Dermatofibrosarcoma protuberans
Dermatofibrosarcoma protuberans
Clinical features
Dermatofibrosarcoma protuberans typically presents in the third and fourth decades, shows a slight male predominance and is uncommon in the elderly.1–5 However, many patients have a long preoperative history (often 10–20 years), probably corresponding to the plaque phase. In these patients a patch develops and may have features resembling morphea, atrophoderma, or an angioma.6 Lesions can occur in children and some of these are congenital (Fig. 35.140).1,4,7–17 Clinical diagnosis in this age group is difficult, as tumors often resemble a vascular birthmark.6 Occurrence at sites of previous trauma (including scars, vaccination, an arteriovenous fistula, a decorative tattoo and leishmaniasis) and even post-radiation tumors have been documented.18–25 Familial cases are exceptional and an association with HIV infection is probably coincidental.26,27 Accelerated growth during pregnancy has been reported in a case.27 Rare (probably coincidental) associations include multiple spindle cell lipomas and a nuchal fibroma.28,29
cell fibroblastoma may recur as dermatofibrosarcoma protuberans and vice versa.18,19 Bednár tumor (pigmented dermatofibrosarcoma protuberans) may also present primarily or recur with areas of giant cell fibroblastoma.20,21 Mixed tumors may have fibrosarcomatous areas and myoid nodules.7
The tumor usually develops as a multinodular cutaneous mass, several centimeters in diameter that is slowly growing and appears to evolve from a dermal fibrous plaque stage. The overlying skin frequently shows a reddish-blue discoloration (Figs 35.141–35.143). Presentation as an atrophic plaque is seen in some cases (Fig. 35.144).30,31 Polypoid tumors are exceptionally seen.32 There is a marked predilection for the trunk (especially the abdominal wall and chest) and lower limbs (particularly the thighs). Involvement of distal extremities is very uncommon with most tumors developing on the foot (mainly the toes) and ankle and hardly any on the hands.33–36 Rare tumors occur in the vulva and exceptional cases have been reported in the oral cavity, penis, and male breast.37–45 Simultaneous occurrence of two tumors at different sites has been documented. Multicentric dermatofibrosarcoma protuberans in patients with adenosine deaminase-deficient severe combined immune deficiency has been documented.46,47
Differential diagnosis Distinction from other myxoid tumors is readily made based on the biphasic appearance of solid and angiectoid areas with giant cells. Fibrous hamartoma of infancy may rarely show areas resembling giant cell fibroblastoma and in these areas tumor cells are also positive for CD34.22 The diagnosis is usually established by the presence of the distinctive components seen in fibrous hamartoma of infancy.
Intermediate (rarely metastasizing) fibroblastic and myofibroblastic tumors
Low-grade malignant lesions are defined as neoplasms with a high recurrence rate and very low metastatic potential.
Purely subcutaneous tumors rarely occur and seem to have a predilection for head and neck.48,49
Local recurrence is frequent and varies in different series from 20% to 50% of cases.1,5,50–56 However, in cases treated by wide excision or in those treated by Mohs micrographic surgery the rate of local recurrence is lower.57–62 A frequent subject of debate is how wide the excision has to be to reduce the rate of local recurrence. Although the tendency in the past was to advocate several excisions with margins of several centimeters, more recent studies suggest that smaller excision margins of 2 cm achieve good local control in many cases.63 Treatment with Mohs micrographic surgery using paraffin sections appears to be an excellent choice of treatment, allowing tissue conservation.64 Other therapeutic options include excision
1742 Connective tissue tumors
