扁平苔癬 (Lichen planus)
臨床特徵 (Clinical Features)
扁平苔癬 (lichen planus)(希臘文 leichen,意指樹苔)是一種常見、通常劇烈搔癢、對稱性的丘疹鱗屑性 (papulosquamous) 皮膚病。其在一般族群中的盛行率約為 1%,最常出現在第四到第六個十年(四十至六十多歲),女性略多。兒童期罕見。偶有家族性病例的報告。
本病的特徵為小而平滑、有光澤、頂端扁平 (flat-topped) 的多角形丘疹,直徑數毫米至 1 cm,常呈紫羅蘭色 (violaceous color)(圖 7.1)。在略帶鱗屑的表面上,典型可見細緻的白色線條,稱為 Wickham striae(圖 7.2)。病灶最常見於手腕的屈側 (flexor aspect)、前臂、手與踝的伸側 (extensor aspect)、腰部,以及陰莖龜頭 (glans penis)(圖 7.3)。罕見病例也可能合併掌蹠角化症 (palmoplantar keratoderma)。可見環狀 (annular) 病灶。Lichen planus 與陽性 Koebner 現象 (Koebner phenomenon) 有關。本病通常為自限性,但有時病程遷延,患者通常在數週至 1 或 2 年內病灶消退。
眼部侵犯罕見,可能包括眼瞼病灶、瞼緣炎 (blepharitis)、結膜炎 (conjunctivitis)、角膜炎 (keratitis)、點狀角膜混濁 (punctate corneal opacities)、虹膜睫狀體炎 (iridocyclitis),以及脈絡膜視網膜炎 (chorioretinitis)。
食道侵犯雖然罕見,但是潛在重要的致病性 (morbidity) 原因,也是最常受侵犯的胃腸道部位。通常同時合併口腔病灶,但在罕見情況下,食道侵犯為最初的表現。迄今,受影響者典型為中年或老年女性。併發症包括慢性吞嚥困難 (dysphagia) 與影響食道中段或上段的狹窄 (stricture) 形成。食道扁平苔癬的患者可能有發展為鱗狀細胞癌 (squamous cell carcinoma) 的風險。部分患者可能在無口腔或皮膚表現的情況下,發展出與食道 lichen planus 相關的鱗狀細胞癌。監測的角色仍不確定。
口腔侵犯非常常見(影響高達 60% 的皮膚病患者),有明顯的女性優勢,最常出現在第七個十年(六十多歲)。它有時可能是唯一的表現(估計 15–35% 的口腔扁平苔癬患者從未發展出皮膚病灶)。可能受侵犯的部位依頻率遞減順序為頰黏膜 (buccal mucosa)、前庭 (vestibule)、舌、牙齦 (gingivae)、硬腭 (hard palate)、穹窿 (fornix)、唇與軟腭 (soft palate)。患者經常表現為白色蕾絲樣 (lacelike) 圖案,
扁平苔癬的生殖器病灶很常見(特別是男性),高達 25% 的患者出現,有時呈環狀 (annular) 構型(圖 7.8)。類似的環狀 lichen planus 也可能出現在身體其他部位,包括間擦 (intertriginous) 區域。偶爾陰莖病灶為本病的唯一表現,且與未割包皮 (uncircumcised) 的男性有關聯。外陰 (vulval) 病灶可見於高達 51% 有皮膚侵犯的女性。有時牙齦與女性生殖器病灶可能並存,為糜爛性扁平苔癬 (erosive lichen planus) 的一種變異型,即所謂的外陰陰道—牙齦症候群 (vulvovaginal-gingival syndrome)。患者表現為性交疼痛 (dyspareunia) 與劇烈灼熱的外陰疼痛。外陰呈充血外觀,可能有糜爛 (erosions),常被白色網狀 (reticulate) 邊緣所環繞。陰道侵犯同樣表現為性交疼痛,並常因發炎性、脫屑性與糜爛性變化而出現性交後出血。在身體其他部位可能遇到較典型的 lichen planus 特徵。鱗狀
242 Lichenoid and interface dermatitis
細胞癌 (squamous carcinoma) 是慢性外陰扁平苔癬重要的併發症,儘管罕見,且似乎在無毛 (nonhair-bearing) 黏膜較為常見。陰莖癌的發展罕見。扁平苔癬的生殖器侵犯於他處討論(見第 12 章)。
約 10% 的扁平苔癬患者指(趾)甲受侵犯;表現包括甲板 (nail plate) 變薄、縱向脊狀化 (longitudinal ridging)、條紋 (striations)、翼狀胬肉形成 (pterygium formation)、甲下角化過度 (subungual hyperkeratosis),以及非常罕見的指(趾)甲完全破壞(圖 7.9)。雖然據說兒童的指(趾)甲侵犯罕見,部分作者將兒童期二十甲營養不良症 (twenty-nail dystrophy of childhood) 視為局部性扁平苔癬的一種變異型,儘管並非所有人都接受此假說。
大多數病灶在發病後 6–18 個月內癒合。然而,口腔型與肥厚型 (hypertrophic) 變異型,以及毛囊扁平苔癬 (lichen planopilaris) 傾向呈慢性病程。
Box 7.1 苔癬樣皮膚炎 (lichenoid dermatitis) 的病因
• 扁平苔癬 (Lichen planus)
• 苔癬樣移植物抗宿主病 (Lichenoid graft-versus-host disease)
• 點狀苔癬 (Lichen nitidus)
• 苔癬樣角化症 (Lichenoid keratosis)
• 苔癬樣藥物反應 (Lichenoid drug reaction)
• 固定性藥物反應 (Fixed drug reaction)
• 毛囊扁平苔癬 (Lichen planopilaris)
• 線狀苔癬 (Lichen striatus)
• 成人 Blaschkitis (Adult Blaschkitis)
• 金黃色苔癬 (Lichen aureus)
• 苔癬樣蕈狀肉芽腫 (Lichenoid mycosis fungoides)
• 灰皮病 (Ashy dermatoses)
• 苔癬樣與肉芽腫性皮膚炎 (Lichenoid and granulomatous dermatitis)
A
Box 7.2 介面性皮膚炎 (interface dermatitis) 的病因
• 苔癬樣皮膚病 (Lichenoid dermatoses)(見 Box 7.1)
• 多形性紅斑 (Erythema multiforme)
• 史蒂芬斯—強生症候群/毒性表皮壞死溶解症 (Stevens-Johnson syndrome/toxic epidermal necrolysis)
• 結締組織疾病 (Connective tissue disorders):紅斑性狼瘡 (lupus erythematosus)、皮肌炎 (dermatomyositis),以及混合性結締組織疾病 (mixed connective tissue disorders)
• 移植物抗宿主病 (Graft-versus-host disease)
• 皮膚異色症 (Poikiloderma),包括與罕見遺傳性疾病相關者
• 介面性藥物反應 (Interface drug reactions)
• 介面性病毒疹 (Interface viral exanthem)
• 苔癬樣糠疹 (Pityriasis lichenoides)
B
243 Lichenoid dermatoses
發炎後色素沉著 (postinflammatory hyperpigmentation) 並不少見,特別是在膚色較深的人(圖 7.10)。
扁平苔癬有若干變異型值得特別提及:
• 毛囊扁平苔癬 (Lichen planopilaris)(濾泡性扁平苔癬,follicular lichen planus)表現為單個或多個瘢痕性禿髮 (scarring alopecia) 的斑塊,伴隨一系列病灶,包括侵犯頭皮的典型苔癬樣丘疹,到影響軀幹與四肢的褐色或紫羅蘭色角化性毛囊性丘疹 (keratotic follicular papules)(圖 7.11–7.13)。也可能出現具有顯著毛囊性丘疹的非瘢痕性斑塊。線狀病灶曾有罕見描述。部分作者認為頭皮扁平苔癬在某些病例中導致 Brocq 假性禿髮 (pseudopélade of Brocq),儘管該實體可能代表各種瘢痕性禿髮的末期。兒童
也可能受影響。Graham-Little-Picardi-Lasseur 症候群指的是毛囊扁平苔癬的一種變異型,其特徵為以下三聯徵:1. 頭皮多灶性瘢痕性禿髮;2. 腋窩與腹股溝的非瘢痕性禿髮;3. 身體其他部位、頭皮或兩者的濾泡性扁平苔癬 (follicular lichen planus)。
• 萎縮性扁平苔癬 (Atrophic lichen planus),其臨床特徵僅僅反映較典型活動期的消退。
• 光化性扁平苔癬 (Lichen planus actinicus)〔亞熱帶扁平苔癬 (lichen planus subtropicus)、夏季光化性苔癬樣疹 (summertime actinic lichenoid eruption, SALE)〕發生於長期暴露於日光的患者,因此通常在春季或夏季顯現,並在秋季或冬季改善或緩解。它特別發生於中東(尤其是埃及)與遠
