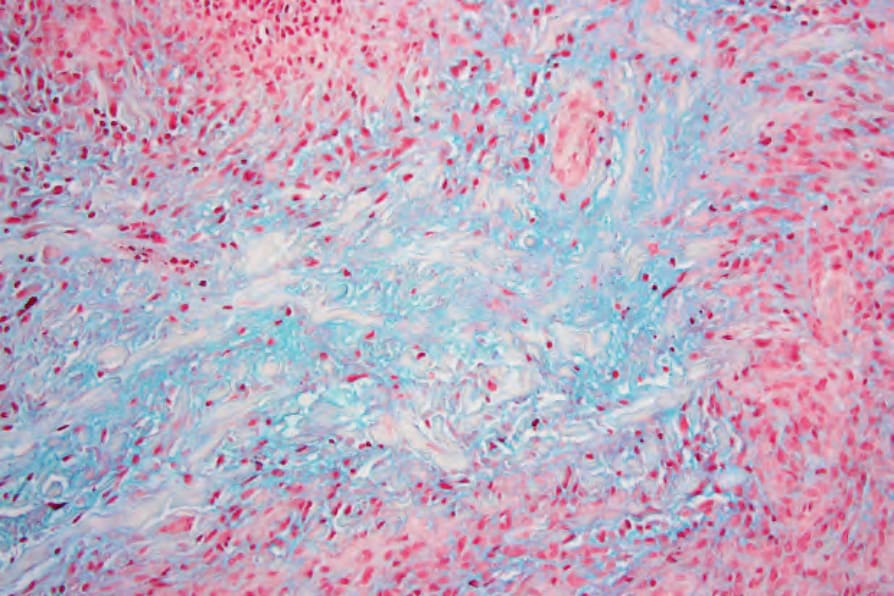
圖 9-41:局限型 granuloma annulare:在此例中,壞死性病灶中央有豐富的黏蛋白 (mucin)。Alcian blue 染色。
Fig. 9.41 Localized granuloma annulare: in this example, there is abundant mucin in the center of the necrobiotic focus. Alcian blue stain.
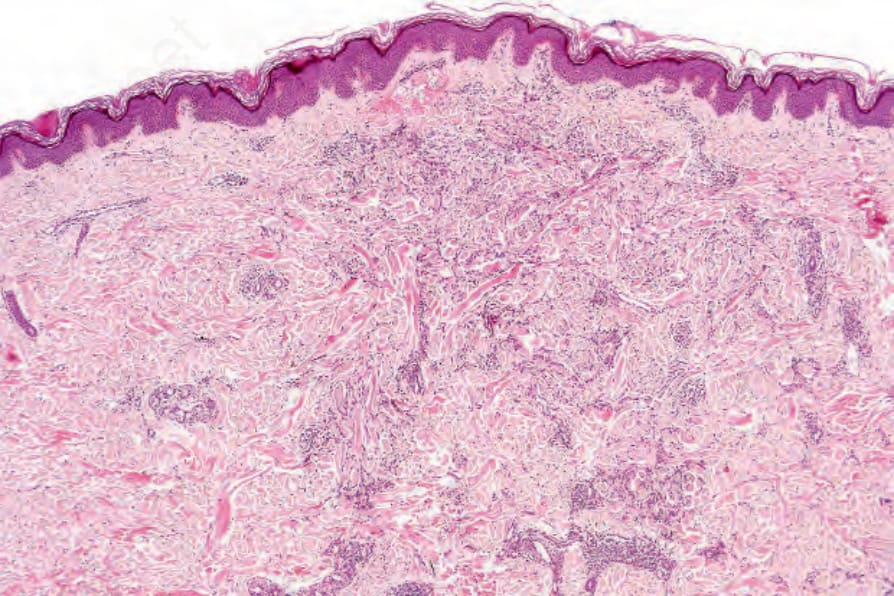
圖 9-42:瀰漫型 granuloma annulare:膠原束 (collagen bundles) 雜亂排列。注意環周的淋巴球浸潤。
Fig. 9.42 Diffuse granuloma annulare: the collagen bundles are arranged haphazardly. Note the circumferential lymphocytic infiltrate.