with wide margins with or without radiotherapy, depending on the margin status. For recurrent or metastatic tumors, targeted therapy may be of help (see below). A multidisciplinary approach is the best option when dealing with challenging cases.63–76 Intracranial invasion may occur in scalp lesions mainly after multiple recurrences.77 Metastasis is exceedingly rare, less than 0.3% in our experience; many of the cases reported to have metastasized are supported by inadequate or even incorrect histologic evidence. Metastasis usually occurs after repeated recurrences, often with fibrosarcomatous transformation.1–3,78–82 Fibrosarcomatous dermatofibrosarcoma protuberans recurs locally in 75% and the rate of metastasis is up to 23% of cases in some series.78,79,83–85 However, in a more recent series, the rate of local recurrence (20%) and metastatic rate (10%) is much less than that reported in the past.83 Aggressive behavior appears is suggested to be related to mitotic activity, pleomorphism and necrosis.57,78,79,87
Pathogenesis and histologic features The genetic abnormalities found in dermatofibrosarcoma protuberans and giant cell fibroblastoma are identical, further indicating that they represent a spectrum.88–90 As expected, other histologic variants of dermatofibrosarcoma protuberans – including Bednár tumor, dermatofibrosarcoma protuberans with granular cell change and fibrosarcomatous dermatofibrosarcoma protuberans – show the same cytogenetic abnormalities.91–99 Ring chromosomes derived from chromosome 22 containing low-level amplified sequences from 17q22-qter and 22q10-q13.1 or t(17;22) are the most frequent finding.90 In both the rings and linear der(22) a specific fusion of COL1A1 and PDGFB is found. Ring chromosomes are mainly observed in adults, whereas translocations are present in all pediatric cases.90 The breakpoint localization in PDGFB is remarkably constant, placing exon 2 under control of the COL1A1 promoter. In contrast, the COL1A1 breakpoint is variably located within the exons of the α-helical coding region (exons 6–49).90,95–97
Evidence of the COL1A1-PDGFB fusion by multiplex reverse transcription polymerase chain reaction or fluorescence in situ hybridization assays is present in almost all cases.90,95–97,100
A recent study of ordinary DFSP and tumors with fibrosarcomatous transformation suggested an association between the activation of the Akt-mTOR pathway proteins and PDGFR with progression from ordinary DFSP to fibrosarcomatous DFSP.101 A case of fibrosarcomatous DFSP expressing programmed death-ligand 1 (PD-L1) in the metastasis but not in the primary tumor has been reported.102
Clonal evolution consisting of different somatic mutations and novel focal amplifications, has been found in metastatic samples but no in those obtained before metastasis is a single patient.103 In a further study, no significant copy number alterations, insertion, or deletions was observed during imatinib treatment response.104 However, emergence of 8 new
1743 Intermediate (rarely metastasizing) fibroblastic and myofibroblastic tumors
non-synonymous somatic gene mutations in imatinib-resistant tumor tissue was identified.
PDGFB appears to act as a mitogen in tumor cells of dermatofibrosarcoma protuberans by autocrine stimulation of the PDGF receptor. Interestingly, imatinib mesylate (an antagonist of the PDGF receptor α tyrosine kinase) has been found to have an inhibitory effect in vivo and has been used with variable success in multiple cases of dermatofibrosarcoma protuberans (mainly in patients with unresectable or recurrent tumors and those with metastatic disease).90,105–109 The rate of response has been estimated to be up to 50%.110
A single case of dermatofibrosarcoma protuberans-like tumor with COL1A1 copy number gain without t(17;22) has been described. In this case, tumor cells were positive for CD3 and H-caldesmon and very focally positive for EMA and SMA.111
