Lichen planus
Lichen planus
Clinical features Lichen planus (Gr. leichen, tree moss) is a common, usually intensely pruritic, symmetrical, papulosquamous dermatosis.1,2 Its prevalence in the general population is approximately 1%, and it most often presents in the fourth to sixth decades with a slight female predominance.3,4 It is uncommon in childhood.5,6 Occasional familial cases have been reported.7,8
The disease is characterized by small, smooth, shiny, flat-topped polygonal papules measuring several millimeters to 1 cm in diameter and often having a violaceous color (Fig. 7.1). Delicate white lines known as Wickham striae typically cross the slightly scaly surface (Fig. 7.2). The lesions are found most commonly on the flexor aspect of the wrists, the forearms, the extensor aspect of the hands and ankles, the lumbar area, and the glans penis (Fig. 7.3). Rare cases may also have associated palmoplantar keratoderma.9,10 Annular lesions may be seen. Lichen planus is associated with a positive Koebner phenomenon. It is a usually self-limiting although sometimes protracted disorder, patients clearing of lesions within weeks to 1 or 2 years.
Ocular involvement is rare and may include eyelid lesions, blepharitis, conjunctivitis, keratitis, punctate corneal opacities, iridocyclitis, and chorioretinitis.29,30
Esophageal involvement, although rare, is an important potential cause of morbidity and is the most frequently involved gastrointestinal site.31 Concomitant oral lesions are typically present, but in rare cases esophageal involvement is the initial presentation.32 To date, middle-aged or elderly females are typically affected.32–36 Complications include chronic dysphagia and stricture formation affecting the mid or upper esophagus.32,33,37–40 Patients with esophageal lichen planus may have a risk of developing squamous cell carcinoma.31,33,35,36,41,42 Some patients may develop squamous cell carcinoma associated with esophageal lichen planus in the absence of oral or cutaneous manifestations.43 The role of surveillance is uncertain.
Oral involvement, which is very common (affecting up to 60% of patients with cutaneous disease), shows a marked female preponderance and presents most often in the seventh decade. It may sometimes be the sole manifestation (an estimated 15–35% of patients with oral lichen planus never develop skin lesions).11–17 The buccal mucosa, vestibule, tongue, gingivae, hard palate, fornix, lip, and soft palate may be affected, in decreasing order of frequency.14,15 Patients frequently present with a white lacelike pattern,
Genital lesions in lichen planus are common (particularly in males), being present in up to 25% of patients, and sometimes adopting an annular configuration (Fig. 7.8).1 Similar annular lichen planus may be found elsewhere on the body, including intertriginous areas.44 Occasionally, penile lesions are the sole expression of the disease, and there is an association in uncircumcised men.45,46 Vulval lesions may be found in up to 51% of females with cutaneous involvement.47 Sometimes gingival and female genital lesions may coexist as a variant of erosive lichen planus, the so-called vulvovaginal-gingival syndrome.48–51 Patients present with dyspareunia and intense burning vulval pain. The vulva appears congested, and there may be erosions, which are often surrounded by a white reticulate border. Vaginal involvement similarly presents as dyspareunia and often postcoital bleeding due to inflammatory, desquamative, and erosive changes. More typical features of lichen planus may be encountered elsewhere on the body. Squamous
242 Lichenoid and interface dermatitis
carcinoma is an important complication, albeit rare, of chronic vulval lichen planus and appears to be more common in nonhair-bearing mucosa.52,53 The development of penile cancer is rare.54 Genital involvement in lichen planus is discussed elsewhere (see Chapter 12).
The nails are affected in about 10% of patients with lichen planus; manifestations include thinning of the nail plate, longitudinal ridging, striations, pterygium formation, subungual hyperkeratosis, and, very rarely, complete destruction of the nail (Fig. 7.9).1 Although nail involvement in children is said to be rare, some authors regard twenty-nail dystrophy of childhood as a variant of localized lichen planus, although not all accept this hypothesis.55–59
Most lesions heal within 6–18 months of onset. However, oral and hypertrophic variants and lichen planopilaris tend to have a chronic course.
Box 7.1 Causes of lichenoid dermatitis
• Lichen planus
• Lichenoid graft-versus-host disease
• Lichen nitidus
• Lichenoid keratosis
• Lichenoid drug reaction
• Fixed drug reaction
• Lichen planopilaris
• Lichen striatus
• Adult Blaschkitis
• Lichen aureus
• Lichenoid mycosis fungoides
• Ashy dermatoses
• Lichenoid and granulomatous dermatitis
A
Box 7.2 Causes of interface dermatitis
• Lichenoid dermatoses (see Box 7.1)
• Erythema multiforme
• Stevens-Johnson syndrome/toxic epidermal necrolysis
• Connective tissue disorders: lupus erythematosus, dermatomyositis, and mixed connective tissue disorders
• Graft-versus-host disease
• Poikiloderma including those related to rare inherited disorders
• Interface drug reactions
• Interface viral exanthem
• Pityriasis lichenoides
B
243 Lichenoid dermatoses
Postinflammatory hyperpigmentation is not uncommon, particularly in darker-skinned people (Fig. 7.10).
A number of variants of lichen planus merit specific mention:
• Lichen planopilaris (follicular lichen planus) presents as single or multiple plaques of scarring alopecia associated with a spectrum of lesions including typical lichenoid papules involving the scalp to brown or violaceous keratotic follicular papules affecting the trunk and extremities (Figs 7.11–7.13).61–63 Nonscarring plaques with prominent follicular papules may also be present. Linear lesions have rarely been described.64–66 Some authors suggest that scalp lichen planus results in some cases of pseudopélade of Brocq, although that entity likely represents the end stage of a variety of scarring alopecias.67–69 Children
can also be affected.70,71 The Graham-Little-Picardi-Lasseur syndrome refers to a variant of lichen planopilaris characterized by the following triad: 1. multifocal scarring alopecia of the scalp; 2. nonscarring alopecia of the axilla and groin; 3. follicular lichen planus of other areas of the body, scalp, or both.
• Atrophic lichen planus, the clinical features of which merely reflect resolution of the more typical active phase.
• Lichen planus actinicus [lichen planus subtropicus, summertime actinic lichenoid eruption (SALE)] develops in patients with prolonged exposure to sunlight and, therefore, usually manifests in spring or summer,72–76 with improvement or remission in the autumn or winter. It occurs particularly in the Middle East (especially Egypt) and the Far
244 Lichenoid and interface dermatitis
A
B
of variably pruritic pigmented dark brown macules predominantly affecting exposed skin and the flexures (Figs 7.15 and 7.16). The most common affected sites include the face and neck, but intertriginous areas may also be affected (lichen planus pigmentosus inversus).77–83 There is no sex predilection. The disorder is characterized by periods of exacerbation and remission.4 Exceptionally, involvement of the oral mucosa has been documented.5
• Hypertrophic lichen planus, which represents superimposed lichen simplex chronicus, commonly affects the lower limbs, particularly the shins, and manifests as highly pigmented warty plaques (Fig. 7.17).84 Often, involvement is restricted to the shins with no other lesions elsewhere. Familial lichen planus shows an increased incidence of this variant.85 The lesions are intensely itchy and very persistent. There is an attendant (albeit very slight) risk of neoplastic transformation.86–88
• Ulcerative lichen planus, a chronic variant affecting the fingers, hands, soles, and toes, is often associated with permanent loss of nails (Figs 7.18 and 7.19). Squamous cell carcinoma may complicate this variant of lichen planus.89,90
East and affects younger people, with a maximum incidence in the second and third decades and a slight female predominance (Fig. 7.14). Affected sites include the lateral aspects of the forehead, the dorsum of the hands, the forearms, face, and neck. The eruption can include a mixture of lichen planus-like and lichen nitidus-like lesions, whereas in others, the lesions appear as purely one or the other (see actinic lichen nitidus, below). Typically, the lichen planus lesions have an annular configuration with a bluish-brown, rather atrophic center and slightly raised border. They may sometimes coalesce to form circinate plaques. Occasionally, a melasma-like appearance has been documented.76 There is usually little pruritus, and Koebner phenomenon is commonly absent. The nails are often unaffected.