244 Lichenoid and interface dermatitis
A
B
由不同程度搔癢的色素性深褐色斑 (macules) 所構成,主要影響暴露部位的皮膚與屈側皺褶 (flexures)(圖 7.15 和 7.16)。最常受影響的部位包括臉與頸,但間擦 (intertriginous) 區域也可能受影響(反轉型色素性扁平苔癬,lichen planus pigmentosus inversus)。無性別偏好。本病以加重與緩解交替的時期為特徵。例外情況下,曾有口腔黏膜受侵犯的紀錄。
• 肥厚性扁平苔癬 (Hypertrophic lichen planus),代表疊加的慢性單純苔癬 (lichen simplex chronicus),常影響下肢,特別是脛部 (shins),表現為高度色素沉著的疣狀 (warty) 斑塊(圖 7.17)。侵犯常局限於脛部,其他部位無病灶。家族性扁平苔癬顯示此變異型的發生率增加。病灶劇烈搔癢且非常頑固。伴隨有(雖然極輕微的)腫瘤性轉化 (neoplastic transformation) 的風險。
• 潰瘍性扁平苔癬 (Ulcerative lichen planus) 是一種慢性變異型,影響手指、手、足底與腳趾,常合併指(趾)甲的永久喪失(圖 7.18 和 7.19)。鱗狀細胞癌 (squamous cell carcinoma) 可能使此扁平苔癬變異型複雜化。
東,並影響較年輕的人,最大發生率在第二與第三個十年(二十至三十多歲),女性略多(圖 7.14)。受影響部位包括前額外側、手背、前臂、臉與頸。此疹可能包含扁平苔癬樣 (lichen planus-like) 與點狀苔癬樣 (lichen nitidus-like) 病灶的混合,而在其他人,病灶純粹表現為其中一種或另一種(見下文光化性點狀苔癬,actinic lichen nitidus)。典型上,lichen planus 病灶呈環狀構型,中央呈藍褐色、相當萎縮,邊緣略隆起。它們有時可能融合形成弧線狀 (circinate) 斑塊。偶爾曾有黑斑樣 (melasma-like) 外觀的紀錄。通常少有搔癢,且 Koebner 現象常缺如。指(趾)甲常不受影響。
• 色素性扁平苔癬 (Lichen planus pigmentosus),最常見於熱帶地區膚色深的患者,特徵為發展出
245 Lichenoid dermatoses
其他變異型包括線狀扁平苔癬 (lichen planus linearis),主要發生於兒童,以及罕見的水疱性或大疱性 (vesicular or bullous) 變異型,後者必須與類天疱瘡型扁平苔癬 (lichen planus pemphigoides) 區分。大疱性扁平苔癬 (bullous lichen planus) 指的是在既存的苔癬樣病灶上發展出水疱或大疱,是嚴重基底細胞水樣變性 (basal cell hydropic degeneration) 的結果。它更常是組織學上的發現,而非臨床觀察。相對地,lichen planus pemphigoides 的特徵為在身體其他部位有典型 lichen planus 的患者,於正常或紅斑皮膚上發展出大而緊繃的大疱。它代表 lichen planus 與大疱性類天疱瘡 (bullous pemphigoid) 的合併表現。
246 Lichenoid and interface dermatitis

圖 7.1:Lichen planus:手背上有典型頂端扁平的多角形丘疹 (flat-topped polygonal papules)。來自已故 N.P. Smith 醫師的收藏,倫敦皮膚科研究所,英國。
Fig. 7.1 Lichen planus: there are typical flat-topped polygonal papules on dorsum of the hand. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
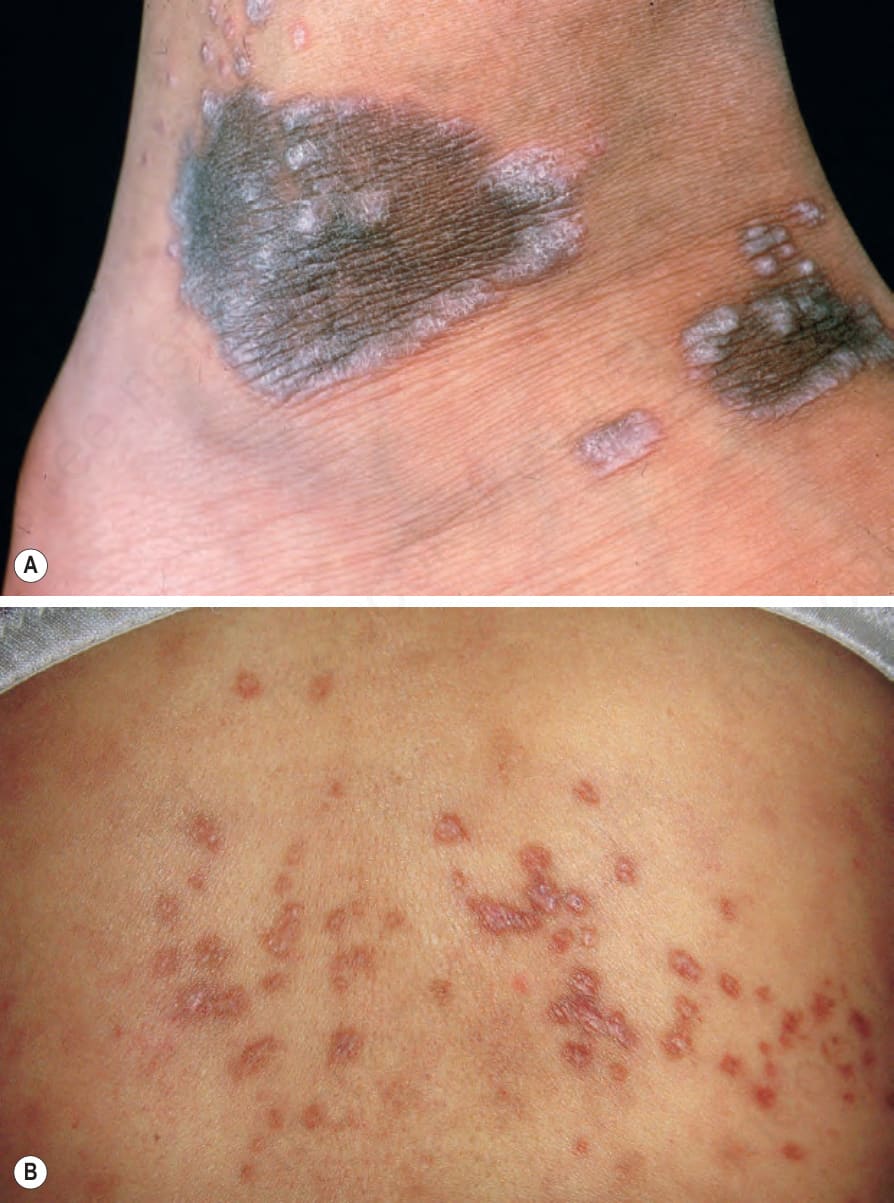
圖 7.2:Lichen planus:(A) 注意這些色素性病灶邊緣具有特徵性的 Wickham striae;(B) 在這些病灶上可見明顯的 Wickham striae,病灶出現於背部,是不常受影響的部位。(A) 來自已故 N.P. Smith 醫師的收藏,倫敦皮膚科研究所,英國。(B) 承蒙 J. Dayrit 醫師提供,馬尼拉,菲律賓。
Fig. 7.2 Lichen planus: (A) note the characteristic Wickham striae at the edge of these pigmented lesions; (B) Wickham striae are evident on these lesions, which have arisen on the back, an uncommonly affected site. (A) From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK. (B) Courtesy of J. Dayrit, MD, Manila, The Philippines.

圖 7.3:Lichen planus:前臂屈側 (flexor aspect) 有廣泛的雙側侵犯。來自已故 N.P. Smith 醫師的收藏,倫敦皮膚科研究所,英國。
Fig. 7.3 Lichen planus: there is extensive bilateral involvement of the flexor aspect of the forearms. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 7.4:Lichen planus:此蕾絲樣 (lacelike) 圖案具特徵性。來自已故 N.P. Smith 醫師的收藏,倫敦皮膚科研究所,英國。
Fig. 7.4 Lichen planus: this lacelike pattern is characteristic. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
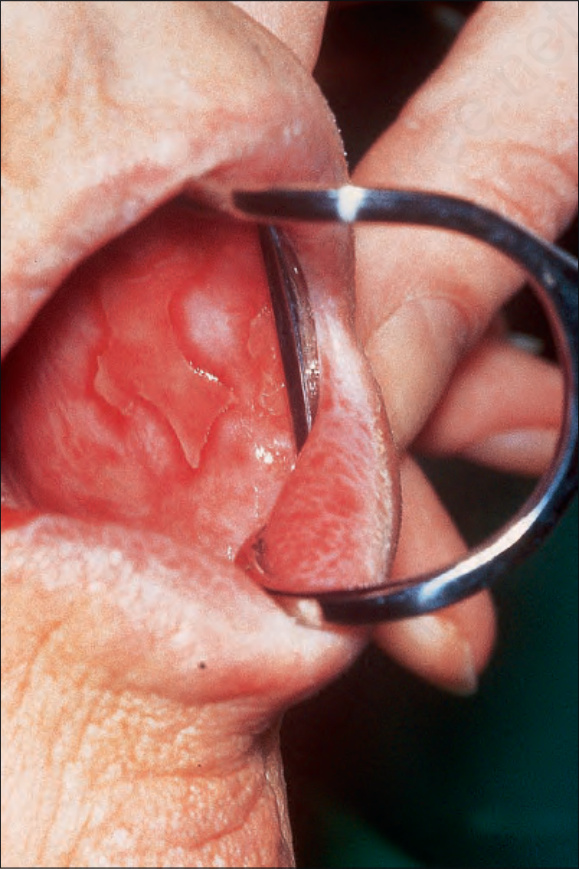
圖 7.5:Lichen planus:頰黏膜 (buccal mucosa) 有廣泛潰瘍。承蒙 R.A. Marsden 醫師提供,聖喬治醫院,倫敦,英國。
Fig. 7.5 Lichen planus: there is extensive ulceration of the buccal mucosa. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 7.6:Lichen planus:舌常受影響。承蒙 M. Blanes 醫師提供,阿利坎特,西班牙。
Fig. 7.6 Lichen planus: the tongue is commonly affected. By courtesy of M. Blanes, MD, Alicante, Spain

圖 7.7:Lichen planus:下唇上有一潰瘍性鱗狀細胞癌 (squamous carcinoma)。承蒙 R.A. Marsden 醫師提供,聖喬治醫院,倫敦,英國。
Fig. 7.7 Lichen planus: there is an ulcerated squamous carcinoma on the lower lip. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 7.8:Lichen planus:(A) 陰莖體 (shaft of the penis) 上有典型丘疹;(B) 注意外陰前庭 (vulval introitus) 與小陰唇 (labia minora) 周圍的紅斑性糜爛 (erythematous erosions)。(A) 來自已故 N.P. Smith 醫師的收藏,倫敦皮膚科研究所,英國;(B) 承蒙 S. Neill 醫師提供,倫敦皮膚科研究所,英國。
Fig. 7.8 Lichen planus: (A) typical papules are present on the shaft of the penis; (B) note the erythematous erosions around the vulval introitus and labia minora. (A) From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK; (B) By courtesy of S. Neill, MD, Institute of Dermatology, London, UK.