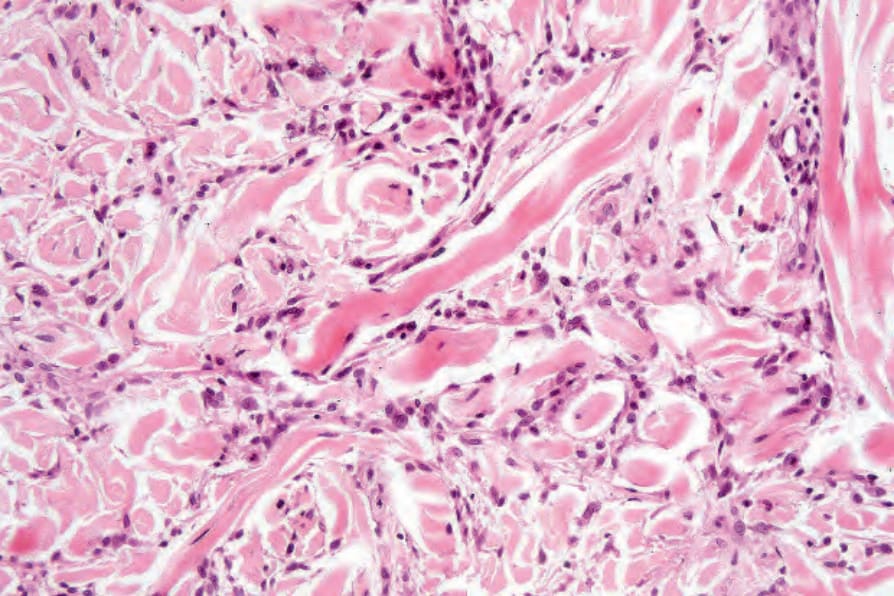
圖 9-43:瀰漫型 granuloma annulare:個別纖維腫脹且強烈嗜伊紅性。纖維的明顯分隔是由於黏蛋白增加所致。
Fig. 9.43 Diffuse granuloma annulare: individual fibers are swollen and intensely eosinophilic. The apparent separation of the fibers is due to increased mucin.
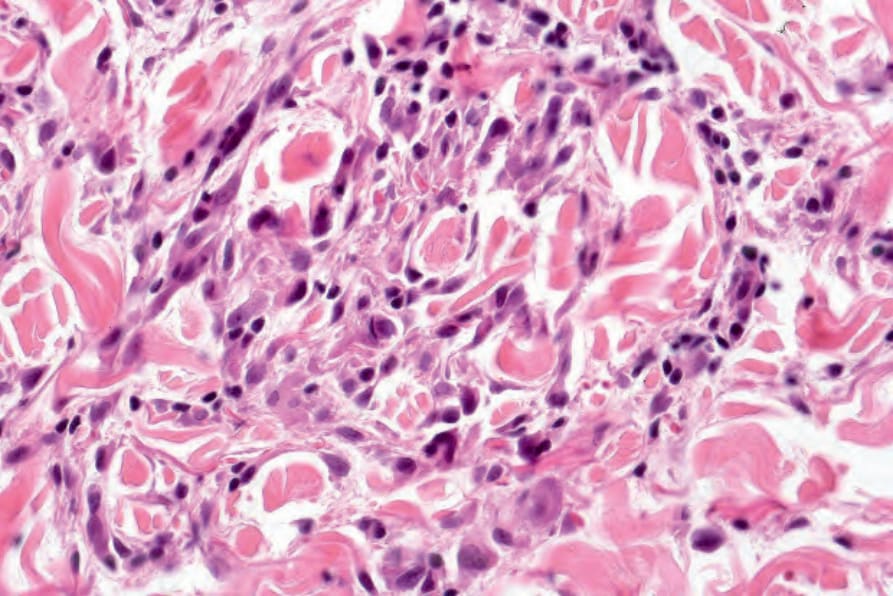
圖 9-45:瀰漫型 granuloma annulare:高倍視野。
Fig. 9.45 Diffuse granuloma annulare: high-power view.