• Lichen planus pigmentosus, most commonly encountered in the tropics in dark-skinned patients, is characterized by the development
245 Lichenoid dermatoses
Other variants include lichen planus linearis, which occurs predominantly in children, and the rare vesicular or bullous variants, which must be distinguished from lichen planus pemphigoides. Bullous lichen planus implies the development of vesicles or bullae on preexistent lichenoid lesions as a consequence of severe basal cell hydropic degeneration. It is more often a histologic finding rather than a clinical observation. In contrast, lichen planus pemphigoides is characterized by the development of large tense bullae arising on normal or erythematous skin in a patient with typical lichen planus elsewhere. It represents the combined expression of lichen planus and bullous pemphigoid.91,92
246 Lichenoid and interface dermatitis

Fig. 7.1 Lichen planus: there are typical flat-topped polygonal papules on dorsum of the hand. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
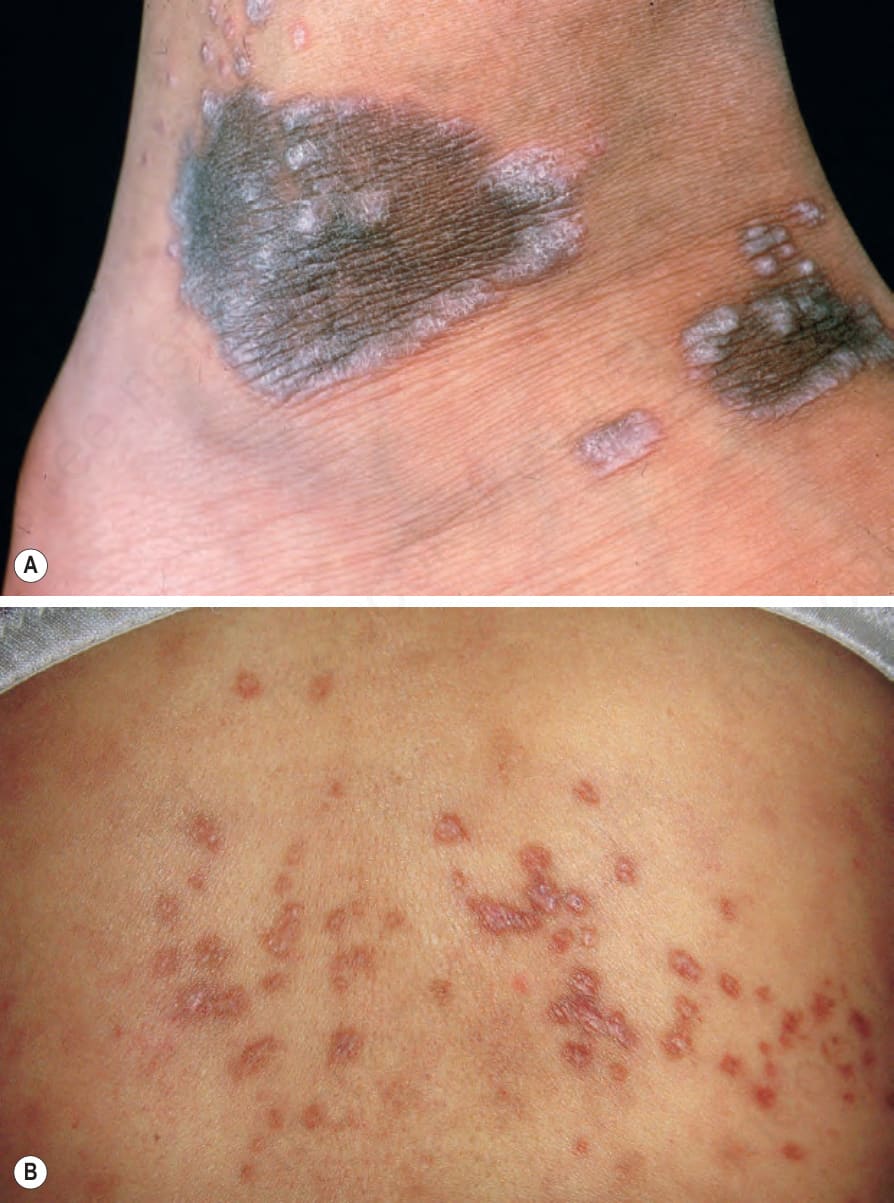
Fig. 7.2 Lichen planus: (A) note the characteristic Wickham striae at the edge of these pigmented lesions; (B) Wickham striae are evident on these lesions, which have arisen on the back, an uncommonly affected site. (A) From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK. (B) Courtesy of J. Dayrit, MD, Manila, The Philippines.

Fig. 7.3 Lichen planus: there is extensive bilateral involvement of the flexor aspect of the forearms. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 7.4 Lichen planus: this lacelike pattern is characteristic. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
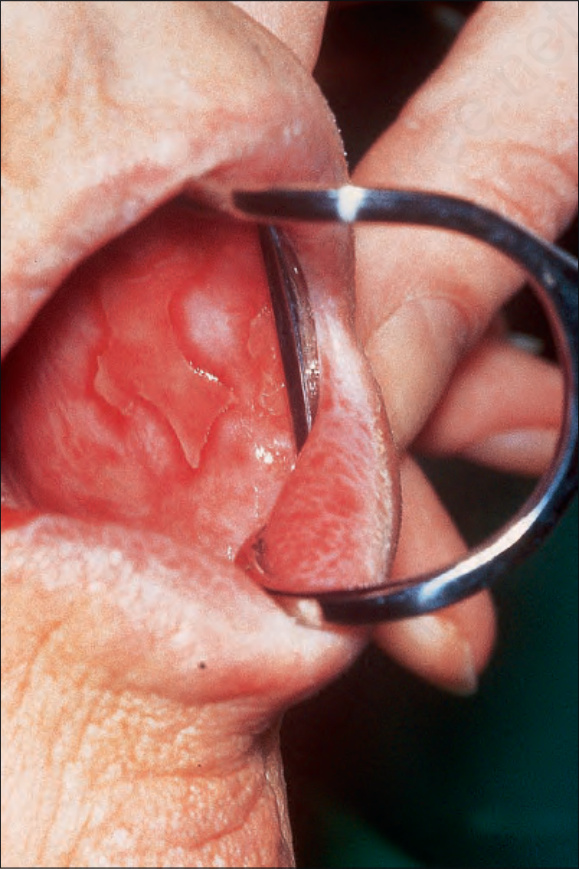
Fig. 7.5 Lichen planus: there is extensive ulceration of the buccal mucosa. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 7.6 Lichen planus: the tongue is commonly affected. By courtesy of M. Blanes, MD, Alicante, Spain

Fig. 7.7 Lichen planus: there is an ulcerated squamous carcinoma on the lower lip. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 7.8 Lichen planus: (A) typical papules are present on the shaft of the penis; (B) note the erythematous erosions around the vulval introitus and labia minora. (A) From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK; (B) By courtesy of S. Neill, MD, Institute of Dermatology, London, UK.

Fig. 7.9 Lichen planus: there is longitudinal ridging and striation affecting the thumbnail, with inflammatory changes in the nail folds. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 7.10 Lichen planus: postinflammatory hyperpigmentation is a common manifestation. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 7.11 Lichen planopilaris: there are characteristic hyperpigmented follicular papules, which are confluent in some areas. The limbs are commonly affected. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 7.12 Lichen planopilaris: marked inflammatory changes with scarring and secondary hair loss. These changes are difficult to distinguish from those of pseudopélade and chronic discoid lupus erythematosus. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
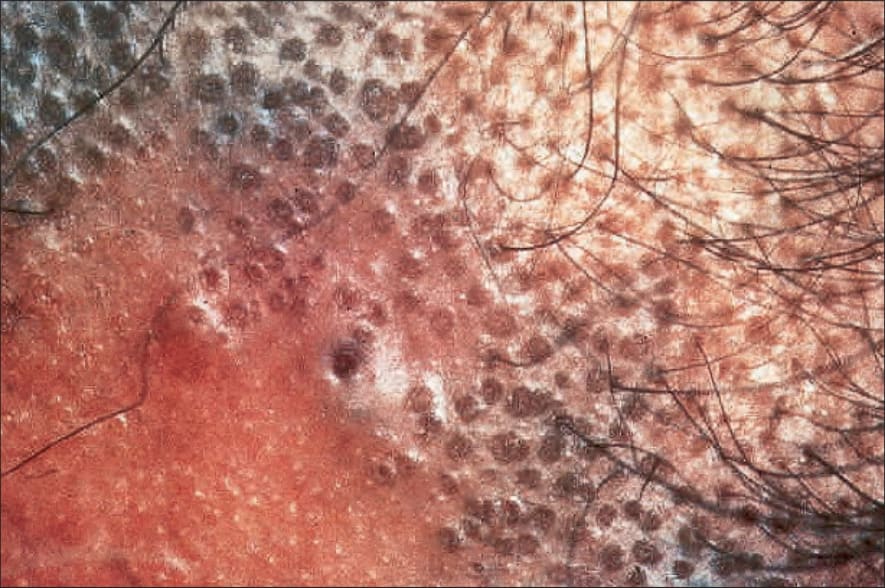
Fig. 7.13 Lichen planopilaris: follicular lichenoid papules are clearly seen in this patient. By courtesy of the Institute of Dermatology, London, UK.