圖 7.9:Lichen planus:拇指甲有縱向脊狀化 (longitudinal ridging) 與條紋 (striation),甲褶 (nail folds) 有發炎性變化。來自已故 N.P. Smith 醫師的收藏,倫敦皮膚科研究所,英國。
Fig. 7.9 Lichen planus: there is longitudinal ridging and striation affecting the thumbnail, with inflammatory changes in the nail folds. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 7.10:Lichen planus:發炎後色素沉著 (postinflammatory hyperpigmentation) 是常見的表現。承蒙 R.A. Marsden 醫師提供,聖喬治醫院,倫敦,英國。
Fig. 7.10 Lichen planus: postinflammatory hyperpigmentation is a common manifestation. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 7.11:Lichen planopilaris:有特徵性的色素沉著毛囊性丘疹,在某些區域呈融合性。四肢常受影響。承蒙 R.A. Marsden 醫師提供,聖喬治醫院,倫敦,英國。
Fig. 7.11 Lichen planopilaris: there are characteristic hyperpigmented follicular papules, which are confluent in some areas. The limbs are commonly affected. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 7.12:Lichen planopilaris:明顯的發炎性變化,伴隨瘢痕形成與繼發性毛髮脫落。這些變化難以與假性禿髮 (pseudopélade) 及慢性盤狀紅斑性狼瘡 (chronic discoid lupus erythematosus) 區分。來自已故 N.P. Smith 醫師的收藏,倫敦皮膚科研究所,英國。
Fig. 7.12 Lichen planopilaris: marked inflammatory changes with scarring and secondary hair loss. These changes are difficult to distinguish from those of pseudopélade and chronic discoid lupus erythematosus. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
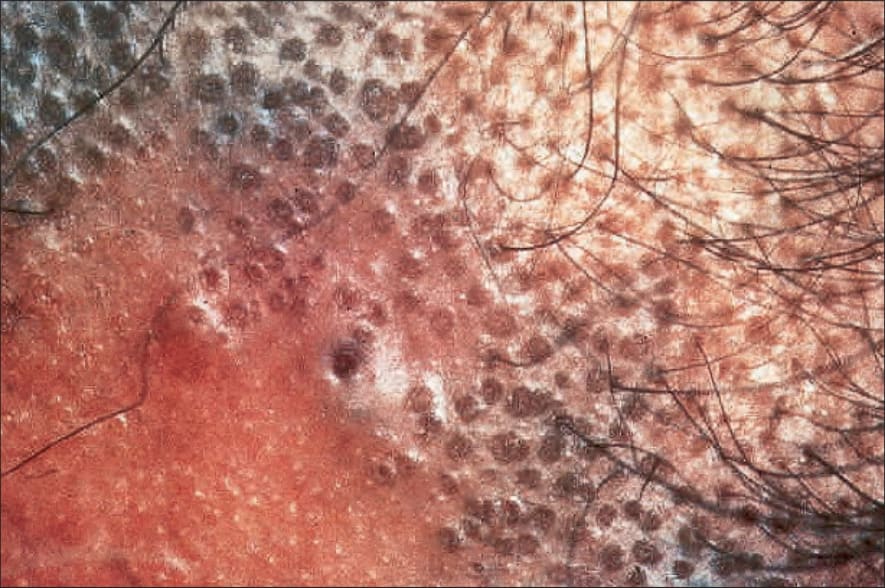
圖 7.13:Lichen planopilaris:在此患者身上可清楚看到濾泡性苔癬樣丘疹 (follicular lichenoid papules)。承蒙倫敦皮膚科研究所提供,英國。
Fig. 7.13 Lichen planopilaris: follicular lichenoid papules are clearly seen in this patient. By courtesy of the Institute of Dermatology, London, UK.

圖 7.14:Lichen planus actinicus:臉部有明顯色素沉著,代表發炎後變化。來自已故 N.P. Smith 醫師的收藏,倫敦皮膚科研究所,英國。
Fig. 7.14 Lichen planus actinicus: there is marked facial hyperpigmentation representing postinflammatory changes. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 7.15:Lichen planus pigmentosus:有融合性的色素性丘疹。來自已故 N.P. Smith 醫師的收藏,倫敦皮膚科研究所,英國。
Fig. 7.15 Lichen planus pigmentosus: there are coalescent pigmented papules. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
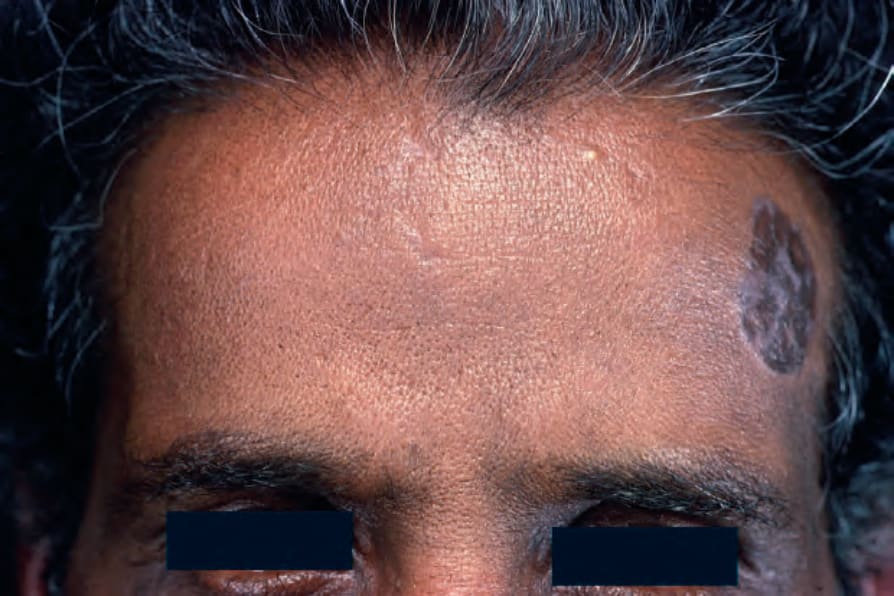
圖 7.16:Lichen planus pigmentosus:臉部是常受影響的部位。來自已故 N.P. Smith 醫師的收藏,倫敦皮膚科研究所,英國。
Fig. 7.16 Lichen planus pigmentosus: the face is a commonly affected site. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

圖 7.17:Hypertrophic lichen planus:一位老年男性脛部上有隆起、疣狀、紫羅蘭色的斑塊。這些病灶已存在 30 年。承蒙 R.A. Marsden 醫師提供,聖喬治醫院,倫敦,英國。
Fig. 7.17 Hypertrophic lichen planus: raised, warty, violaceous plaques on the shin of an elderly man. These lesions had been present for 30 years. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 7.18:Ulcerative lichen planus:此結痂潰瘍周圍的皮膚有明顯萎縮 (atrophy)。承蒙倫敦皮膚科研究所提供,英國。
Fig. 7.18 Ulcerative lichen planus: there is marked atrophy of the skin around this crusted ulcer. By courtesy of the Institute of Dermatology, London, UK.

圖 7.19:Ulcerative lichen planus:指(趾)常受影響。此變異型與鱗狀細胞癌 (squamous cell carcinoma) 風險的輕微增加有關。承蒙 R.A. Marsden 醫師提供,聖喬治醫院,倫敦,英國。
Fig. 7.19 Ulcerative lichen planus: the digits are often affected. This variant is associated with a slightly increased risk of squamous cell carcinoma. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
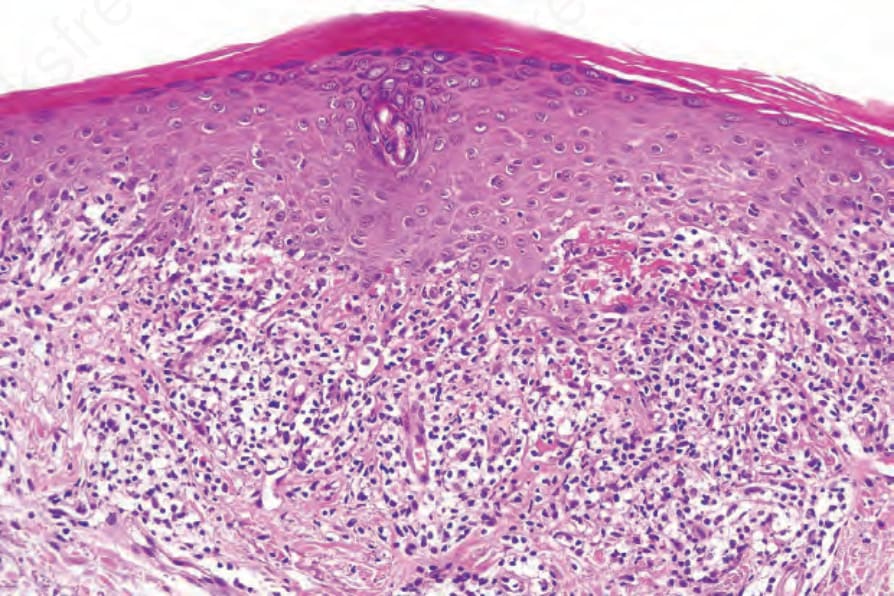
圖 7.23:Lichen planus:顆粒層增厚 (hypergranulosis) 明顯與汗管末端 (acrosyringium) 相關。有明顯的基底細胞液化變性 (basal cell liquefactive degeneration)。注意纖維蛋白 (fibrin) 沉積。
Fig. 7.23 Lichen planus: the hypergranulosis is clearly related to the acrosyringium. There is marked basal cell liquefactive degeneration. Note the fibrin deposition.
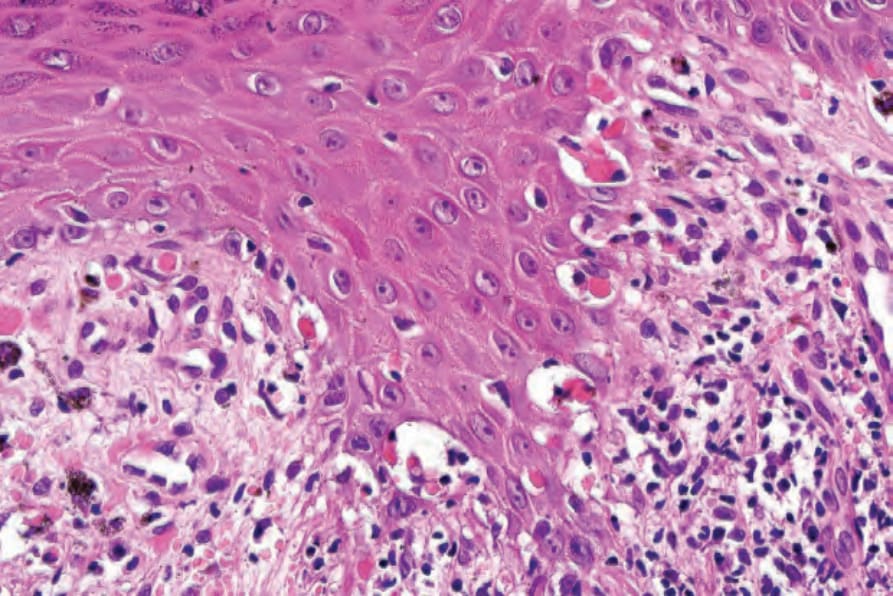
圖 7.25:Lichen planus:圖 7.24 的近觀,顯示基底細胞液化變性 (basal cell liquefactive degeneration) 與類細胞體 (cytoid bodies)。
Fig. 7.25 Lichen planus: close-up view of Fig. 7.24 showing basal cell liquefactive degeneration and cytoid bodies.