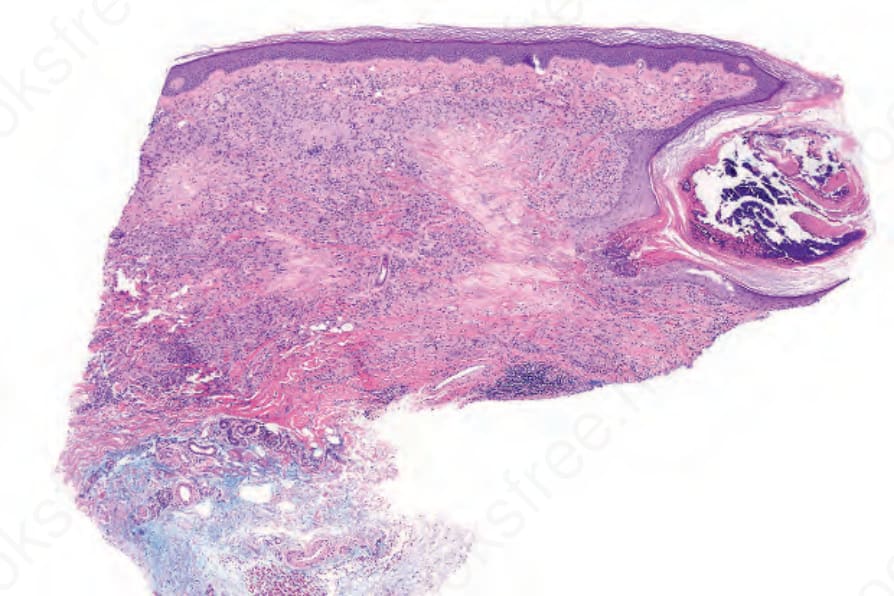
圖 9-46:穿透型 granuloma annulare:掃描視野顯示廣泛的典型 granuloma annulare(在右上象限,退化的膠原蛋白正在進行經表皮排除 transepidermal elimination)。
Fig. 9.46 Perforating granuloma annulare: scanning view showing widespread typical granuloma annulare (in the upper-right quadrant, degenerate collagen is undergoing transepidermal elimination).
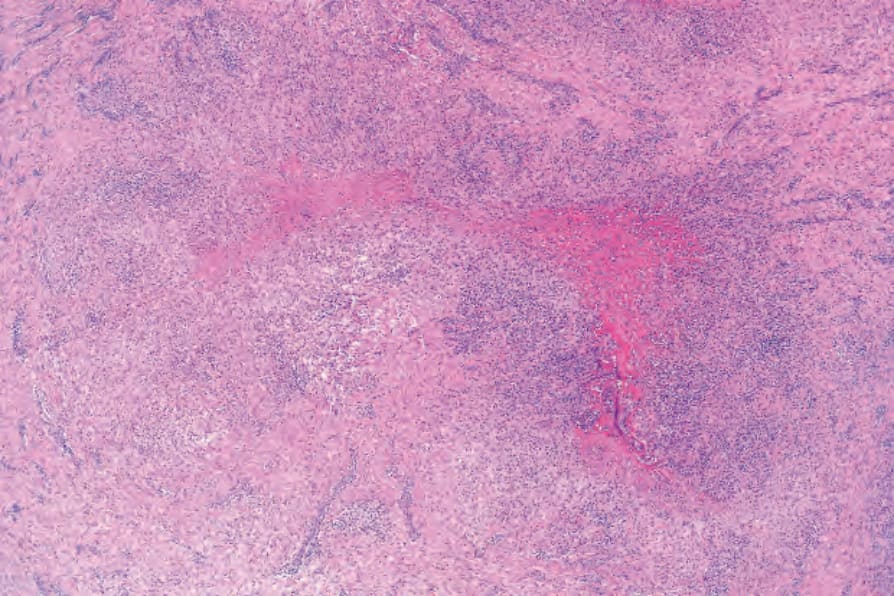
圖 9-48:皮下型 granuloma annulare:在皮下脂肪內並侵犯筋膜 (fascia),有一巨大的壞死性結節 (necrobiotic nodule)。
Fig. 9.48 Subcutaneous granuloma annulare: within the subcutaneous fat and involving the fascia is a massive necrobiotic nodule.