Fig. 7.14 Lichen planus actinicus: there is marked facial hyperpigmentation representing postinflammatory changes. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 7.15 Lichen planus pigmentosus: there are coalescent pigmented papules. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.
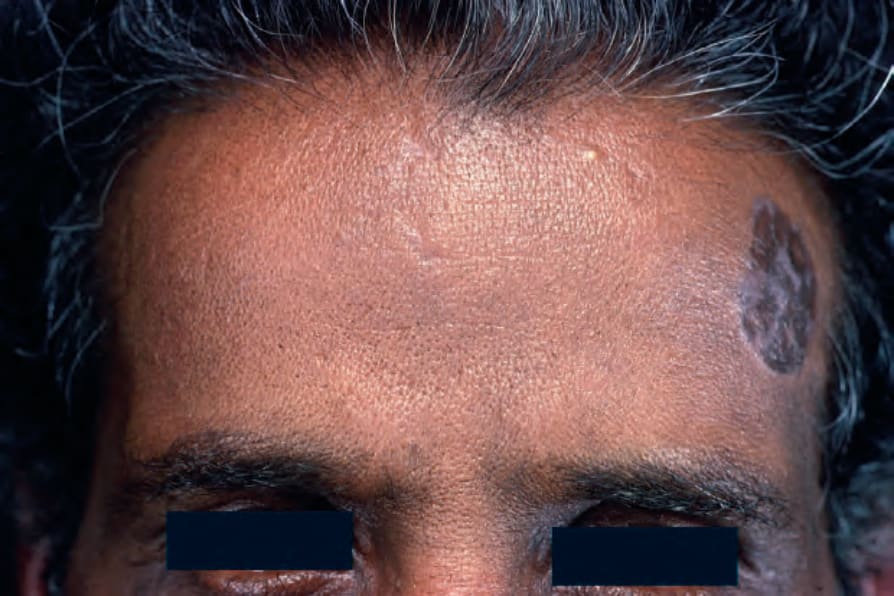
Fig. 7.16 Lichen planus pigmentosus: the face is a commonly affected site. From the collection of the late N.P. Smith, MD, the Institute of Dermatology, London, UK.

Fig. 7.17 Hypertrophic lichen planus: raised, warty, violaceous plaques on the shin of an elderly man. These lesions had been present for 30 years. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 7.18 Ulcerative lichen planus: there is marked atrophy of the skin around this crusted ulcer. By courtesy of the Institute of Dermatology, London, UK.

Fig. 7.19 Ulcerative lichen planus: the digits are often affected. This variant is associated with a slightly increased risk of squamous cell carcinoma. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
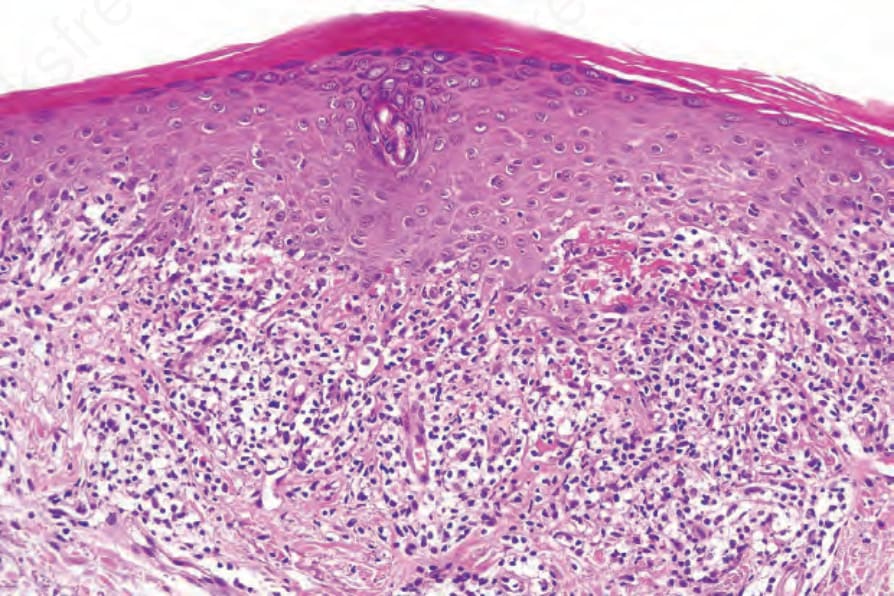
Fig. 7.23 Lichen planus: the hypergranulosis is clearly related to the acrosyringium. There is marked basal cell liquefactive degeneration. Note the fibrin deposition.
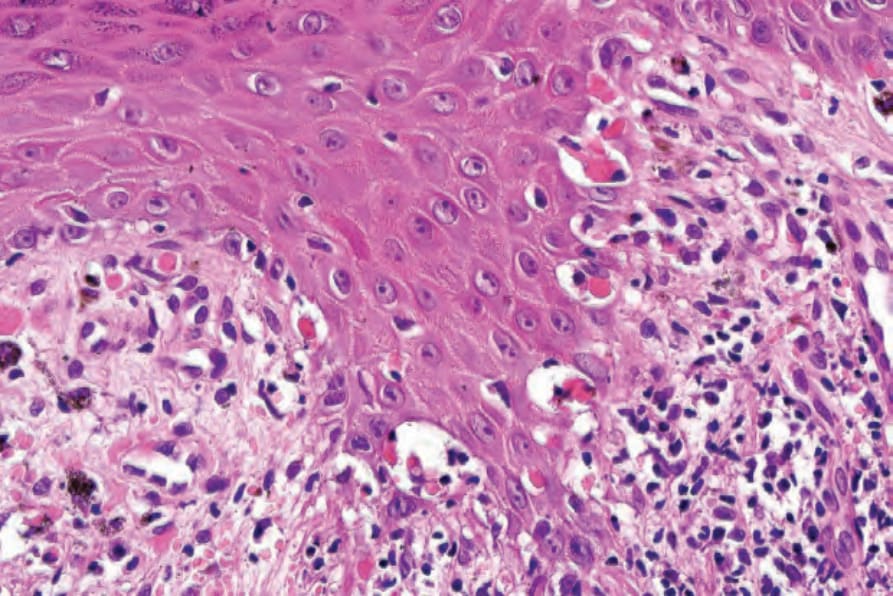
Fig. 7.25 Lichen planus: close-up view of Fig. 7.24 showing basal cell liquefactive degeneration and cytoid bodies.
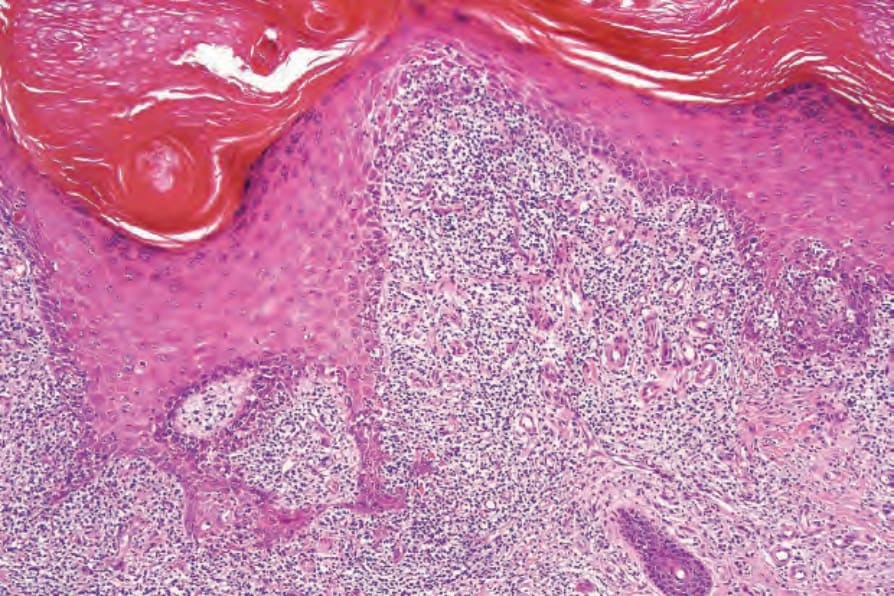
Fig. 7.32 Hypertrophic lichen planus: there is very marked irregular acanthosis. Note the hypergranulosis.