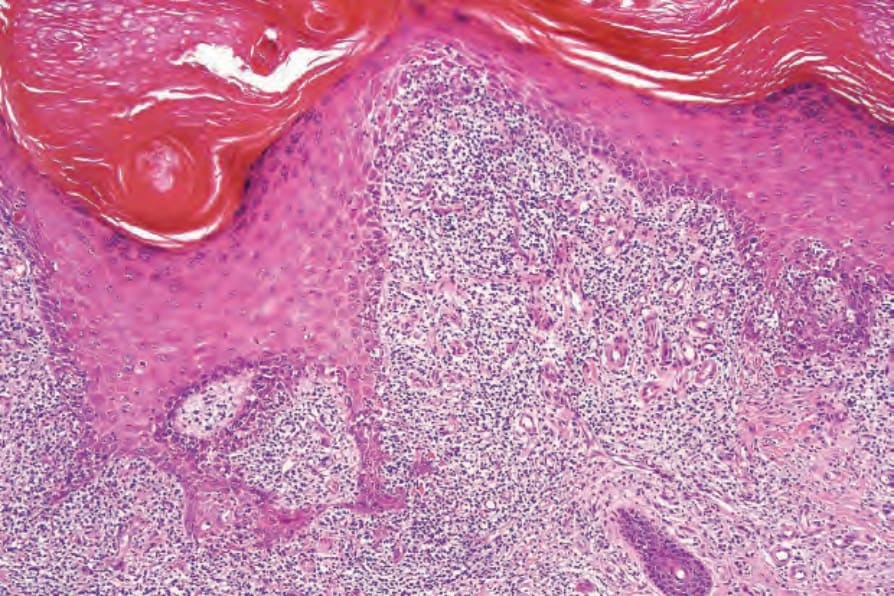
圖 7.32:Hypertrophic lichen planus:有非常明顯的不規則棘層肥厚 (irregular acanthosis)。注意顆粒層增厚 (hypergranulosis)。
Fig. 7.32 Hypertrophic lichen planus: there is very marked irregular acanthosis. Note the hypergranulosis.
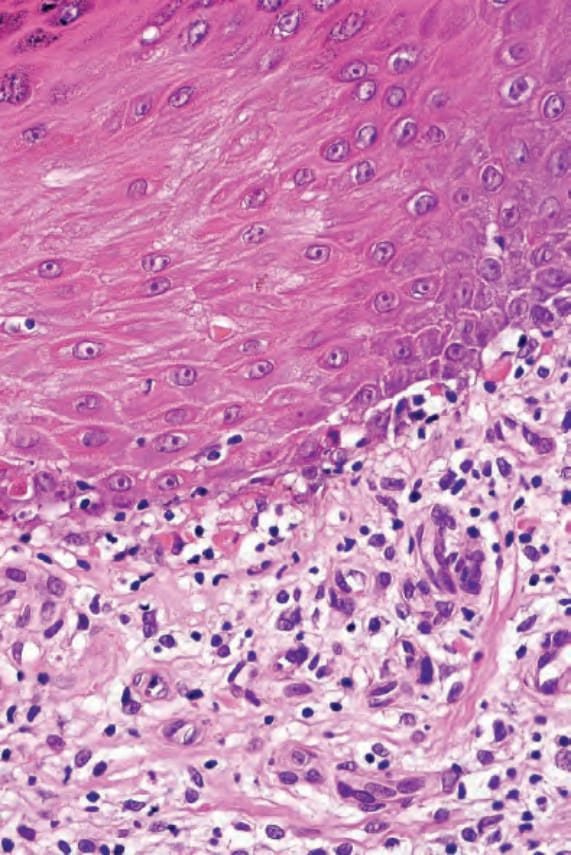
圖 7.33:Hypertrophic lichen planus:有基底細胞液化變性 (basal cell liquefactive degeneration) 與類細胞體 (cytoid bodies)。
Fig. 7.33 Hypertrophic lichen planus: there is basal cell liquefactive degeneration with cytoid bodies.

圖 7.38:Lichen nitidus:一位幼童的胸部上有許多微小的丘疹。承蒙 R.A. Marsden 醫師提供,聖喬治醫院,倫敦,英國。
Fig. 7.38 Lichen nitidus: numerous tiny papules are present on the chest of a young child. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
兒童扁平苔癬顯示輕度的男性優勢 (2 : 1)。雖然據說黏膜侵犯罕見,近期的系列研究報告其頻率為 14–39%。肥厚性病灶可見於高達 26% 的病例。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
扁平苔癬的病因不明。感染性(細菌與病毒)、自體免疫、代謝性、心身性與遺傳性病因的理論都曾有其支持者。然而,目前認為扁平苔癬代表對一種尚未確定的表皮新抗原 (epidermal neoantigen) 的異常遲發性過敏反應 (delayed hypersensitivity reaction),可能是對外來抗原與內源性自體抗原 (self-antigen) 結合的反應。扁平苔癬與多種病毒感染(包括 B 型與 C 型肝炎以及人類免疫缺乏病毒 [HIV])的關聯,加上與眾多藥物公認的關係,為此假說增添了支持。
扁平苔癬與多種肝細胞異常有關,包括異常的肝功能檢查與血清學。也曾記錄到慢性活動性肝炎 (chronic active hepatitis)、原發性硬化性膽管炎 (primary sclerosing cholangitis) 與原發性膽汁性肝硬化 (primary biliary cirrhosis) 的發生率增加。然而,並非所有已記錄的系列研究都證實這些觀察,這顯示所報告的關係可能取決於背景的 B 型肝炎病毒感染水準。扁平苔癬也曾接續疫苗接種而出現,最常見的是 B 型肝炎疫苗接種,但也包括流感、狂犬病與 Tdap 疫苗接種。較近期,扁平苔癬(特別是口腔疾病)被連結到 C 型肝炎病毒與慢性肝病。然而,扁平苔癬患者的 C 型肝炎病毒發生率變異極大,從某些國家(包括英國、印度、德國與斯洛維尼亞)實際上為零,到日本高達 100%。
扁平苔癬中也曾記錄到其他疾病的證據,包括甲狀腺疾病、血脂異常 (dyslipidemia),以及碳水化合物代謝受損(包括明顯的糖尿病 [diabetes mellitus]),特別是口腔變異型。近期一項來自日本的研究顯示,C 型肝炎感染可能與糖尿病及扁平苔癬兩者有關。其他研究則對其中部分關聯提出質疑。
多位作者已注意到扁平苔癬與人類白血球抗原 (human leukocyte antigen, HLA)-DR1、HLA-DQ1 與 HLA-DQB1 之間有顯著關聯。此關聯適用於有或無黏膜病灶的患者,但不延伸至藥物誘發的變異型。有人認為此關聯與 HLA-DR1+ 細胞向 T 輔助細胞 (T-helper cells) 呈現抗原,並由此導致自體免疫反應的發展有關。
雖然普遍接受扁平苔癬中基底細胞損傷的致病機轉主要涉及細胞免疫反應,可能透過第 I 型干擾素 (type I interferons) 的作用,增加 IP10/CXCR10 的表現,並經由 CXCR3 與 CCR5 招募 CD8+ T 細胞,
247 Lichenoid dermatoses
但確切的機轉仍需進一步闡明。自體抗體與免疫複合物 (immune complex) 介導的損傷不太可能在苔癬樣組織反應 (lichenoid tissue reaction) 中扮演重要角色。
扁平苔癬丘疹演變的起始事件是表皮基底層(角質細胞與黑色素細胞)的破壞。在發展的最早階段,表皮內存在數量增加的蘭格漢氏細胞 (Langerhans cells),咸信這些細胞處理經修飾的表皮抗原,以呈現給 T 淋巴球。角質細胞表現 HLA-DR,這可能具有致病重要性。隨後的遷移與由此產生的 CD8+ T 細胞活化,導致基底角質細胞死亡,乃因干擾素-γ (IFN-γ)、白介素 (IL)-6、顆粒球-巨噬細胞群落刺激因子 (GM-CSF) 與腫瘤壞死因子-α (TNF-α) 的綜合效應所致。基底角質細胞表現 FasR/FasL 顯示細胞凋亡 (apoptosis) 是扁平苔癬中重要的細胞死亡模式。真皮浸潤主要由 Ia+、CD4+ 淋巴球組成。CD8+ 淋巴球也存在,緊鄰真皮—表皮交界處 (dermal–epidermal junction),靠近基底角質細胞壞死的病灶,據說在早期病灶中占優勢。B 淋巴球稀少,且漿細胞 (plasma cells) 在皮膚病灶中典型缺如,肥厚性變異型除外。
典型丘疹的發展似乎是由於持續的角質細胞破壞與再生活動的綜合作用,後者取決於上皮從病灶邊緣與鄰近小汗腺導管 (eccrine ducts) 的遷移,而非有絲分裂活性的增加。在基底細胞損傷部位,氚標記胸苷 (tritiated thymidine) 的攝取很少,但在病灶邊緣攝取顯著;而作為再生的反映,keratin 17 的表現在基底上層 (suprabasal) 上皮也上調。因此,扁平苔癬的典型特徵取決於基底細胞液化變性 (basal cell liquefactive degeneration) 與不規則表皮再生之間不同程度的相互作用。
