Morton neuroma
Morton neuroma
Clinical features Morton neuroma (metatarsalgia) is also not a true neoplasm, but represents a degenerative response to chronic low-grade tissue damage.1,2 It most often presents in adults, who complain of pain in the distal sole of the foot, usually when walking. Females are affected more often than males. Close examination reveals that the pain is often localized between (or over) the metatarsal heads, but a nodule or mass is not usually palpable. Bilateral involvement is rare.3 If excision is undertaken, a localized, rather fusiform, expansion of one of the plantar digital nerves is seen. Excision is usually undertaken for symptomatic lesions but in a percentage of patients, pain resists or even gets worse.4–8 A relationship between the width of the forefoot and the Greek foot has been suggested.9,10
Histologic features Histologically, in dermal hyperneury, hyperplastic and hypertrophic myelinated nerve bundles are seen scattered throughout the dermis.7 When associated with an inflammatory infiltrate, it must be distinguished from an infectious process.8
Histologic features Traditionally, histology has been described as revealing marked fibrosis of the endo-, epi- and perineurium associated with edematous change, marked degeneration and loss of nerve fibers (Figs 35.298 and 35.299). Fibrotic changes are often seen in the adjacent subcutaneous tissues and around blood vessels. However, a recent study comparing the histology of nerves
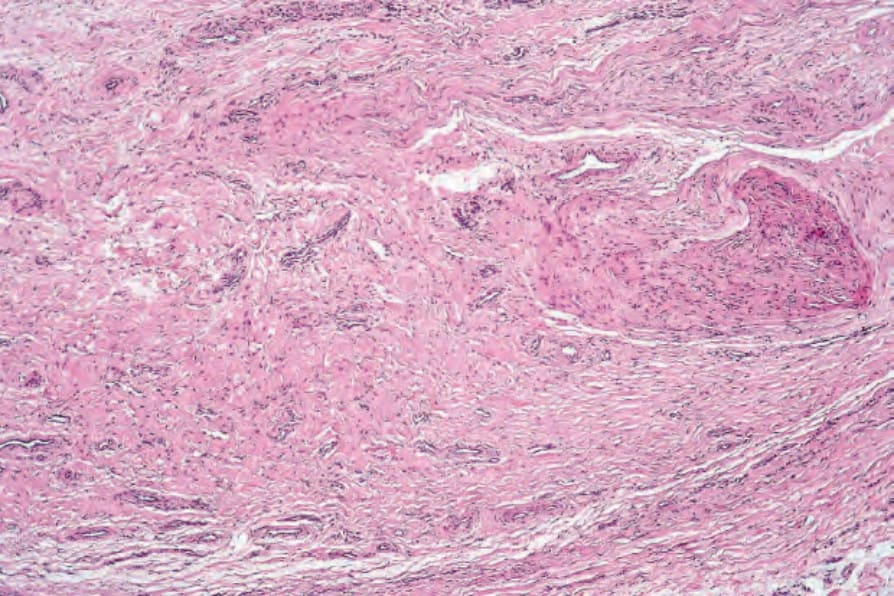
Fig. 35.298 Morton neuroma: the nerve trunk is markedly distorted by intense concentric fibrosis.