The microscopic appearances vary little from case to case. The tumor is located in the dermis, but invariably shows diffuse irregular infiltration of the subcutaneous fat in a typical lace-like pattern or bundles of cells which ramify parallel to the epidermis (Figs 35.145 and 35.146). Rare cases may be mainly or exclusively subcutaneous.48,49,112 Epidermal hyperplasia is very rare but does occur and the degree of hyperplasia seems to be inversely related to the distance of the tumor from the epidermis.113
The lesion is composed almost entirely of fairly uniform spindled cells with elongated nuclei showing little or no pleomorphism and scanty pale cytoplasm. The cells are characteristically arranged in a storiform or ‘rush mat’ pattern typified by numerous whorls of cells, sometimes centered around small blood vessels (Figs 35.147–35.149).
Mitotic activity, rarely abnormal in appearance, is scanty, not usually exceeding five mitoses per 10 high-power fields. Peripheral collections of chronic inflammatory cells are sometimes present, as are foci of myxoid degeneration, but necrosis is rarely a feature and is always minimal (Fig. 35.150). Cytological polymorphism is not a feature except in those infrequent cases showing overlap with giant cell fibroblastoma. However, in some cases, occasional nonpleomorphic giant cells are present. Focal histologic variation may be seen and includes areas of sclerosis, palisading, formation of Verocay-like bodies, granular cell change, meningothelial-like whorls and pseudocystic spaces.114–120 In a case treated with imatinib mesylate prominent hyalinized collagen was seen.121
Immunohistochemically, tumor cells are usually diffusely positive for CD34 and negative for other markers including factor XIIIa, S100 protein, desmin, actin and, with rare exceptions, CD117 (Fig. 35.151).122–124 Staining for EMA has been reported and, based on this finding, a perineural line of differentiation has been suggested although this marker is not specific.125
CD99 is also positive in a number of cases.126 Stromelysin, cathepsin K and D2–40 have been reported as useful markers in the differential diagnosis between dermatofibroma and dermatofibrosarcoma protuberans, as they tend to be positive in the former and negative in the latter.127–129 Cthrc1 (collagen triple helix repeat containing-1) and Apo D, on the other hand, tend to be positive in dermatofibrosarcoma protuberans and negative in dermatofibroma.130,131 Other markers that have been reported as useful in dermatofibrosarcoma protuberans include low-affinity nerve growth factor receptor (p75) and tenascin.132 Tumor cells in dermatofibroma and dermatofibrosarcoma protuberans show positive staining with tenascin but staining of the dermal–epidermal junction overlying the tumor is only seen in dermatofibroma.133
Although the line of differentiation in dermatofibrosarcoma protuberans has been controversial for many years, it is increasingly being accepted as a fibroblastic tumor (Figs 35.152 and 35.153).134,135
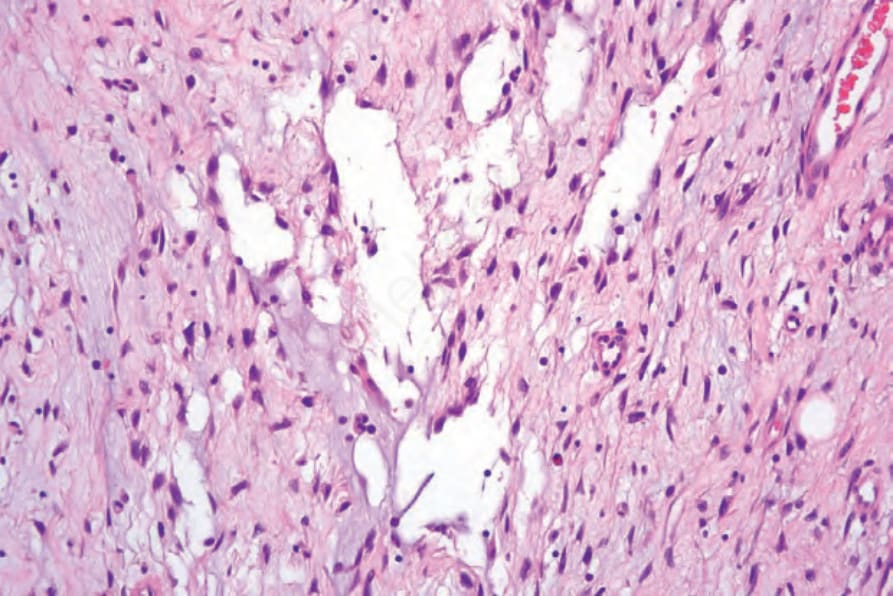
Fig. 35.139 Giant cell fibroblastoma: higher-power view of the left side of the field showing typical features.

Fig. 35.140 Dermatofibrosarcoma protuberans: congenital lesions as shown here are exceedingly rare. By courtesy of the Institute of Dermatology, London, UK.

Fig. 35.141 Dermatofibrosarcoma protuberans: a typical multinodular reddish-blue plaque is present on the lower abdomen of a middle-aged female. By courtesy of M.H.A. Rustin, MD, Royal Free Hospital, London, UK.

Fig. 35.142 Dermatofibrosarcoma protuberans: close-up view. By courtesy of M.H.A. Rustin, MD, Royal Free Hospital, London, UK.

Fig. 35.143 Dermatofibrosarcoma protuberans: this example shows a combination of a plaque and nodules. By courtesy of the Institute of Dermatology, London, UK.
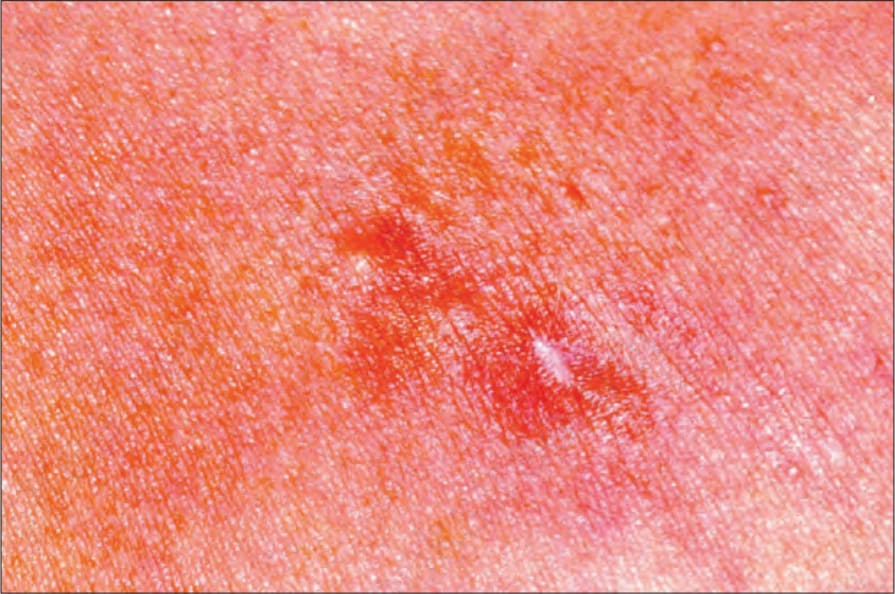
Fig. 35.144 Dermatofibrosarcoma protuberans: presentation as an atrophic plaque is rare. By courtesy of the Institute of Dermatology, London, UK.