已成熟丘疹的特徵性組織學特徵通常可在掃描放大倍率下辨識(圖 7.21)。它們包括角化過度 (hyperkeratosis)、典型呈楔形 (wedge-shaped) 的顆粒層增厚 (hypergranulosis)(臨床上表現為 Wickham striae),與汗腺導管及毛囊的表皮內部分相關,以及不規則棘層肥厚 (irregular acanthosis)(圖 7.22 和 7.23)。棘層肥厚常呈鋸齒狀 (sawtooth) 外觀(圖 7.24 和 7.25)。顯著角化不全 (parakeratosis) 的存在強烈不支持皮膚扁平苔癬的診斷。表皮內有時可見淋巴球與組織球 (histiocytes),偶爾衛星細胞壞死 (satellite cell necrosis) 為一特徵。上皮基底層的液化變性具特徵性,且常存在表皮下裂隙 (subepidermal clefts)(Max Joseph 間隙)。色素失禁 (pigmentary incontinence) 常見(圖 7.26)。淋巴組織球性帶狀浸潤 (lymphohistiocytic bandlike infiltrate) 占據上層真皮,並遮蔽真皮—表皮交界處。可能存在偶見的嗜酸性球 (eosinophils)。在消退中的扁平苔癬,角化過度持續存在,但棘層肥厚消退,留下變平的表皮(圖 7.27);可能有局灶性瘢痕,且真皮浸潤較不明顯(圖 7.28)。
扁平苔癬中最早可辨識的變化是類細胞體 (cytoid bodies) 的存在與相關的色素失禁。類細胞體(膠樣體或 Civatte 體,colloid or Civatte bodies)是圓形或卵圓形、均質、嗜酸性的小體,可在基底上皮與真皮乳頭 (papillary dermis) 內辨識(圖 7.20)。它們呈現抗澱粉酶 (diastase-resistant) 的過碘酸希夫 (PAS) 陽性,可在丘疹、病灶周圍皮膚,甚至明顯未受侵犯的皮膚內辨識。雖然它們可見於多種皮膚病(包括紅斑性狼瘡、移植物抗宿主病 [graft-versus-host disease] 與皮膚異色症 [poikiloderma])以及看似正常的皮膚,但若其數量眾多或成簇出現,則提示扁平苔癬。
在超微結構上,類細胞體由緊密排列的絲狀物 (filaments) 聚集體組成,直徑 6–8 nm;免疫細胞化學上由角蛋白 (keratin) 組成。
病灶可能變得完全萎縮,組織學上表現為表皮變平、數量不等的膠樣體,以及色素失禁,幾乎沒有發炎。若膠樣體罕見,與皮膚異色症 (poikiloderma) 的區分可能非常困難。
248 Lichenoid and interface dermatitis
在環狀扁平苔癬 (annular lichen planus) 的病灶中,典型的組織學特徵僅見於病灶進展邊緣的周邊。
在微丘疹性扁平苔癬 (micropapular lichen planus) 中,變化非常局灶,以致若未檢查連續切片 (serial sections),可能漏失診斷。
毛囊扁平苔癬 (Lichen planopilaris) 在其早期階段顯示圍繞毛囊下部與毛乳頭 (papilla) 的浸潤、毛囊擴張,以及角質栓塞 (keratin plugging)(圖 7.29)。鄰近的毛囊間 (interfollicular) 上皮可能顯示或不顯示典型的苔癬樣浸潤(圖 7.30)。有時也明顯可見基底細胞水樣變性 (basal cell hydropic degeneration)、類細胞體形成與色素失禁。在進展期的頭皮病灶中,毛囊被破壞,並由垂直走向的纖維性瘢痕所取代,使人聯想到 Brocq 假性禿髮 (pseudopélade of Brocq) 中所見的纖維性條索 (fibrous streamers)。
汗孔扁平苔癬 (Lichen planoporitis) 是一種罕見的變異型,其苔癬樣/介面性變化以汗管末端 (acrosyringium) 與小汗腺汗管進入表皮處為中心。導管襯裡上皮的鱗狀化生 (squamous metaplasia) 可能為一特徵。
在光化性扁平苔癬 (lichen planus actinicus) 中,斑的環狀邊緣顯示扁平苔癬的典型特徵。然而,在病灶中央,上皮萎縮、變薄且變平,儘管淋巴組織球性浸潤仍然存在。也曾描述濾泡上皮 (follicular epithelium) 內
249 Lichenoid dermatoses
A
B
A
角化不全與濕疹化 (eczematization) 的病灶。有時可見點狀苔癬樣 (lichen nitidus-like) 病灶(見下文)。
色素性扁平苔癬 (Lichen planus pigmentosus) 的特徵為表皮變薄,伴隨基底細胞空泡化 (basal cell vacuolization)、色素失禁,以及淺層真皮的苔癬樣淋巴組織球性浸潤。
肥厚性扁平苔癬 (Hypertrophic lichen planus) 的特徵為更明顯的角化過度與棘層肥厚,上皮有時顯示假上皮瘤樣增生 (pseudoepitheliomatous hyperplasia),以致誤診為鱗狀細胞癌 (squamous cell carcinoma) 是一個明確的可能性,特別是在小活檢檢體中,且若無臨床資訊時(圖 7.31–7.33)。可觀察到若干在普通扁平苔癬中未見的變化,包括角化不全、海綿水腫 (spongiosis)、基底細胞層上方的壞死角質細胞、更頻繁的嗜酸性球,以及真皮浸潤中的漿細胞。這些變化可能引起苔癬樣藥物疹 (lichenoid drug eruption) 的可能性。鑑別診斷不困難,因為苔癬樣藥物疹傾向較為廣泛,且通常不伴隨肥厚性變化。
B
扁平苔癬的口腔病灶雖然常顯示典型特徵,但通常顯示角化不全;偶爾兩者交替的病灶皆明顯可見。與皮膚病灶相對,上皮有時相當薄,且鋸齒狀 (sawtooth) 圖案不明顯(圖 7.34)。典型有基底細胞水樣變性。由於富含纖維蛋白的嗜酸性無定形物質沉積,常存在基底膜增厚 (basement membrane thickening)。細胞浸潤除了淋巴球與組織球外,常含有漿細胞。可見發育異常 (dysplasia)。
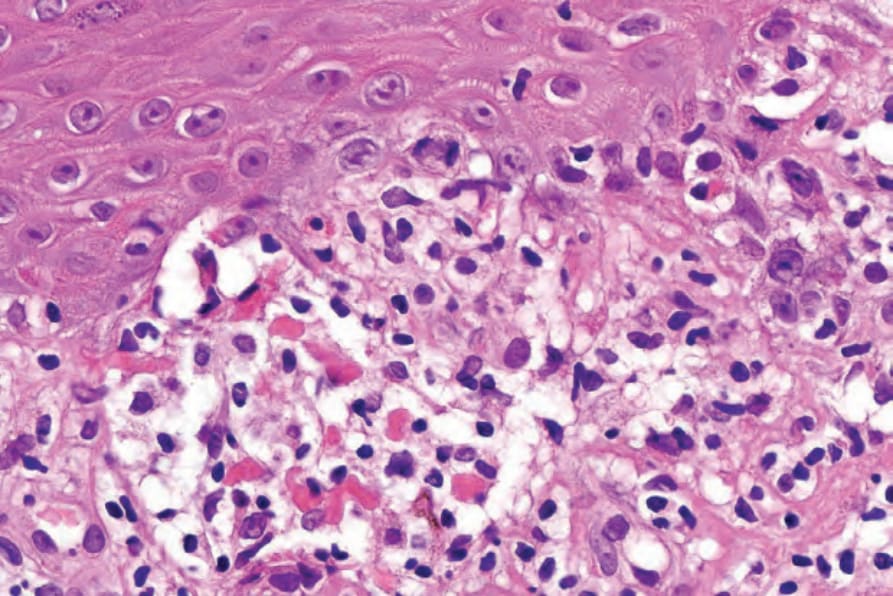
圖 7.20:Lichen planus:此視野顯示特徵性的嗜酸性類細胞體 (eosinophilic cytoid bodies),伴隨基底細胞液化變性 (basal cell liquefactive degeneration) 與淋巴組織球性浸潤。
Fig. 7.20 Lichen planus: this view shows characteristic eosinophilic cytoid bodies associated with basal cell liquefactive degeneration and a lymphohistiocytic infiltrate.
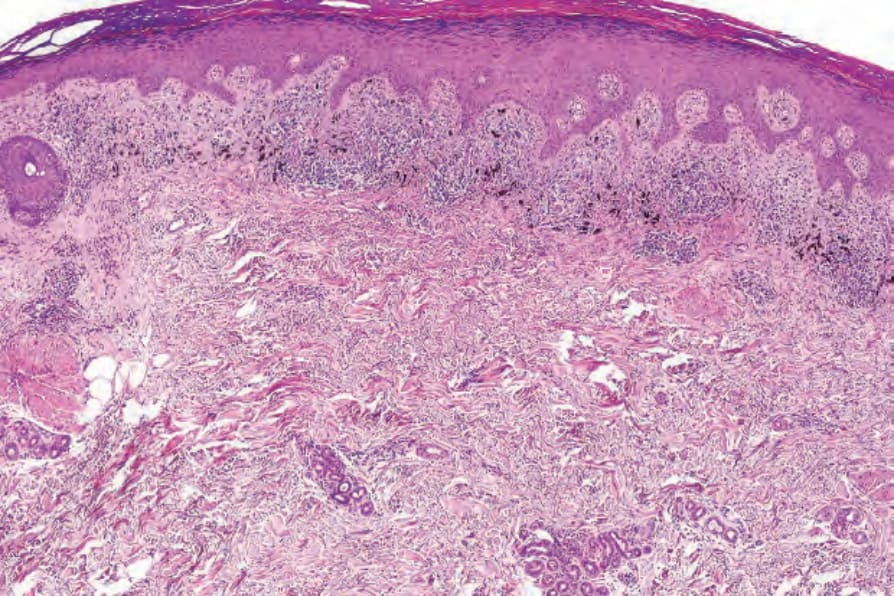
圖 7.21:Lichen planus:此掃描視野具特徵性,凸顯出角化過度 (hyperkeratosis)、顆粒層增厚 (hypergranulosis) 與不規則棘層肥厚 (irregular acanthosis)。注意典型的帶狀發炎細胞浸潤與色素失禁。
Fig. 7.21 Lichen planus: this scanning view is characteristic and highlights the hyperkeratosis, hypergranulosis, and irregular acanthosis. Note the typical bandlike inflammatory cell infiltrate and pigment incontinence.