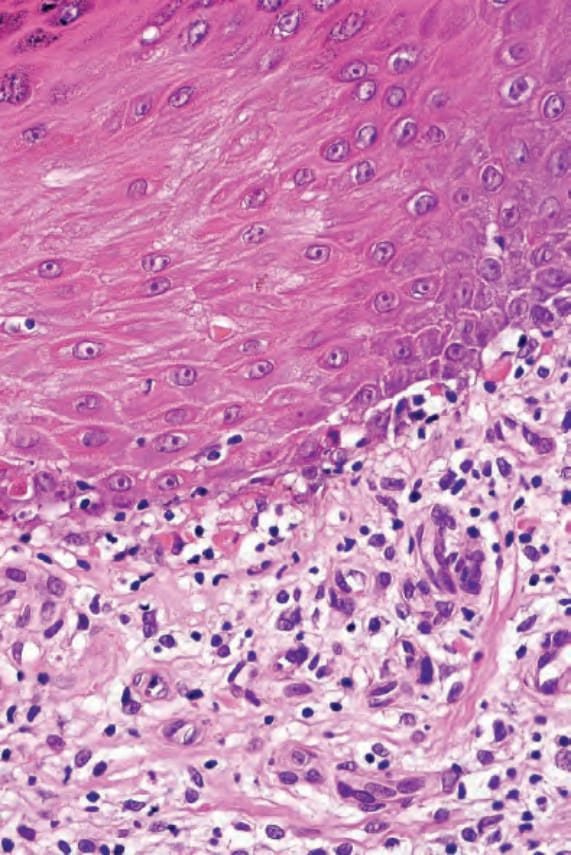
Fig. 7.33 Hypertrophic lichen planus: there is basal cell liquefactive degeneration with cytoid bodies.

Fig. 7.38 Lichen nitidus: numerous tiny papules are present on the chest of a young child. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
Childhood lichen planus shows a modest male predominance (2 : 1).5,6,61,78 Although mucosal involvement is said to be rare, recent series report a frequency of 14–39%.6,70,93 Hypertrophic lesions may be seen in up to 26% of cases.6
Pathogenesis and histologic features The etiology of lichen planus is unknown. Theories of infectious (bacterial and viral), autoimmune, metabolic, psychosomatic, and genetic causes have all had their proponents. Currently, however, it is thought that lichen planus represents an abnormal delayed hypersensitivity reaction to an as yet undetermined epidermal neoantigen, possibly to a combination of an external antigen coupled with an internal self-antigen.94–96 The association of lichen planus with a number of viral infections including hepatitis B and C and human immunodeficiency virus (HIV), combined with the well-recognized relationship to numerous drugs, adds support to this hypothesis.97–99
Lichen planus is associated with a variety of liver cell abnormalities including aberrant liver function tests and serology.100,101 An increased incidence of chronic active hepatitis, primary sclerosing cholangitis and primary biliary cirrhosis has also been recorded.102–107 Not all documented series, however, have confirmed these observations, suggesting that the reported relationship may be dependent on the background level of hepatitis B virus infection.105 Lichen planus has also followed vaccination, most commonly hepatitis B vaccination but also influenza, rabies, and Tdap vaccination.108–114 More recently, lichen planus (particularly oral disease) has been linked to hepatitis C virus and chronic liver disease. The incidence of hepatitis C virus in patients with lichen planus is, however, very variable, ranging from effectively zero in some countries, including the United Kingdom, India, Germany, and Slovenia, to as high as 100% in Japan.115–121
Evidence of other disorders including thyroid disease, dyslipidemia, and impaired carbohydrate metabolism including overt diabetes mellitus, has also been documented in lichen planus, particularly the oral variant.122–131 A recent study from Japan suggests a possible association of hepatitis C infection with both diabetes and lichen planus.129 Other studies have cast doubt on some of these associations.132
A significant association between lichen planus and human leukocyte antigen (HLA)-DR1, HLA-DQ1, and HLA-DQB1 has been noted by a number of authors.133–140 This association pertains to patients with or without mucosal lesions but does not extend to patients with the drug-induced variant. It is suggested that this association relates to antigen presentation by HLA-DR1+ cells to T-helper cells with the resultant development of an autoimmune response.133
Although it is generally accepted that the pathogenesis of the basal cell damage in lichen planus primarily involves the cellular immune response, likely through the action of type I interferons increasing the expression of IP10/CXCR10 and recruiting CD8+ T cells via CXCR3 and CCR5,141–143
247 Lichenoid dermatoses
the precise mechanism(s) require further elucidation. It is unlikely that autoantibody and immune complex-mediated damage have a significant role in the lichenoid tissue reaction.94,95
The initial event in the evolution of the lichen planus papule is destruction of the basal epidermal layer (keratinocytes and melanocytes).144,145 In the earliest stage of development, increased numbers of Langerhans cells are present within the epidermis, and it is believed that these cells process modified epidermal antigens for presentation to T lymphocytes.146,147 Keratinocytes express HLA-DR, and this is likely to be of pathogenetic importance. Subsequent migration with resultant CD8+ T-cell activation results in basal keratinocyte death due to the combined effects of interferon-gamma (IFN- γ), interleukin (IL)-6, granulocyte-macrophage colony stimulating factor (GM-CSF), and tumor necrosis factor alpha (TNF-α).97–99,141–143,148 The expression of FasR/FasL by the basal keratinocytes suggests that apoptosis is an important mode of cell death in lichen planus.149 The dermal infiltrate consists predominantly of Ia+, CD4+ lymphocytes.146,150 CD8+ lymphocytes are also present in close apposition to the dermal–epidermal junction adjacent to foci of basal keratinocyte necrosis and are said to predominate in early lesions.148,150–152 B lymphocytes are scarce and plasma cells are characteristically absent in cutaneous lesions, except in the hypertrophic variant.
Development of the typical papule appears to be due to a combination of continued keratinocyte destruction and regenerative activity, with the latter depending upon the migration of epithelium from the edge of the lesion and from adjacent eccrine ducts, rather than from increased mitotic activity. There is little uptake of tritiated thymidine at the site of basal cell damage, but conspicuous uptake at the edges of the lesion and, as a reflection of regeneration, keratin 17 expression is also upregulated in the suprabasal epithelium.153 The typical features of lichen planus therefore depend upon a variable interplay between basal cell liquefactive degeneration and irregular epidermal regeneration.
Characteristic histologic features of an established papule can usually be recognized at scanning magnification (Fig. 7.21). They comprise hyperkeratosis, typically wedge-shaped hypergranulosis (clinically presenting as Wickham striae) related to the intraepidermal components of sweat ducts and hair follicles, and irregular acanthosis (Figs 7.22 and 7.23). The acanthosis often has a sawtooth appearance (Figs 7.24 and 7.25). The presence of prominent parakeratosis argues strongly against a diagnosis of cutaneous lichen planus. Lymphocytes and histiocytes may sometimes be seen in the epidermis and occasionally satellite cell necrosis is a feature. Liquefactive degeneration of the basal layer of the epithelium is characteristic and often subepidermal clefts are present (Max Joseph spaces). Pigmentary incontinence is common (Fig. 7.26). A lymphohistiocytic bandlike infiltrate occupies the upper dermis and obscures the dermal–epidermal junction. Occasional eosinophils may be present.154 Hyperkeratosis persists in resolving lichen planus, but the acanthosis regresses, leaving a flattened epidermis (Fig. 7.27); there may be focal scarring and the dermal infiltrate is less conspicuous (Fig. 7.28).
The earliest identifiable change in lichen planus is the presence of cytoid bodies and associated pigmentary incontinence. Cytoid bodies (colloid or Civatte bodies) are round or oval, homogeneous, eosinophilic bodies identifiable within the basal epithelium and the papillary dermis (Fig. 7.20). They display diastase-resistant periodic acid-Schiff (PAS) positivity, and may be identified within papules, perilesional skin, and even apparently uninvolved skin. Although they may be seen in a variety of dermatoses (including lupus erythematosus, graft-versus-host disease, and poikiloderma) and seemingly normal skin, where their presence, if either in large numbers or in a cluster, suggests lichen planus.
Ultrastructurally, cytoid bodies are composed of tightly arranged aggregates of filaments 6–8 nm in diameter; immunocytochemically they are composed of keratin.
Lesions may become completely atrophic and histologically there is flattening of the epidermis, variable number of colloid bodies, and pigment incontinence with almost no inflammation. If colloid bodies are rare, distinction from poikiloderma may be very difficult.
248 Lichenoid and interface dermatitis
In lesions of annular lichen planus, the typical histologic features are only seen in the periphery at the advancing edge of the lesion.
In micropapular lichen planus, the changes are so focal that the diagnosis may be missed if serial sections are not examined.
Lichen planopilaris in its early stages shows an infiltrate surrounding the lower hair follicle and papilla, follicular dilatation, and keratin plugging (Fig. 7.29).60,62 The adjacent interfollicular epithelium may or may not show a typical lichenoid infiltrate (Fig. 7.30). Basal cell hydropic degeneration, cytoid body formation, and pigmentary incontinence are also sometimes evident. In advanced scalp lesions, the hair follicles are destroyed and replaced by vertically orientated fibrous scars, reminiscent of the fibrous streamers seen in pseudopélade of Brocq.