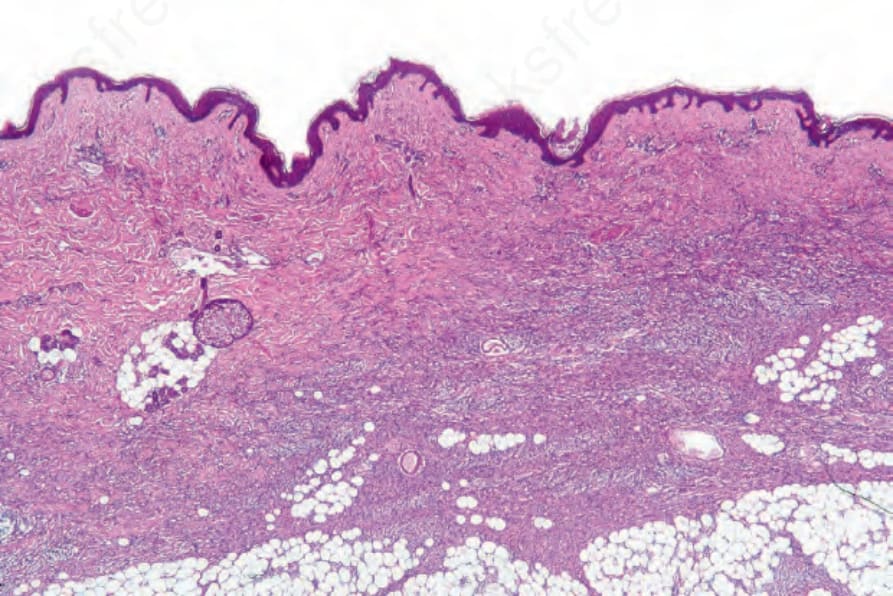
Fig. 35.145 Dermatofibrosarcoma protuberans: the lower dermis is replaced by a dense cellular infiltrate. In contrast to fibrous histiocytoma, the epidermis appears normal.
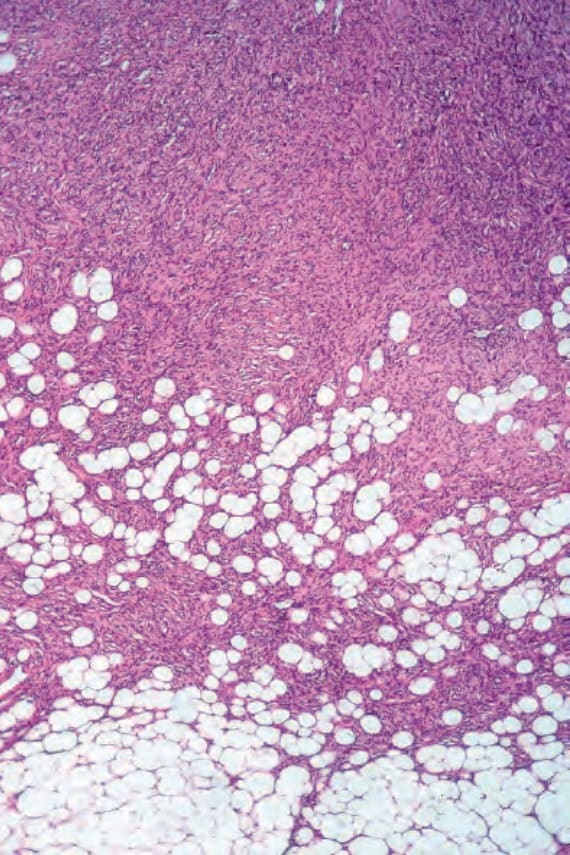
Fig. 35.146 Dermatofibrosarcoma protuberans: involvement of the subcutaneous fat is usual and typically results in a lace-like appearance.
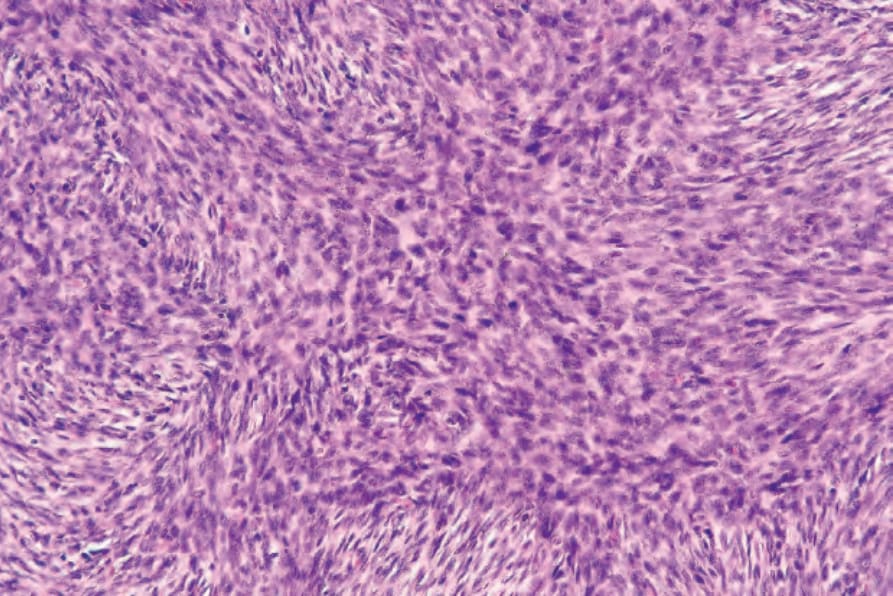
Fig. 35.147 Dermatofibrosarcoma protuberans: this field shows the characteristic storiform (L. storia, a rush mat) pattern.