[註:原文於此處插入 Table 9.1 內容;表格之文字資料於原文中呈分散流式排列,依鐵則 1:1 鏡射原文順序、不重排]
Granuloma annulare (GA)
皮下型 GA 穿透型 GA
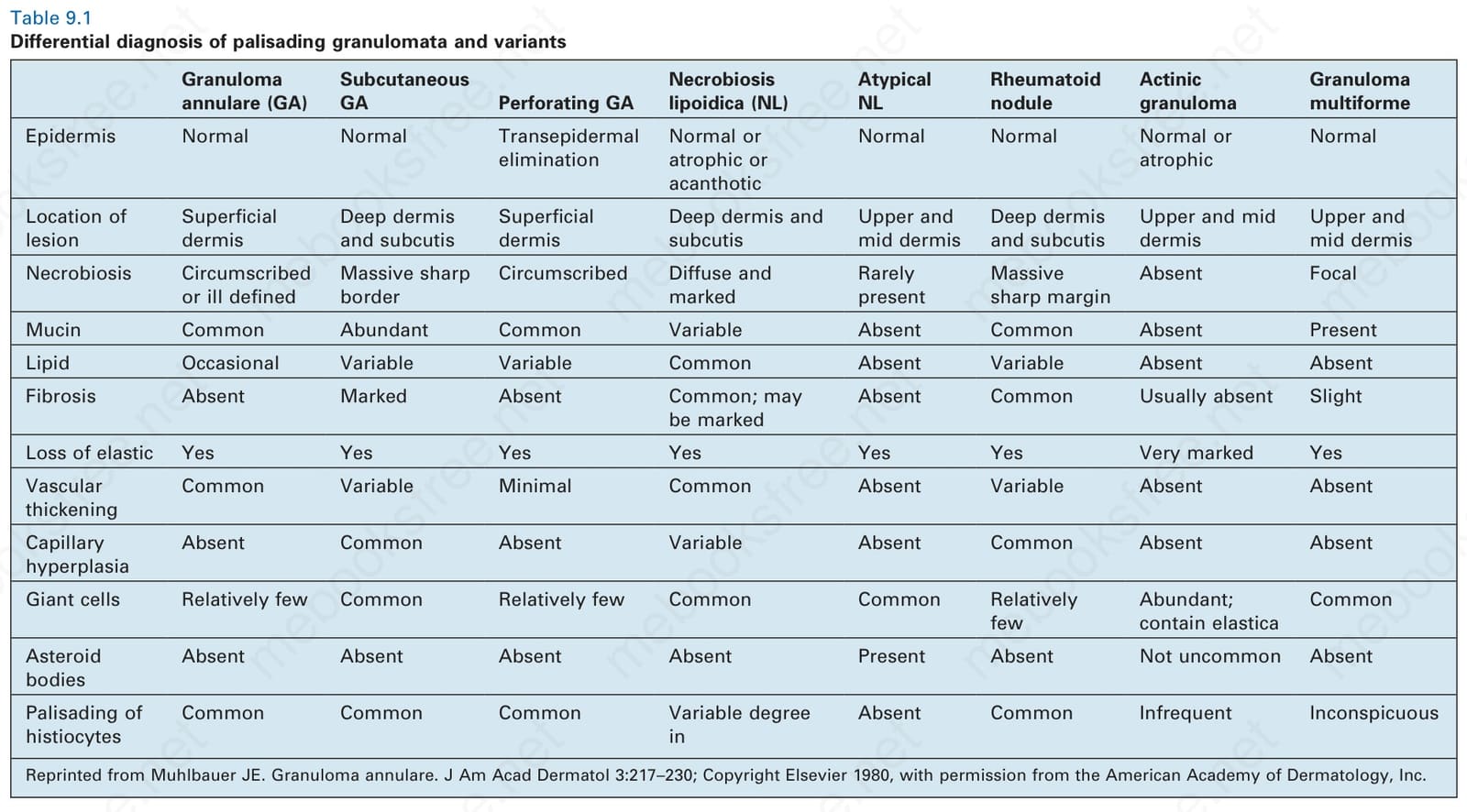
表 9-1:柵欄狀肉芽腫及其變異型之鑑別診斷 (Differential diagnosis of palisading granulomata and variants)。
Table 9.1 Differential diagnosis of palisading granulomata and variants
類脂質漸進性壞死 (Necrobiosis lipoidica, NL)
表皮 (Epidermis):正常 正常 經表皮排除 (Transepidermal elimination)
非典型 NL (Atypical NL)
類風濕結節 (Rheumatoid nodule)
日光性肉芽腫 (Actinic granuloma)
多形性肉芽腫 (Granuloma multiforme)
正常或萎縮或棘層肥厚 (Normal or atrophic or acanthotic)
病灶位置 (Location of lesion)
表淺真皮 (Superficial dermis)
深部真皮與皮下 (Deep dermis and subcutis)
表淺真皮 (Superficial dermis)
正常 正常 正常或萎縮 (Normal or atrophic)
正常 (Normal)
深部真皮與皮下 (Deep dermis and subcutis)
壞死 (Necrobiosis):界線清楚或界線不清 (Circumscribed or ill defined)
巨大且邊界銳利 (Massive sharp border)
上層與中層真皮 (Upper and mid dermis)
深部真皮與皮下 (Deep dermis and subcutis)
上層與中層真皮 (Upper and mid dermis)
上層與中層真皮 (Upper and mid dermis)
界線清楚 (Circumscribed) 瀰漫且明顯 (Diffuse and marked)
罕見出現 (Rarely present)
巨大且邊緣銳利 (Massive sharp margin)
缺失 (Absent) 局灶 (Focal)
黏蛋白 (Mucin):常見 (Common) 豐富 (Abundant) 常見 (Common) 不定 (Variable) 缺失 (Absent) 常見 (Common) 缺失 (Absent) 存在 (Present)