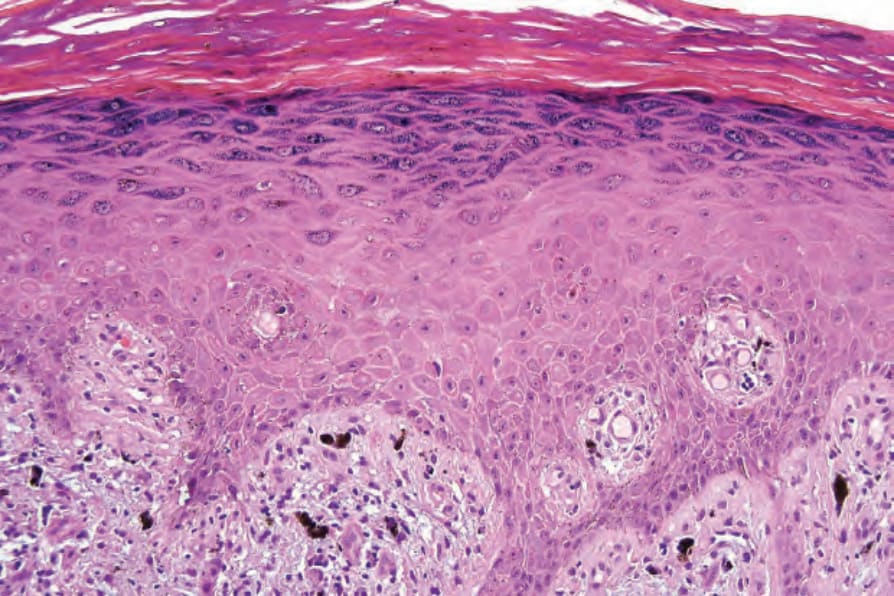
圖 7.22:Lichen planus:注意角化過度 (hyperkeratosis)、顆粒層增厚 (hypergranulosis) 與不規則棘層肥厚 (irregular acanthosis)。
Fig. 7.22 Lichen planus: note the hyperkeratosis, hypergranulosis, and irregular acanthosis.
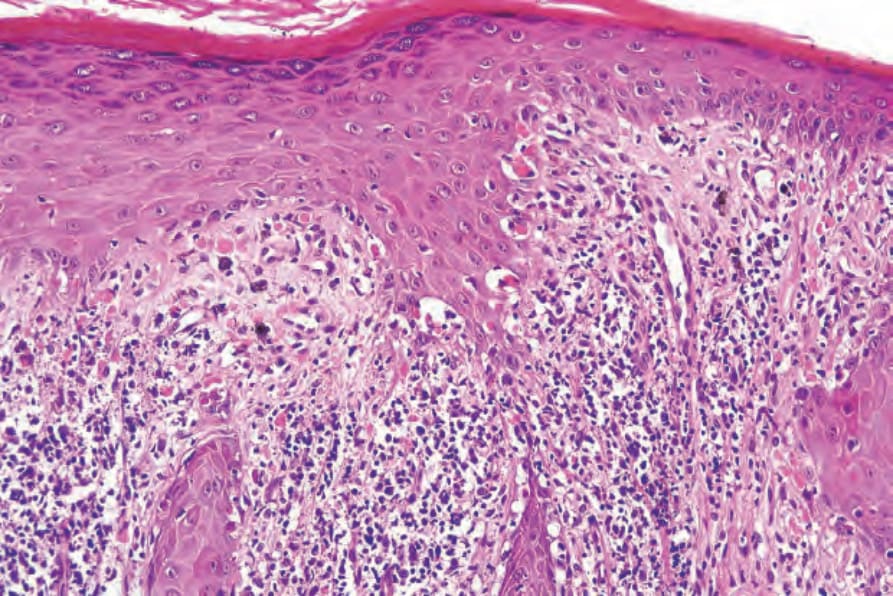
圖 7.24:Lichen planus:棘層肥厚 (acanthosis) 不規則,常呈鋸齒狀 (sawtooth) 外觀。
Fig. 7.24 Lichen planus: the acanthosis is irregular and often has a sawtooth appearance.
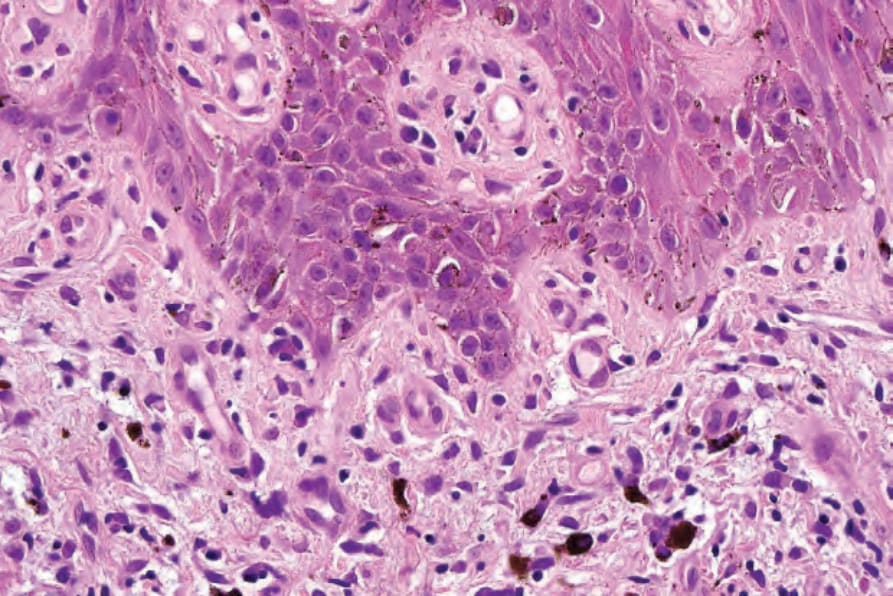
圖 7.26:Lichen planus:黑色素 (melanin) 存在於巨噬細胞 (macrophages) 內(色素失禁,pigmentary incontinence)。
Fig. 7.26 Lichen planus: melanin pigment is present within macrophages (pigmentary incontinence).
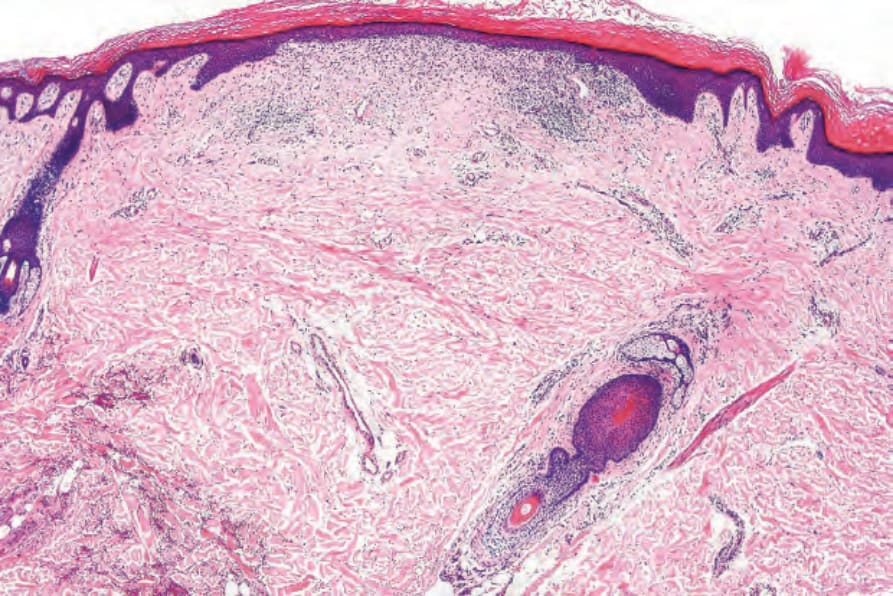
圖 7.27:萎縮性(消退中)扁平苔癬 (Atrophic (resolving) lichen planus):有角化過度、表皮變平,以及輕微的殘餘淋巴組織球性浸潤。
Fig. 7.27 Atrophic (resolving) lichen planus: there is hyperkeratosis, epidermal flattening, and a slight residual lymphohistiocytic infiltrate.
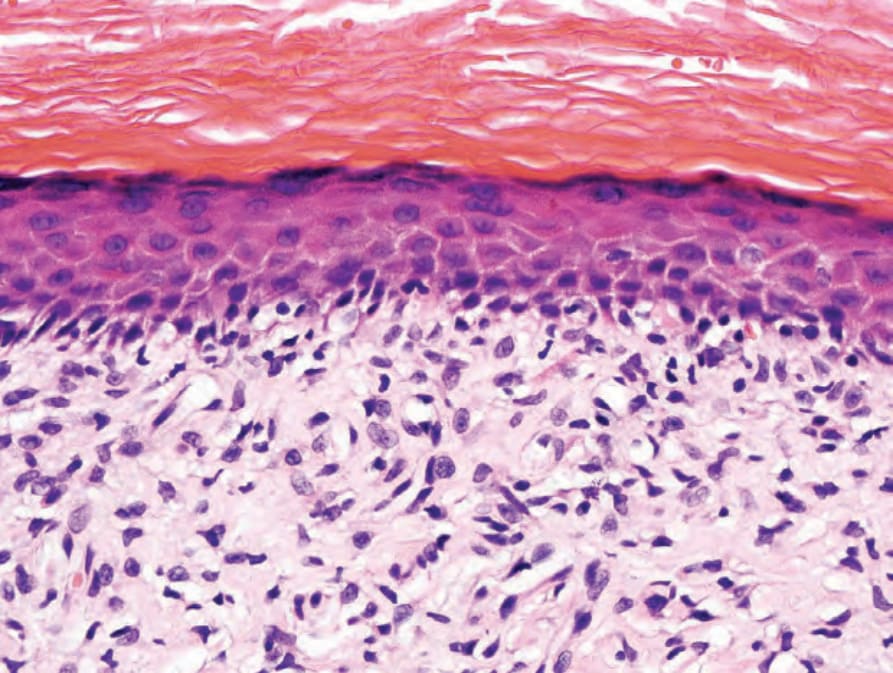
圖 7.28:萎縮性(消退中)扁平苔癬 (Atrophic (resolving) lichen planus):除了淋巴組織球性浸潤外,還有過多數量的纖維母細胞 (fibroblasts) 與增加的真皮乳頭膠原蛋白 (papillary dermal collagen)。
Fig. 7.28 Atrophic (resolving) lichen planus: in addition to the lymphohistiocytic infiltrate, there are excessive numbers of fibroblasts and increased papillary dermal collagen.