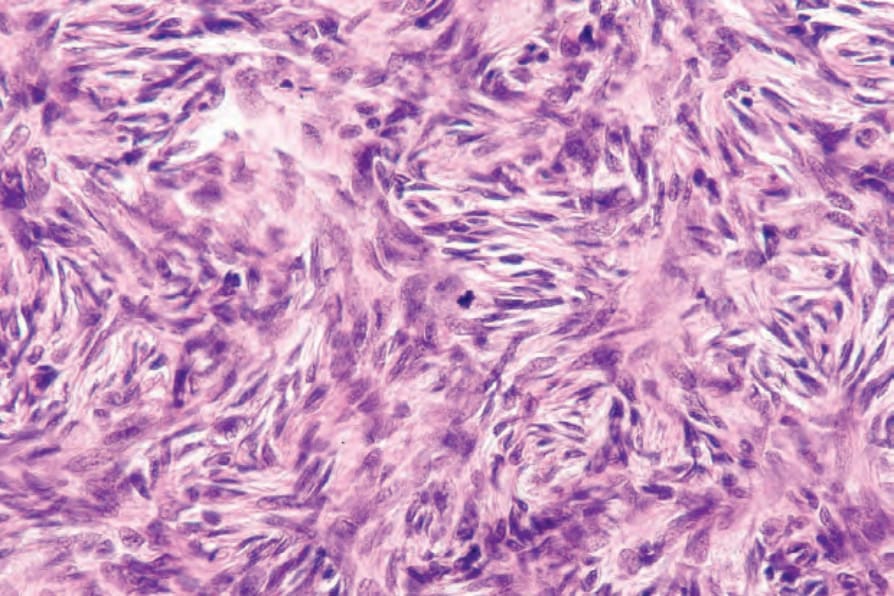
Fig. 35.148 Dermatofibrosarcoma protuberans: the storiform pattern comprises a central, almost syncytial, arrangement of cells with vesicular nuclei from which radiate the more delicate spindle cells with elongated darkly staining nuclei. Taken in context, this appearance is pathognomonic. Note the mitotic figure.
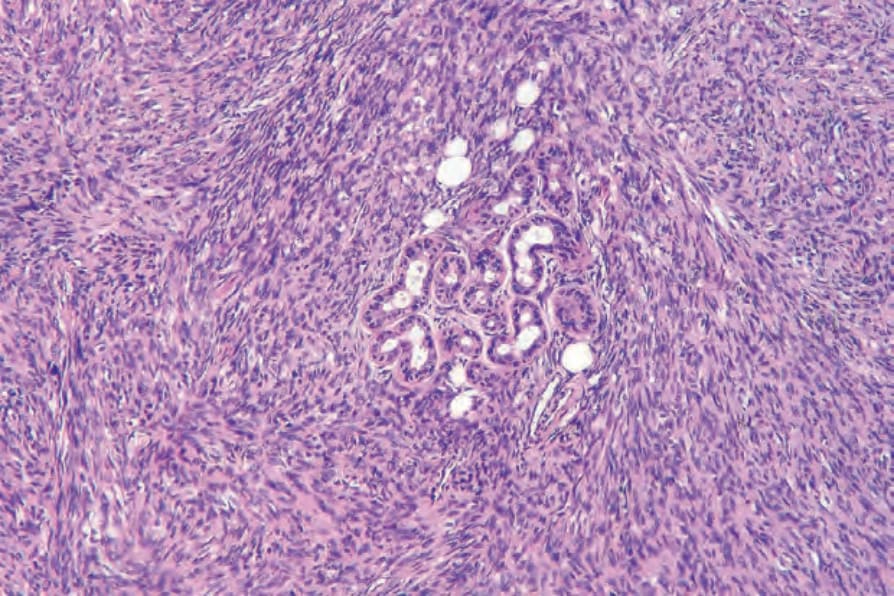
Fig. 35.149 Dermatofibrosarcoma protuberans: adnexal sparing is typically seen.