脂質 (Lipid):偶見 (Occasional) 不定 (Variable) 不定 (Variable) 常見 (Common) 缺失 (Absent) 不定 (Variable) 缺失 (Absent) 缺失 (Absent)
纖維化 (Fibrosis):缺失 (Absent) 明顯 (Marked) 缺失 (Absent) 常見;可能明顯 (Common; may be marked)
缺失 (Absent) 常見 (Common) 通常缺失 (Usually absent) 輕微 (Slight)
彈性組織喪失 (Loss of elastic):是 (Yes) 是 (Yes) 是 (Yes) 是 (Yes) 是 (Yes) 是 (Yes) 非常明顯 (Very marked) 是 (Yes)
血管增厚 (Vascular thickening)
常見 (Common) 不定 (Variable) 極微 (Minimal) 常見 (Common) 缺失 (Absent) 不定 (Variable) 缺失 (Absent) 缺失 (Absent)
微血管增生 (Capillary hyperplasia)
缺失 (Absent) 常見 (Common) 缺失 (Absent) 不定 (Variable) 缺失 (Absent) 常見 (Common) 缺失 (Absent) 缺失 (Absent)
巨細胞 (Giant cells):相對較少 (Relatively few) 常見 (Common) 相對較少 (Relatively few) 常見 (Common) 常見 (Common) 相對較少 (Relatively few)
星狀體 (Asteroid bodies)
豐富;含彈性蛋白 (Abundant; contain elastica)
常見 (Common)
缺失 (Absent) 缺失 (Absent) 缺失 (Absent) 缺失 (Absent) 存在 (Present) 缺失 (Absent) 不罕見 (Not uncommon) 缺失 (Absent)
組織球柵欄狀排列 (Palisading of histiocytes)
常見 (Common) 常見 (Common) 常見 (Common) 程度不定 (Variable degree)
缺失 (Absent) 常見 (Common) 不常見 (Infrequent) 不明顯 (Inconspicuous)
Reprinted from Muhlbauer JE. Granuloma annulare. J Am Acad Dermatol 3:217–230; Copyright Elsevier 1980, with permission from the American Academy of Dermatology, Inc.