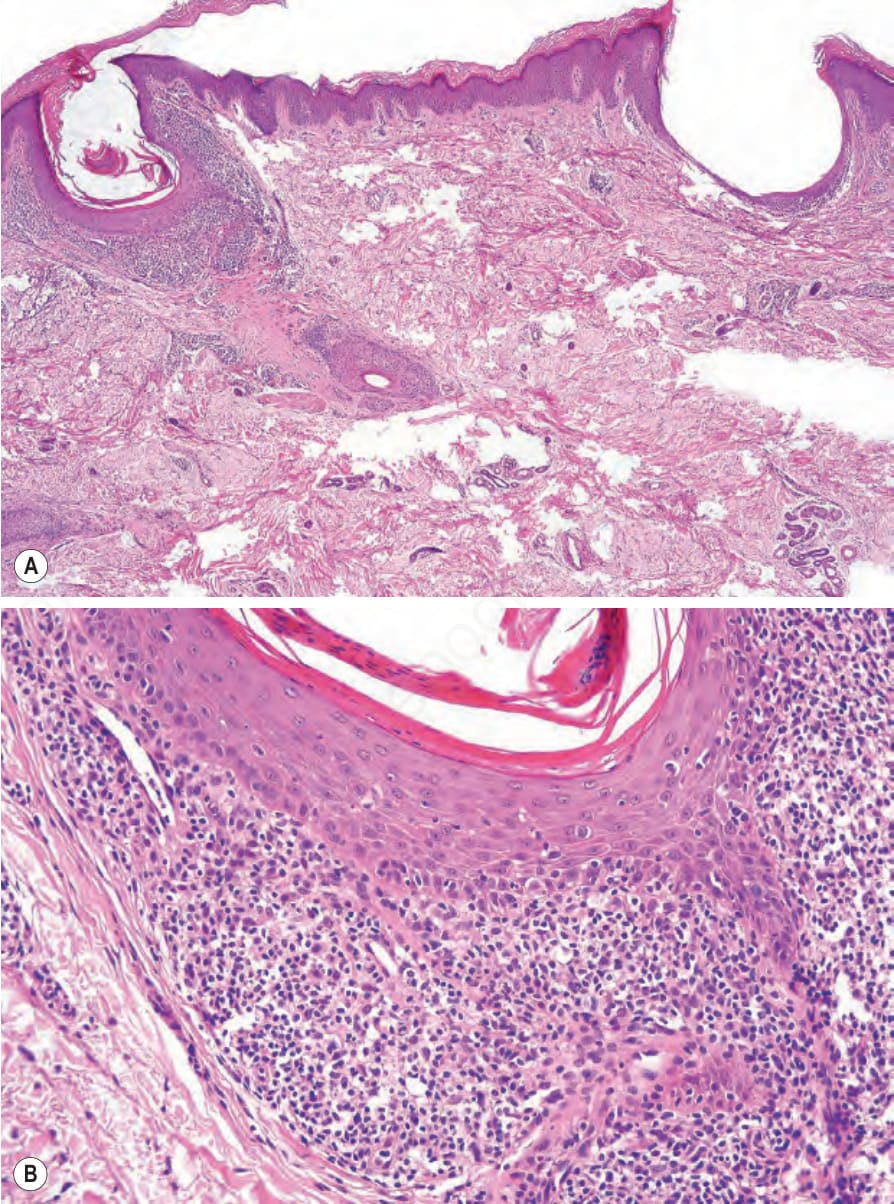
圖 7.29:Lichen planopilaris:(A, B) 有明顯的毛囊擴張與栓塞,伴隨帶狀的以毛囊為中心 (folliculocentric) 的浸潤。此患者表現為瘢痕性禿髮,且身體其他部位有典型扁平苔癬病灶。
Fig. 7.29 Lichen planopilaris: (A, B) there is marked follicular dilatation and plugging accompanied by a bandlike folliculocentric infiltrate. This patient presented with scarring alopecia and typical lichen planus lesions elsewhere.
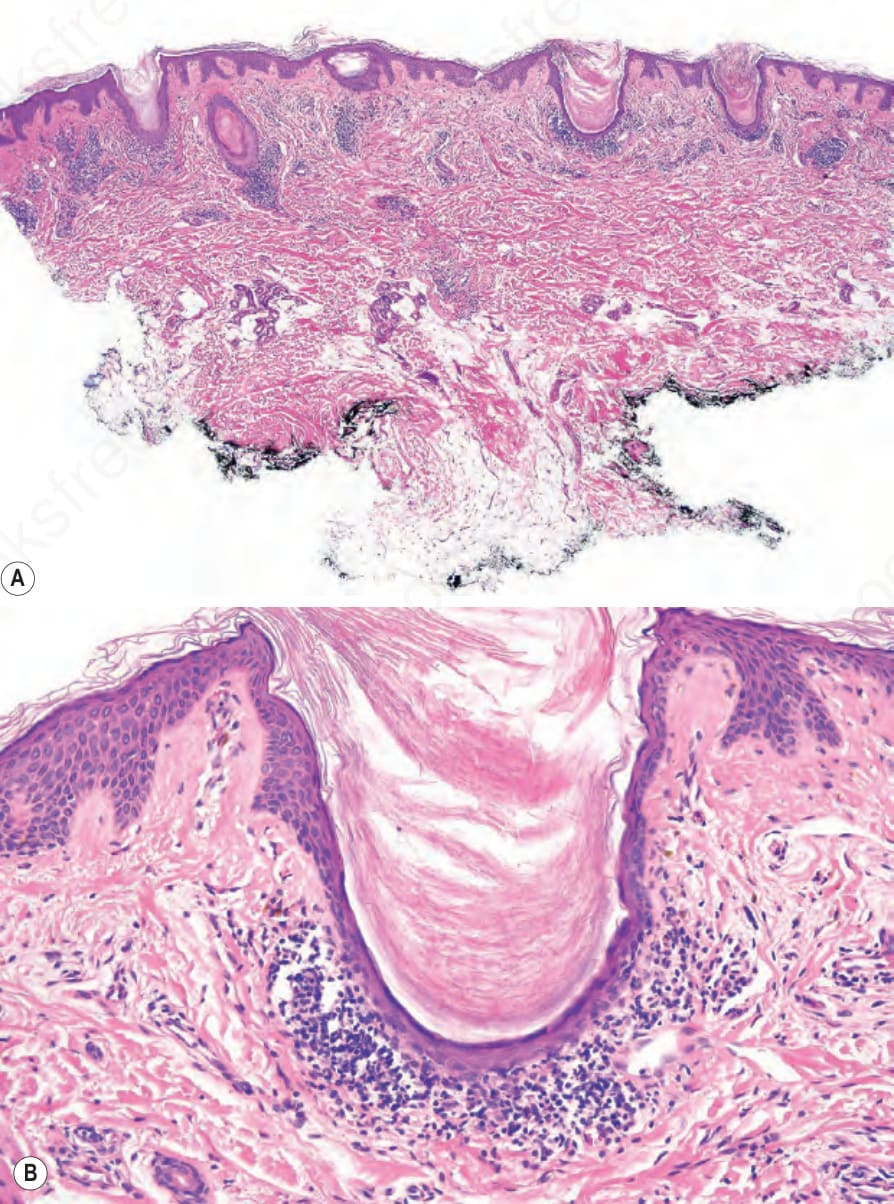
圖 7.30:Lichen planopilaris:(A, B) 有顯著的以毛囊為中心 (folliculocentric) 的帶狀浸潤,伴隨角質栓塞 (keratin plugging)。毛囊間表皮未受影響。
Fig. 7.30 Lichen planopilaris: (A, B) there is a strikingly folliculocentric bandlike infiltrate associated with keratin plugging. The interfollicular epidermis is unaffected.
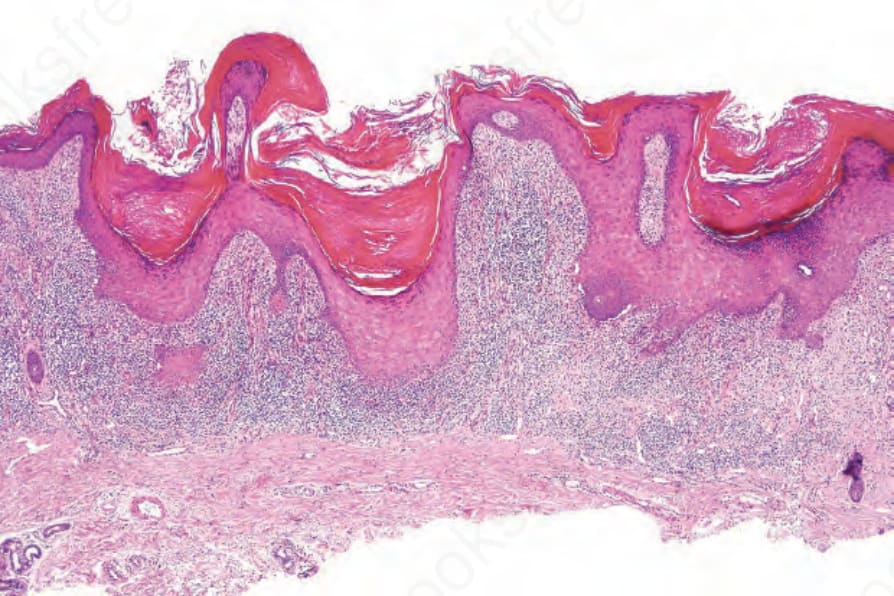
圖 7.31:Hypertrophic lichen planus:注意角化過度、局灶性楔形顆粒層增厚 (focal wedge-shaped hypergranulosis)、非常明顯的不規則棘層肥厚,以及淺層緻密的帶狀浸潤。
Fig. 7.31 Hypertrophic lichen planus: note the hyperkeratosis, focal wedge-shaped hypergranulosis, very marked irregular acanthosis, and superficial dense bandlike infiltrate.
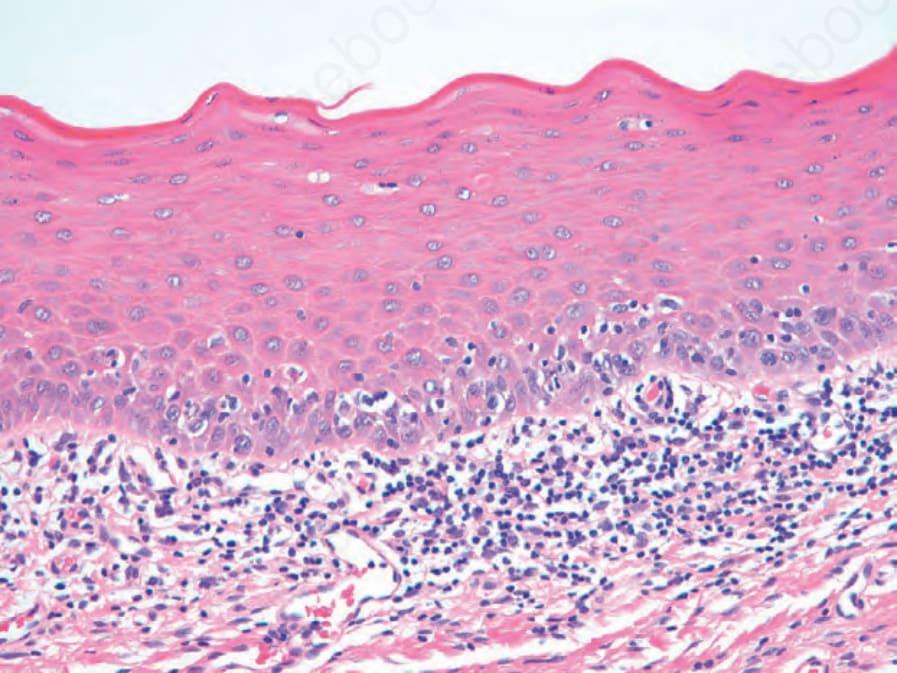
圖 7.34:口腔扁平苔癬 (Oral lichen planus):有角化不全、微妙的顆粒層,且與皮膚扁平苔癬相對,上皮—上皮下交界處 (epithelial–subepithelial junction) 無鋸齒狀化 (sawtoothing)。
Fig. 7.34 Oral lichen planus: there is parakeratosis, a subtle granular layer, and no sawtoothing of the epithelial–subpithelial junction in contrast to cutaneous lichen planus.