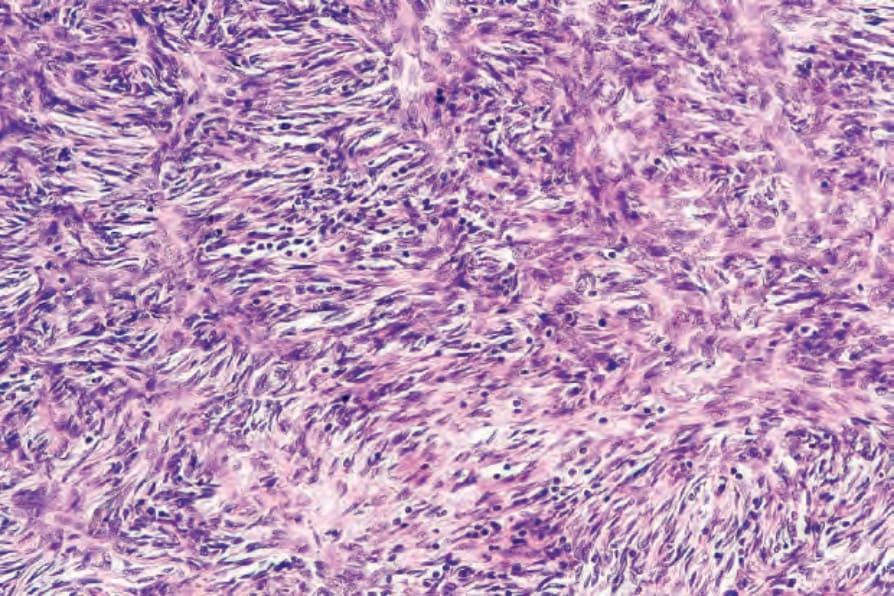
Fig. 35.150 Dermatofibrosarcoma protuberans: a diffuse lymphocytic infiltrate is present in this field.
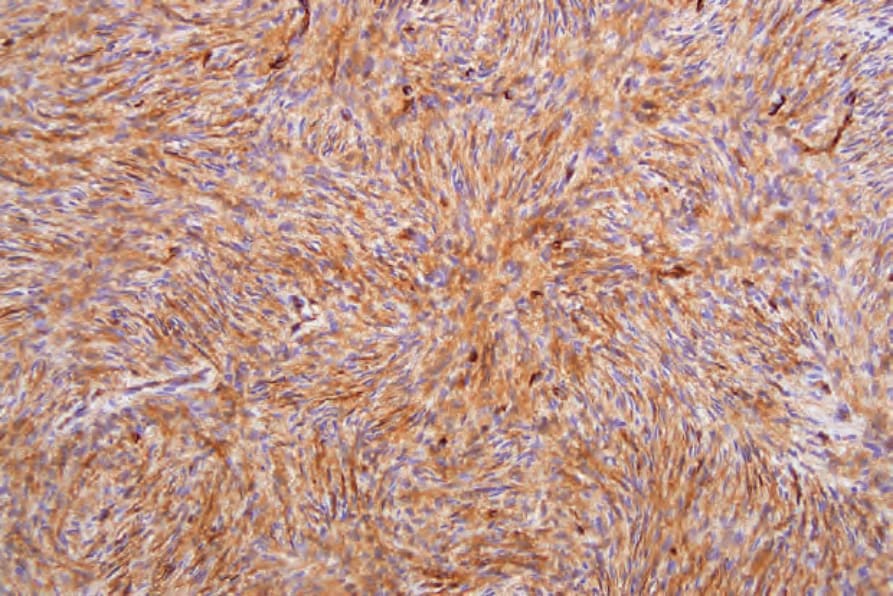
Fig. 35.151 Dermatofibrosarcoma protuberans: the tumor cells characteristically express CD34.
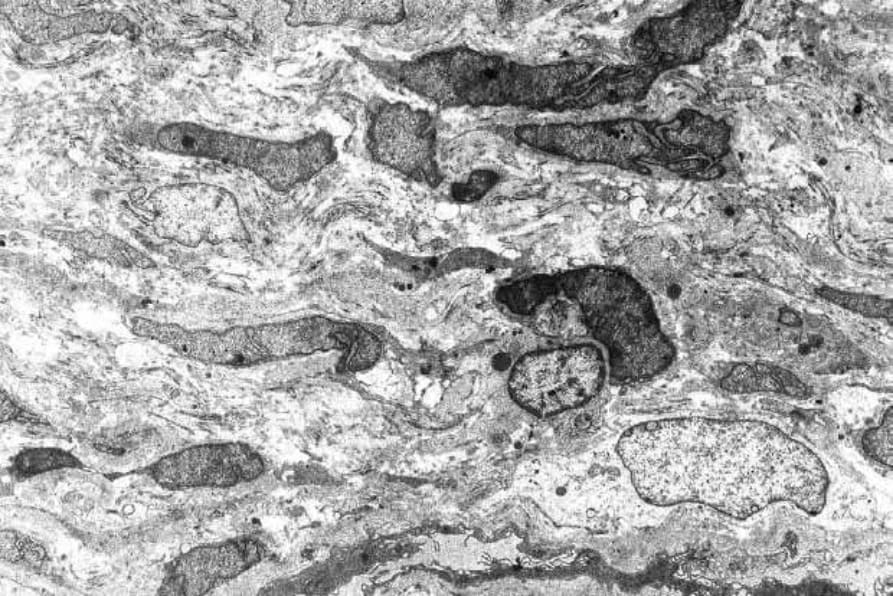
Fig. 35.152 Dermatofibrosarcoma protuberans: the tumor consists of a uniform population of fibroblasts typified by elongated nuclei and abundant rough endoplasmic reticulum.