Lichen planoporitis represents a rare variant in which lichenoid/interface changes are centered on the acrosyringium and eccrine sweat duct as it enters the epidermis. Squamous metaplasia of the ductal lining epithelium may be a feature.155
In lichen planus actinicus, the annular borders of the macules show typical features of lichen planus. In the center of the lesions, however, the epithelium is atrophic, thin, and flattened, although the lymphohistiocytic infiltrate remains. Foci of parakeratosis and eczematization within the
249 Lichenoid dermatoses
A
B
A
follicular epithelium have also been described. Lichen nitidus-like lesions may sometimes be seen (see below).
Lichen planus pigmentosus is characterized by epidermal thinning accompanied by basal cell vacuolization, pigmentary incontinence, and a superficial dermal lichenoid lymphohistiocytic infiltrate.4
Hypertrophic lichen planus is characterized by more marked hyperkeratosis and acanthosis, with the epithelium sometimes showing pseudoepitheliomatous hyperplasia such that misdiagnosis as squamous cell carcinoma is a distinct possibility, particularly in small biopsies and if clinical information is not available (Figs 7.31–7.33).84 A number of changes not seen in ordinary lichen planus may be observed and include parakeratosis, spongiosis, necrotic keratinocytes above the basal cell layer, more frequent eosinophils, and plasma cells in the dermal infiltrate. These changes may raise the possibility of a lichenoid drug eruption. The differential diagnosis is not difficult, as lichenoid drug eruptions tend to be more generalized and are not usually associated with hypertrophic changes.
B
The oral lesions of lichen planus, although often displaying the classical features, usually show parakeratosis; occasionally, alternate foci of both are evident.156 In contrast to the cutaneous lesions, the epithelium is sometimes rather thin and the sawtooth pattern indistinct (Fig. 7.34). There is typically basal cell hydropic degeneration. Basement membrane thickening due to the deposition of fibrin-rich eosinophilic amorphous material is commonly present. The cellular infiltrate, in addition to lymphocytes and histiocytes, frequently contains plasma cells. Dysplasia may be seen.
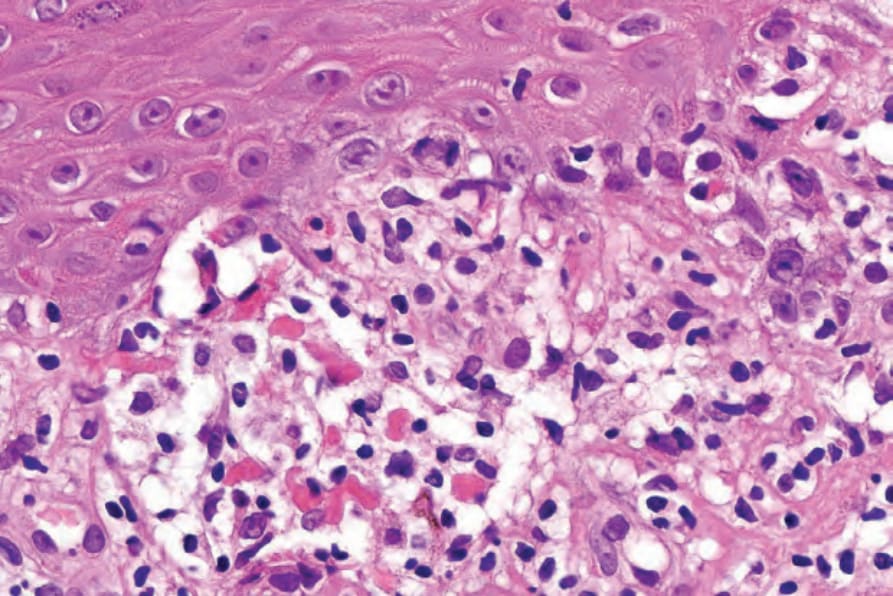
Fig. 7.20 Lichen planus: this view shows characteristic eosinophilic cytoid bodies associated with basal cell liquefactive degeneration and a lymphohistiocytic infiltrate.
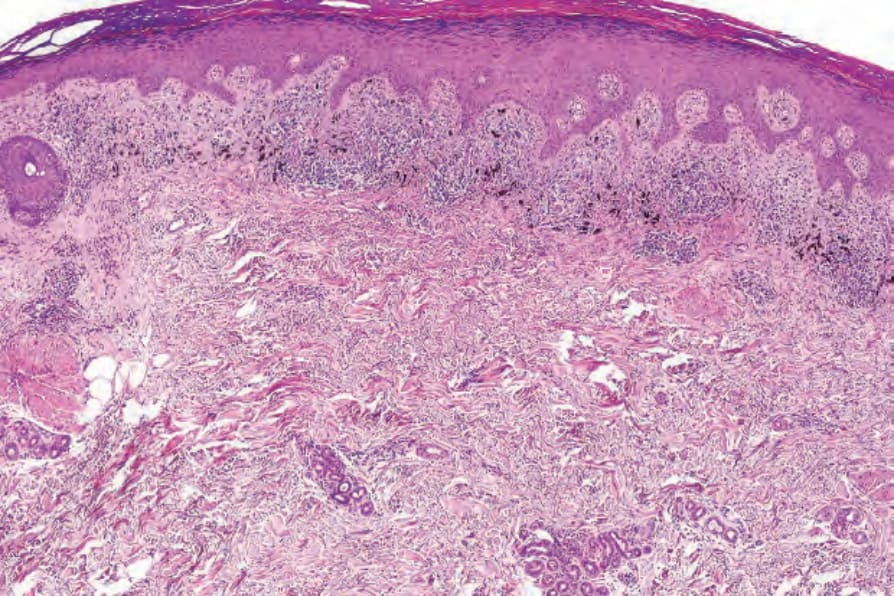
Fig. 7.21 Lichen planus: this scanning view is characteristic and highlights the hyperkeratosis, hypergranulosis, and irregular acanthosis. Note the typical bandlike inflammatory cell infiltrate and pigment incontinence.
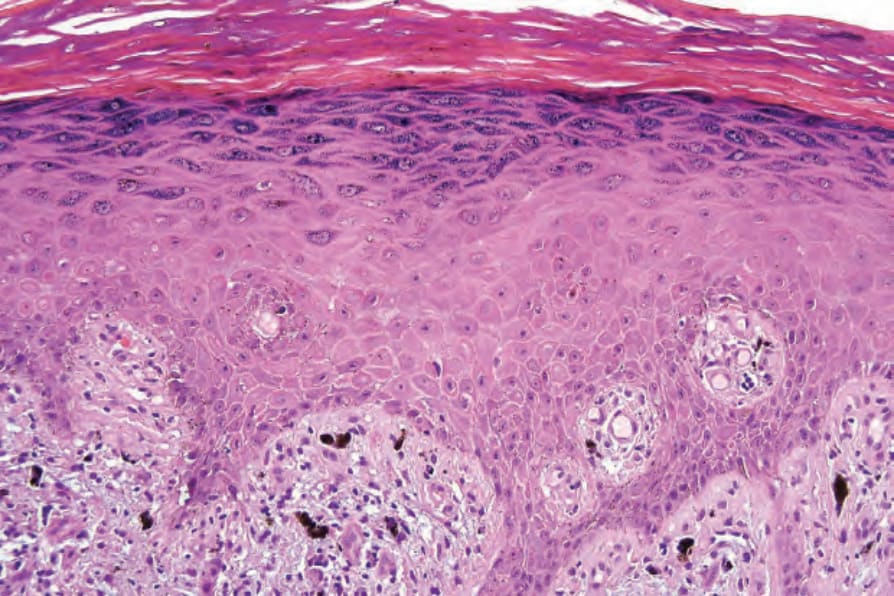
Fig. 7.22 Lichen planus: note the hyperkeratosis, hypergranulosis, and irregular acanthosis.
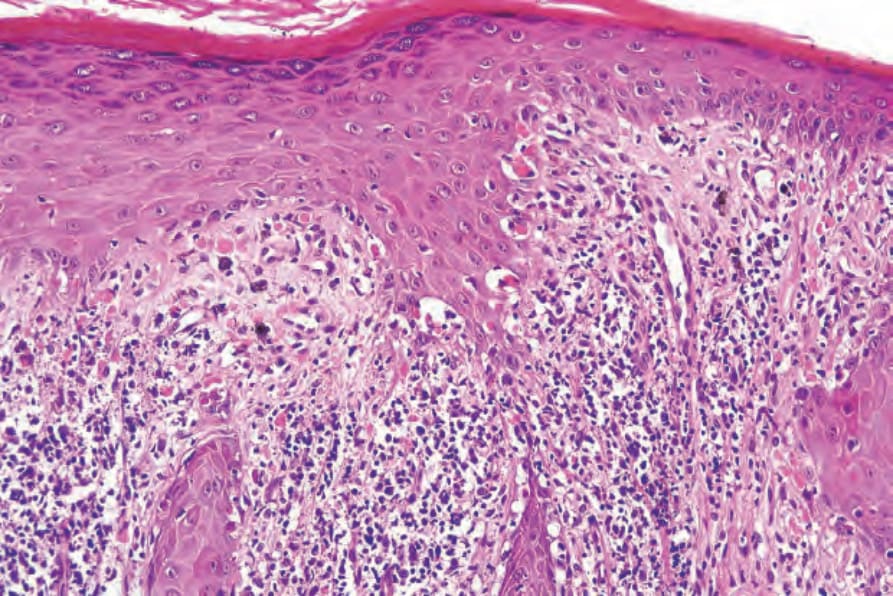
Fig. 7.24 Lichen planus: the acanthosis is irregular and often has a sawtooth appearance.