250 Lichenoid and interface dermatitis
與皮膚侵犯不同,食道病灶顯示角化不全。通常可見不同程度的上皮萎縮及/或輕度增厚,且棘層肥厚的鋸齒狀圖案並非一個特徵。如同口腔病灶,漿細胞常伴隨淋巴球性浸潤。
水疱性或大疱性病灶為表皮下 (subepidermal),因伴隨基底膜帶 (basement membrane zone) 損傷(使基底細胞水樣變性複雜化)而發展出過度水腫所致(圖 7.35)。
扁平苔癬患者的直接免疫螢光 (direct immunofluorescence) 研究通常顯示真皮—表皮交界處有一條線狀纖維狀 (linear fibrillar) 的纖維蛋白 (fibrin) 帶(圖 7.36)。類細胞體可能被非特異性地凸顯,主要對 IgM,但也對 IgG、IgA 與 C3(圖 7.37)。一種存在於棘細胞層 (prickle cell) 與顆粒細胞層的扁平苔癬「特異性抗原」(lichen planus ‘specific antigen’),已透過以患者血清對胎兒皮膚進行間接免疫螢光 (indirect immunofluorescence) 而被證實。其致病意義不明。毛囊扁平苔癬 (Lichen planopilaris) 的直接免疫螢光顯示毛囊性、線狀的基底膜帶以免疫球蛋白(主要為 IgG 或 IgA)標記。也可能存在纖維蛋白。此觀察的分類學 (nosological) 意涵尚不確定。針對循環中抗基底膜帶抗體的間接免疫螢光為陰性。
鑑別診斷 (Differential Diagnosis)
扁平苔癬應與其他顯示苔癬樣浸潤及上皮基底層水樣變性的疾病區分。因此,扁平苔癬可能與苔癬樣角化症 (lichenoid keratosis) 無法區分,兩者的區分完全取決於臨床病理相關性 (clinicopathological correlation)。在許多苔癬樣角化症的病例中,有其他相關的變化,包括局灶性海綿水腫 (focal spongiosis) 與角化不全 (parakeratosis)。萎縮性病灶可能與皮膚異色症 (poikiloderma) 及慢性盤狀紅斑性狼瘡 (chronic discoid lupus erythematosus) 混淆。扁平苔癬樣 (lichen planus-like) 型態是慢性
251 Lichenoid dermatoses
移植物抗宿主病 (graft-versus-host disease, GVHD) 早期階段的典型表現,但此實體的浸潤密度通常較低。
皮膚異色症 (Poikiloderma) 顯示表皮萎縮,伴隨表皮突 (ridge) 圖案的喪失,且無鋸齒狀外觀的傾向。在那些與蕈狀肉芽腫 (mycosis fungoides) 相關的例子中,苔癬樣浸潤含有數量不等的非典型淋巴球。
慢性盤狀紅斑性狼瘡 (Chronic discoid lupus erythematosus) 伴隨表皮萎縮與毛囊栓塞 (follicular plugging)。發炎細胞浸潤呈斑塊狀,傾向於附屬器周圍 (periappendageal) 位置,並伴隨真皮黏蛋白 (mucin) 沉積。陽性的狼瘡帶試驗 (lupus band test) 可能有幫助。
扁平苔癬可能輕易被誤認為苔癬樣藥物反應 (lichenoid drug reaction),特別是在缺乏臨床資訊的情況下。支持後者的組織學特徵
包括高層次的類細胞體 (high-level cytoid bodies) 與真皮浸潤中頻繁的嗜酸性球。
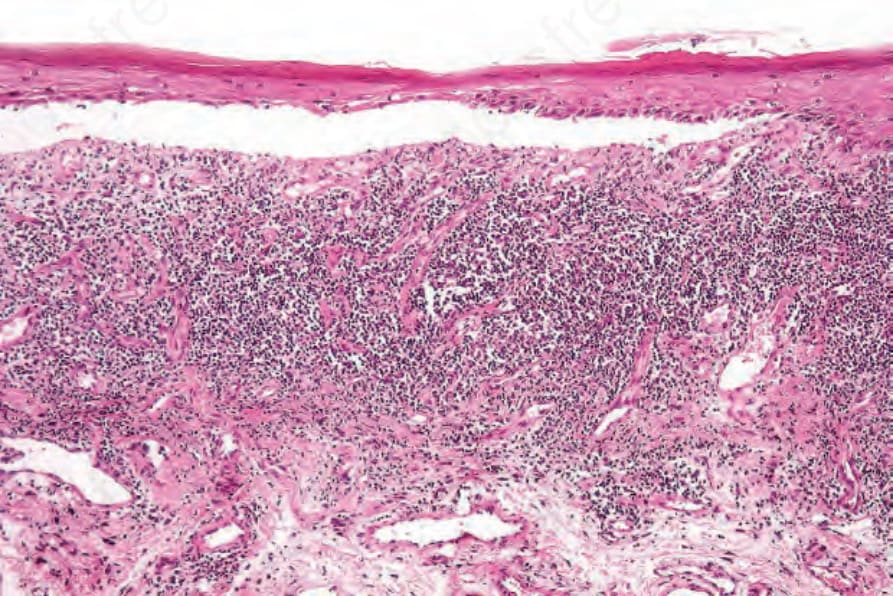
圖 7.35:大疱性扁平苔癬 (Bullous lichen planus):口腔病灶顯示鱗狀上皮與固有層 (lamina propria) 的分離。注意帶狀浸潤。
Fig. 7.35 Bullous lichen planus: oral lesion showing separation of the squamous epithelium from the lamina propria. Note the bandlike infiltrate.
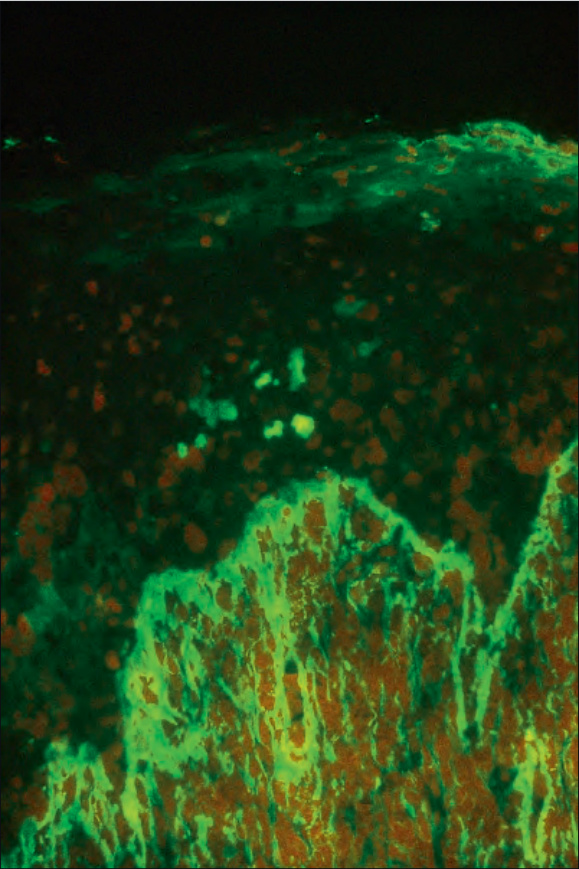
圖 7.36:Lichen planus:亮綠色螢光顯示纖維蛋白 (fibrin) 的存在。承蒙倫敦皮膚科研究所免疫螢光部門提供,英國。
Fig. 7.36 Lichen planus: brilliant green fluorescence indicates the presence of fibrin. By courtesy of the Department of Immunofluorescence, Institute of Dermatology, London, UK.
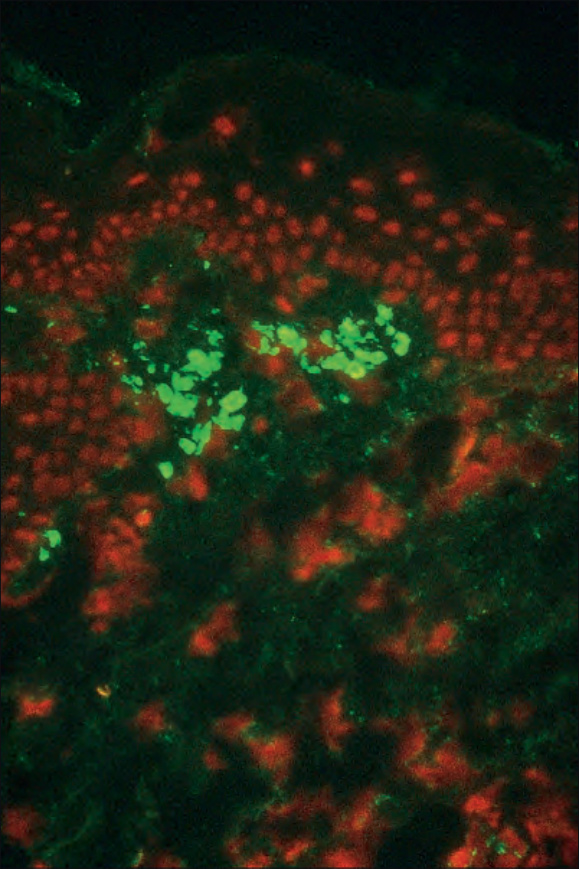
圖 7.37:Lichen planus:類細胞體 (cytoid bodies) 對 IgM 呈陽性標記。承蒙倫敦皮膚科研究所免疫螢光部門提供,英國。
Fig. 7.37 Lichen planus: cytoid bodies labeled positively for IgM. By courtesy of the Department of Immunofluorescence, Institute of Dermatology, London, UK.