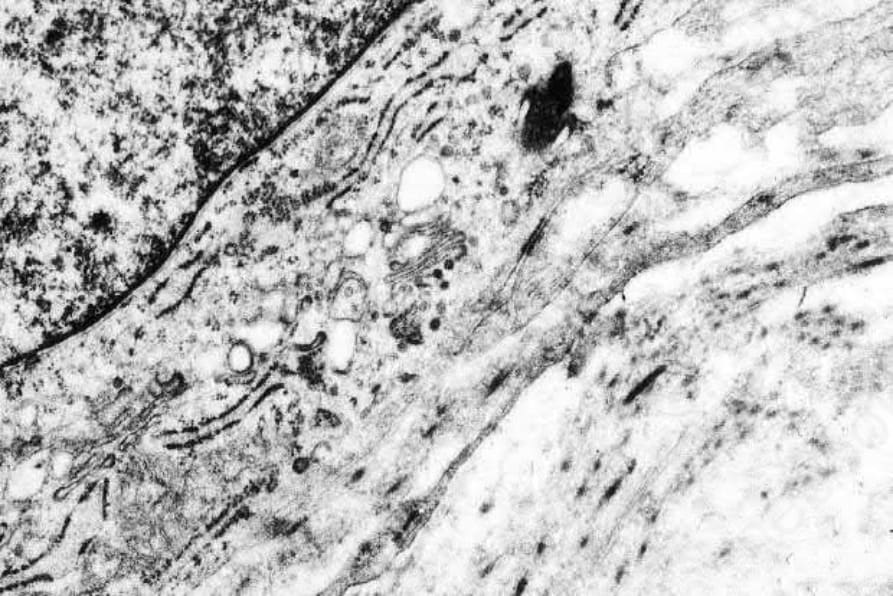
Fig. 35.153 Dermatofibrosarcoma protuberans: myofibroblastic differentiation is not a feature of this tumor.
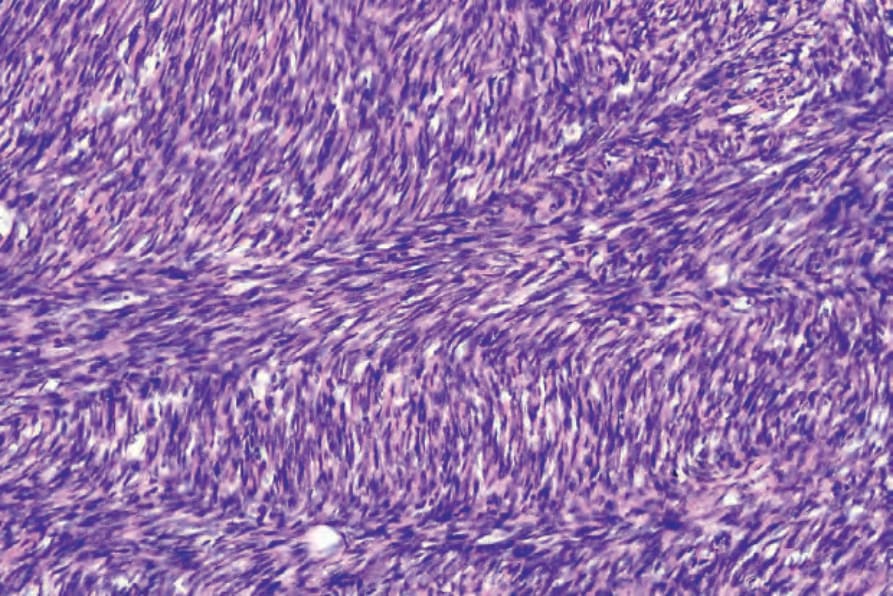
Fig. 35.155 Dermatofibrosarcoma protuberans: high-power view.