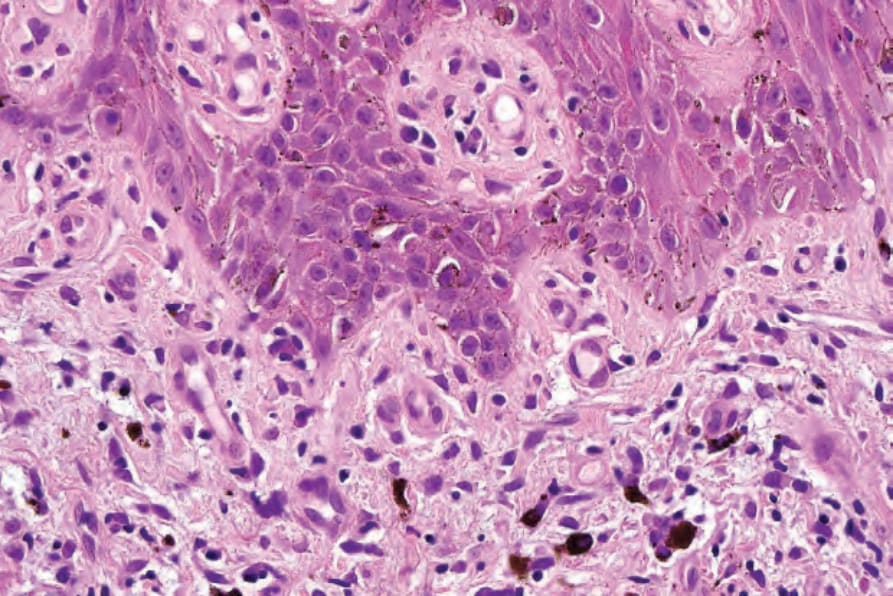
Fig. 7.26 Lichen planus: melanin pigment is present within macrophages (pigmentary incontinence).
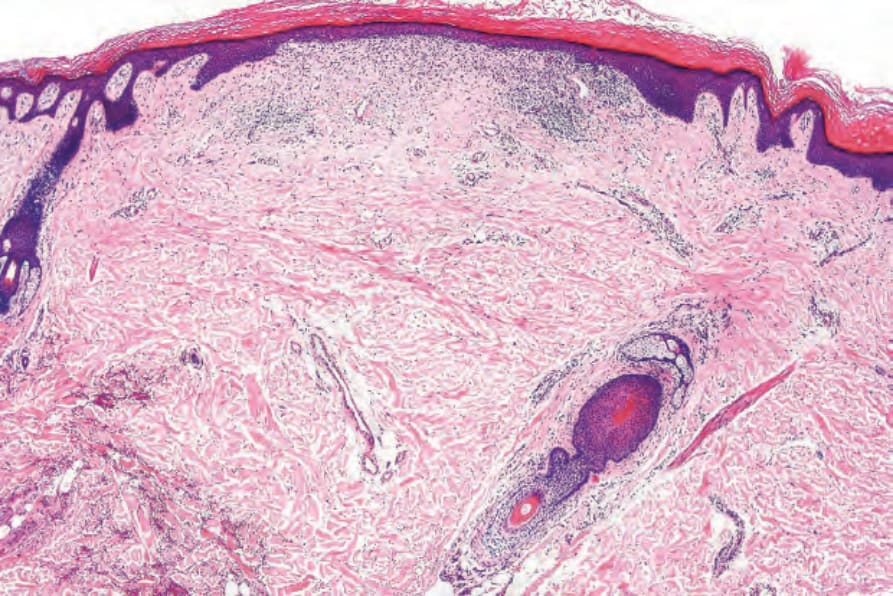
Fig. 7.27 Atrophic (resolving) lichen planus: there is hyperkeratosis, epidermal flattening, and a slight residual lymphohistiocytic infiltrate.
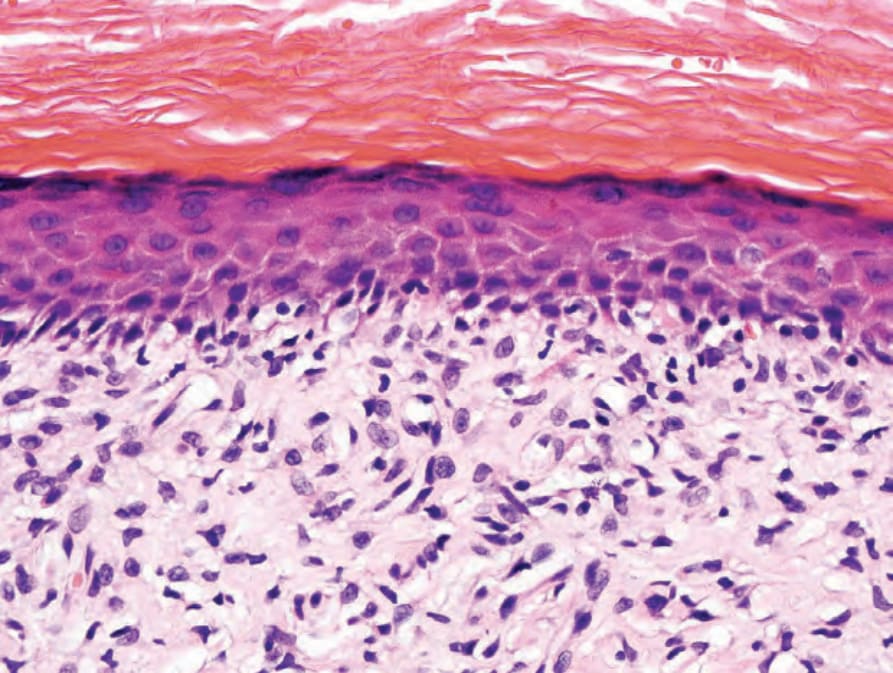
Fig. 7.28 Atrophic (resolving) lichen planus: in addition to the lymphohistiocytic infiltrate, there are excessive numbers of fibroblasts and increased papillary dermal collagen.
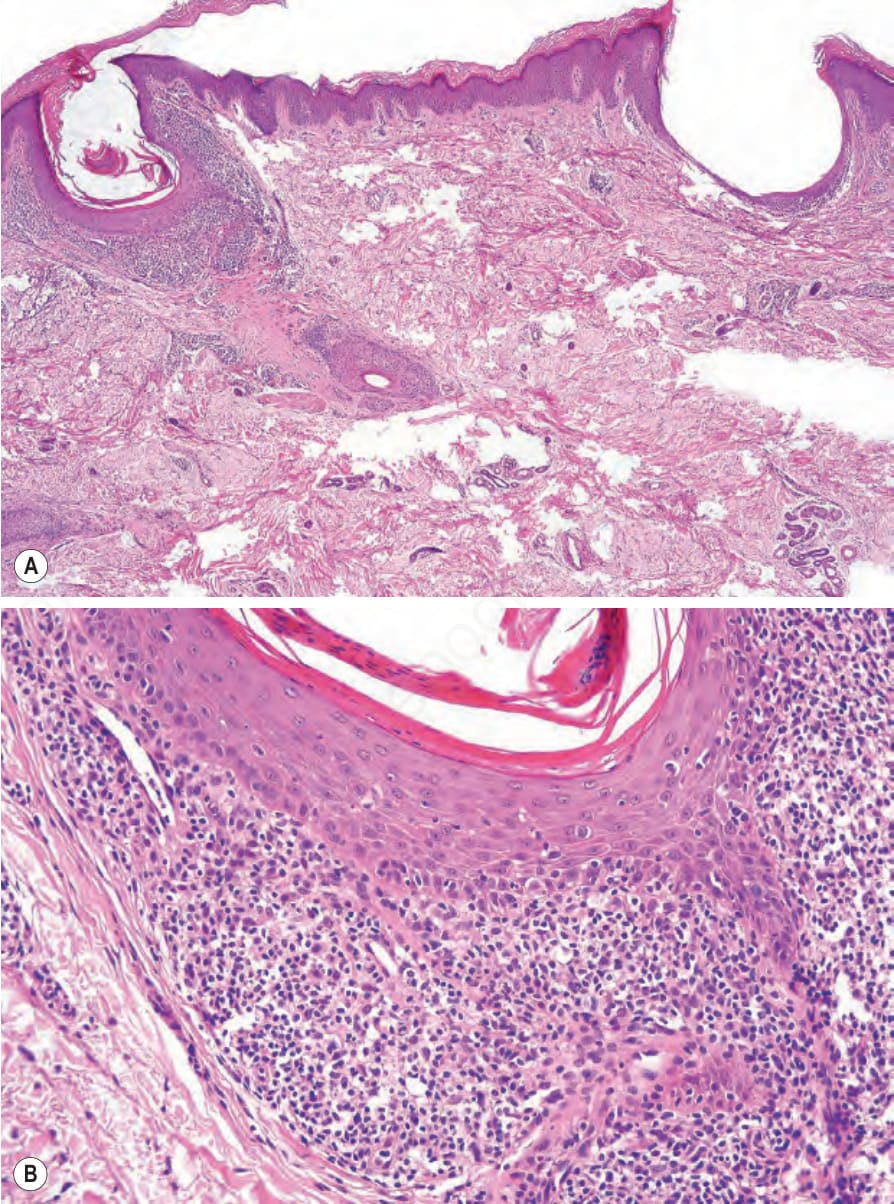
Fig. 7.29 Lichen planopilaris: (A, B) there is marked follicular dilatation and plugging accompanied by a bandlike folliculocentric infiltrate. This patient presented with scarring alopecia and typical lichen planus lesions elsewhere.