在具挑戰性的病例中,背景中黏蛋白的存在連同其他更典型的 granuloma annulare 變化,可允許作出區分。
在全身性疾病的情境下,可能遇到附加血管炎 (vasculitis) 特徵與顯著急性發炎細胞成分的 granuloma annulare 樣病灶。此疾病模式於柵欄狀嗜中性球與肉芽腫性皮膚炎 (palisaded neutrophilic and granulomatous dermatitis) 及相關疾病的章節中詳細討論。
曾報告 granuloma annulare 樣藥物疹 (granuloma annulare-like drug eruptions)。伴隨介面變化 (interface changes) 的存在傾向支持藥物疹。
極罕見地,硬化性黏液水腫 (scleromyxedema) 在組織學上可能局灶性地類似間質性 granuloma annulare。然而,模擬 granuloma annulare 的變化是局灶性的,切片其他部位有更典型的 scleromyxedema 特徵,包括纖維化與纖維母細胞增加。
偶爾,Mycobacterium marinum 感染可能類似間質性 granuloma annulare。顯微特徵可能如此相似,以致僅能藉由特殊染色與培養作出診斷。
雖然類上皮肉瘤 (epithelioid sarcoma),連同其伴隨的地圖狀壞死 (geographic necrosis),在低倍檢查下可能與 granuloma annulare 有表面上的相似,但前者的核異型性 (nuclear atypia) 與多形性 (pleomorphism) 程度,在大多數病例中應可區分兩者。此外,epithelioid sarcoma 常顯示神經周圍腫瘤浸潤 (perineural tumor infiltration)。然而應注意,granuloma annulare 中可能遇到有絲分裂活性 (mitotic activity)。在困難病例中,keratin、上皮膜 (epithelial membrane)、在高達 60% 的病例中的 CD34 抗原免疫反應性,以及 epithelioid sarcoma 中 INI1 表現的喪失,應有助於此鑑別診斷。
罕見病例的蕈狀肉芽腫 (mycosis fungoides) 可能伴隨類似 granuloma annulare 的組織反應。雖然間質性蕈狀肉芽腫 (interstitial mycosis fungoides) 可能在膠原束之間顯示組織球,但以具核異型性的間質性淋巴球為主、以及表皮趨向性 (epidermotropism)(一個在 granuloma annulare 中不見的特徵),應可解決此鑑別診斷。大多數間質性蕈狀肉芽腫病人有此病其他典型的臨床特徵。值得注意的是,皮膚 T 細胞淋巴瘤 (cutaneous T cell lymphoma) 中的間質性腫瘤細胞常具有細胞毒性表型 (cytotoxic phenotype)。
慢性萎縮性肢端皮膚炎 (Acrodermatitis chronica atrophicans) 罕見地可顯示類似 granuloma annulare 的組織學變化。然而,臨床病理相關性與前者中漿細胞 (plasma cells) 的存在通常可作出區分。