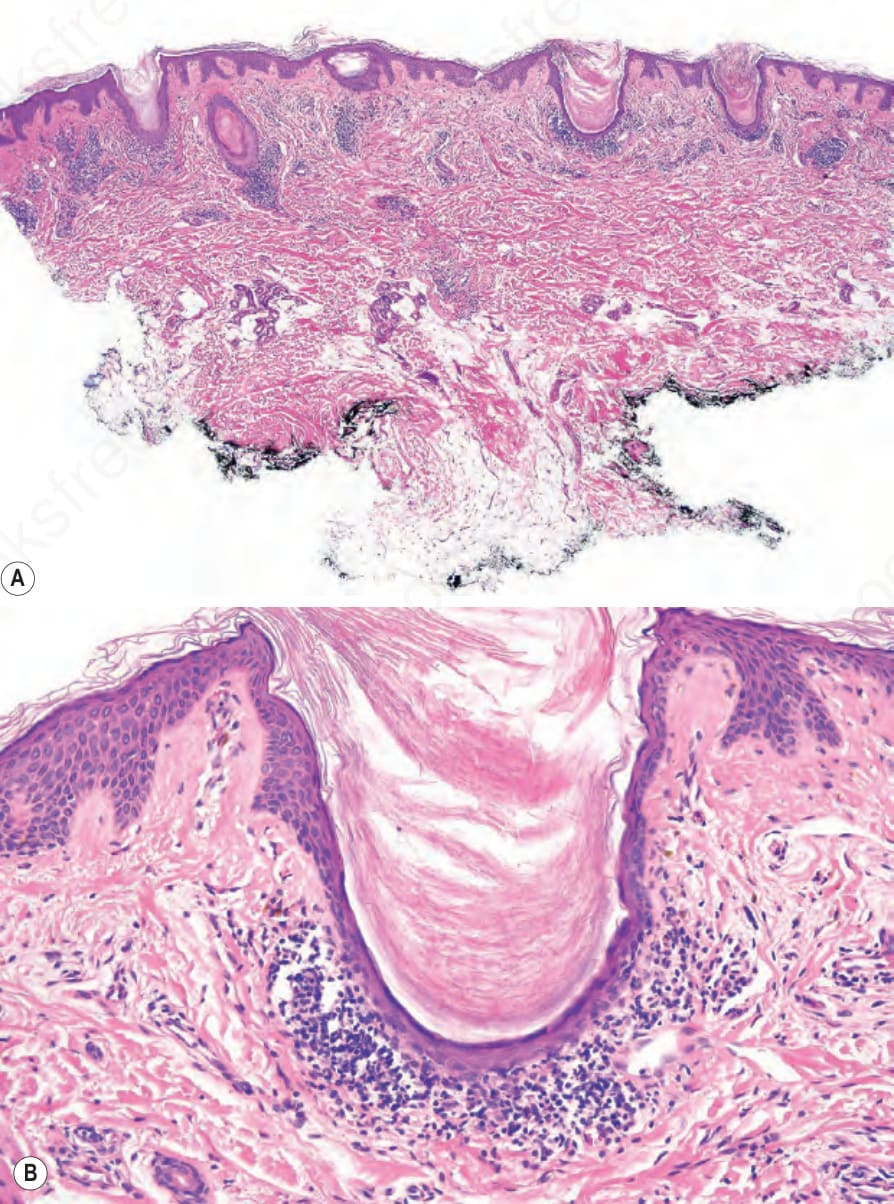
Fig. 7.30 Lichen planopilaris: (A, B) there is a strikingly folliculocentric bandlike infiltrate associated with keratin plugging. The interfollicular epidermis is unaffected.
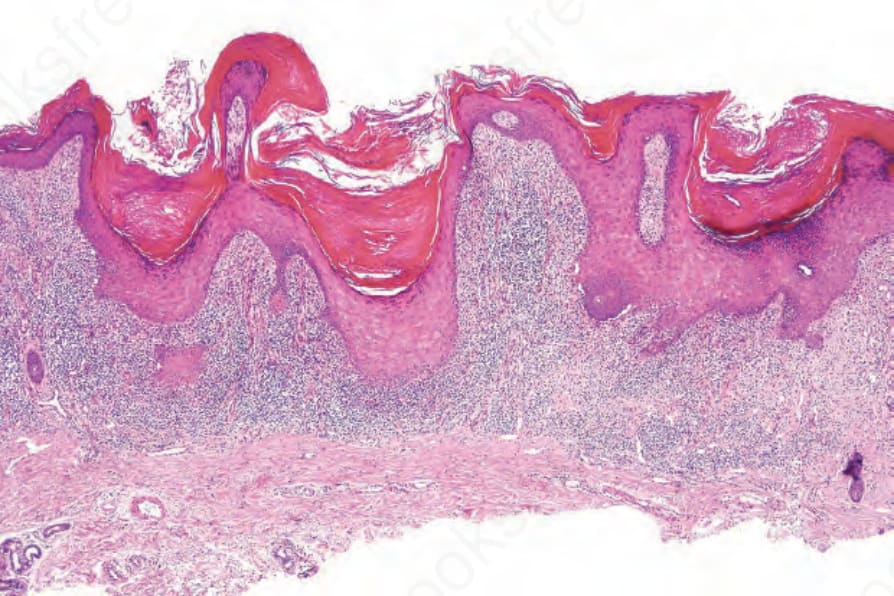
Fig. 7.31 Hypertrophic lichen planus: note the hyperkeratosis, focal wedge-shaped hypergranulosis, very marked irregular acanthosis, and superficial dense bandlike infiltrate.
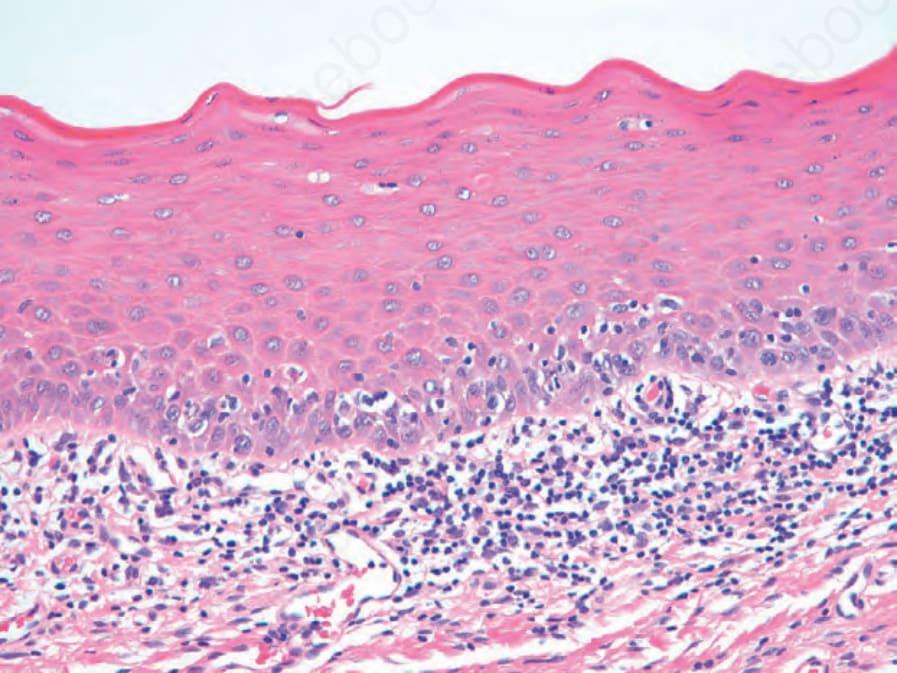
Fig. 7.34 Oral lichen planus: there is parakeratosis, a subtle granular layer, and no sawtoothing of the epithelial–subpithelial junction in contrast to cutaneous lichen planus.
250 Lichenoid and interface dermatitis
Unlike skin involvement, esophageal lesions show parakeratosis. Variable epithelial atrophy and/or mild thickening are usually seen, and the sawtooth pattern of acanthosis is not a feature.33,37–39 As with oral lesions, plasma cells often accompany the lymphocytic infiltrate.
Vesicular or bullous lesions are subepidermal and occur due to excessive edema developing in association with the basement membrane zone damage complicating basal cell hydropic degeneration (Fig. 7.35).
Direct immunofluorescence studies from patients with lichen planus usually reveal a linear fibrillar band of fibrin at the dermal–epidermal junction (Fig. 7.36). The cytoid bodies may be highlighted non-specifically, mainly to IgM, but also to IgG, IgA, and C3 (Fig. 7.37). A lichen planus ‘specific antigen’, which is present in the prickle cell and granular cell layers, has been demonstrated by indirect immunofluorescence of patients’ serum with fetal skin.157 The pathogenetic significance of this is unknown. Direct immunofluorescence of lichen planopilaris reveals follicular, linear basement membrane zone labeling with immunoglobulin (primarily IgG or IgA).158 Fibrin may also be present. The nosological implications of this observation are uncertain. Indirect immunofluorescence for circulating antibasement membrane zone antibodies is negative.
Differential diagnosis Lichen planus should be differentiated from other diseases showing a lichenoid infiltrate and hydropic degeneration of the basal layer of the epithelium.159 Thus, lichen planus may be indistinguishable from lichenoid keratosis and their distinction is entirely dependent on clinicopathological correlation. In many cases of lichenoid keratoses, there are other associated changes including focal spongiosis and parakeratosis. Atrophic lesions may be confused with poikiloderma and chronic discoid lupus erythematosus. A lichen planus-like morphology is typical of the early stages of chronic
251 Lichenoid dermatoses
graft-versus-host disease (GVHD), but the density of the infiltrate is typically less in this entity.
Poikiloderma shows epidermal atrophy, with loss of the ridge pattern and no tendency to a sawtooth appearance. In those examples associated with mycosis fungoides, the lichenoid infiltrate contains variable numbers of atypical lymphocytes.
Chronic discoid lupus erythematosus is associated with epidermal atrophy and follicular plugging. The inflammatory cell infiltrate is patchy with a tendency to periappendageal location with associated dermal mucin deposition. A positive lupus band test can be helpful.
Lichen planus may easily be mistaken for a lichenoid drug reaction, particularly in the absence of clinical information. Histologic features favoring
the latter include high-level cytoid bodies and frequent eosinophils within the dermal infiltrate.
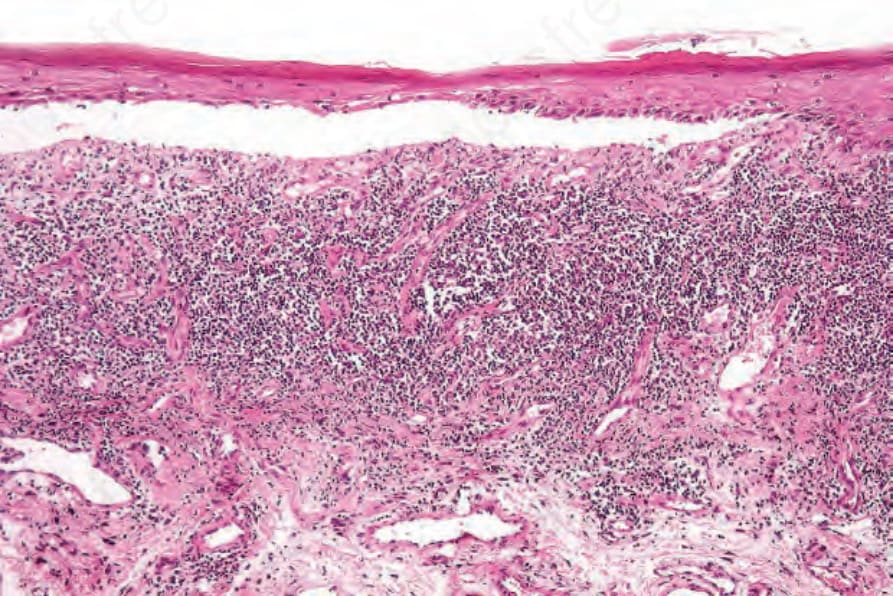
Fig. 7.35 Bullous lichen planus: oral lesion showing separation of the squamous epithelium from the lamina propria. Note the bandlike infiltrate.
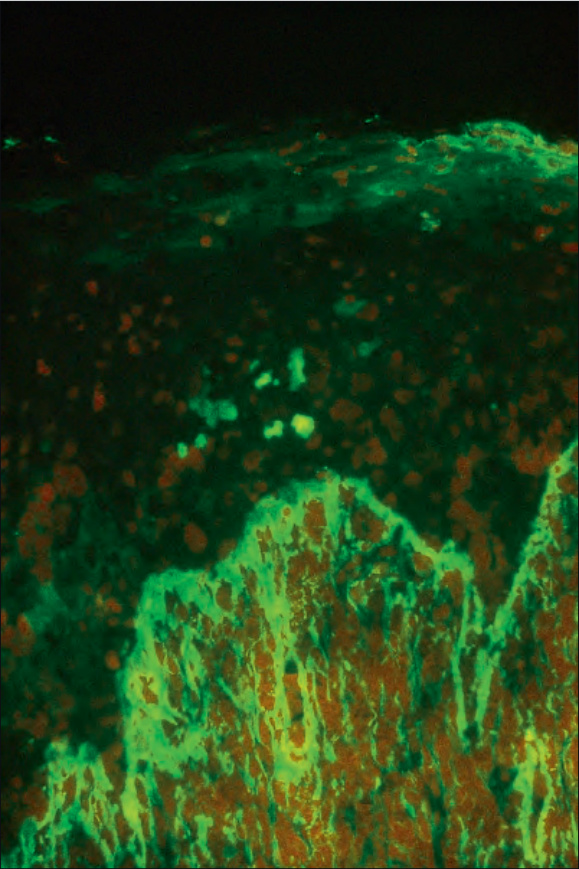
Fig. 7.36 Lichen planus: brilliant green fluorescence indicates the presence of fibrin. By courtesy of the Department of Immunofluorescence, Institute of Dermatology, London, UK.
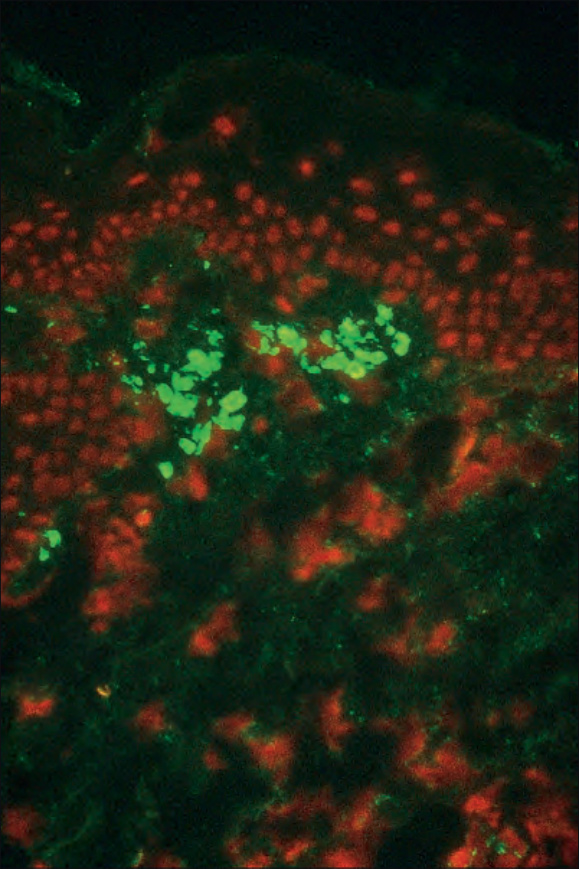
Fig. 7.37 Lichen planus: cytoid bodies labeled positively for IgM. By courtesy of the Department of Immunofluorescence, Institute of Dermatology, London, UK.