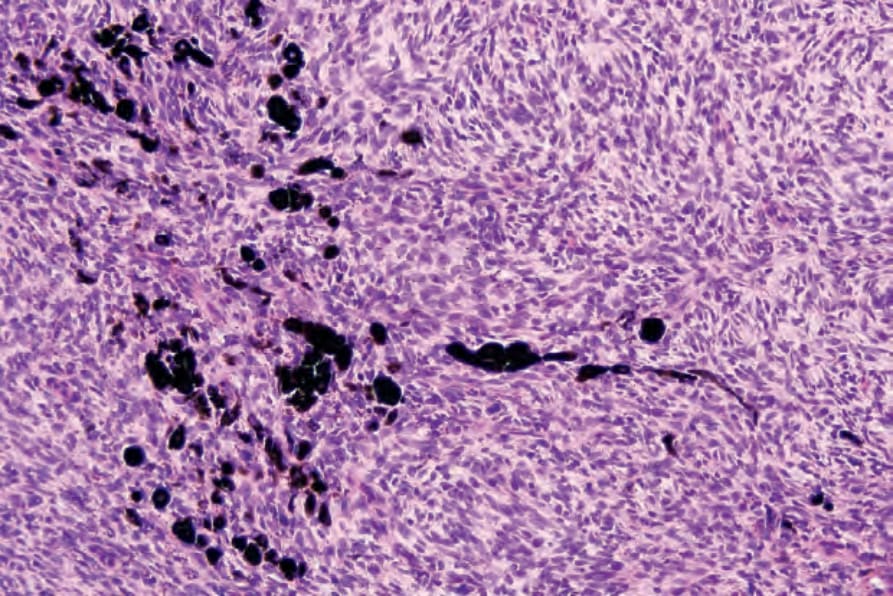
Fig. 35.157 Bednár tumor: the melanin pigment is contained within dendritic cells.
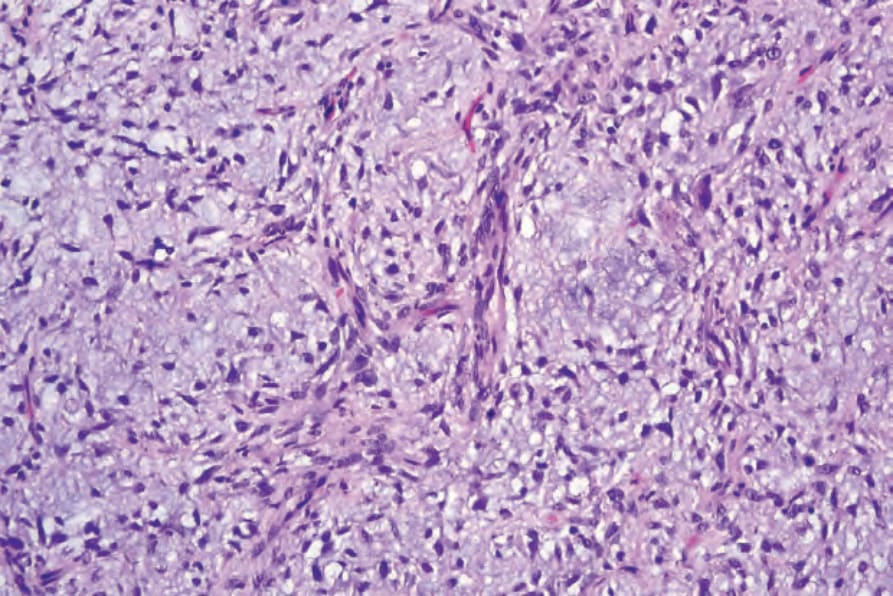
Fig. 35.159 Myxoid dermatofibrosarcoma protuberans: high-power view.
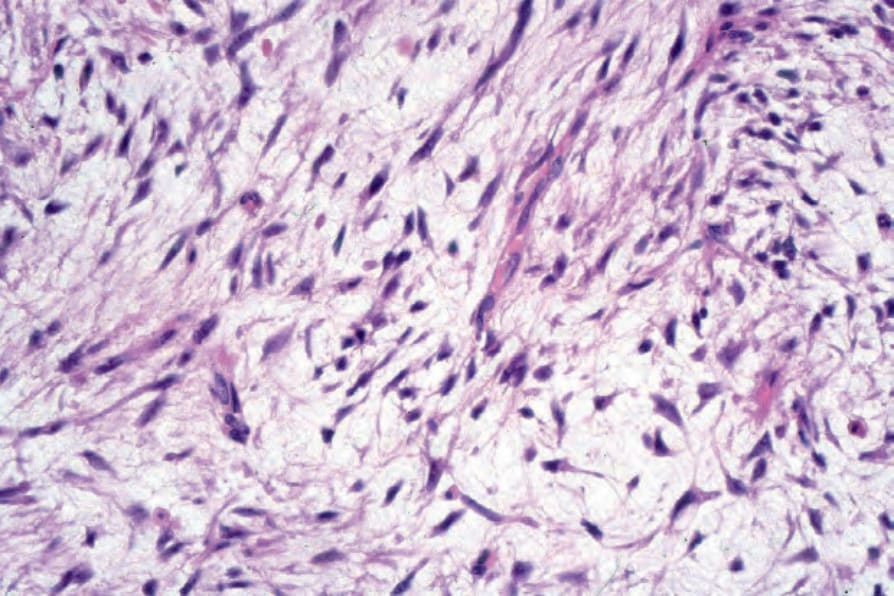
Fig. 35.160 Myxoid dermatofibrosarcoma protuberans: high-power view from a different case showing complete loss of the storiform growth pattern.
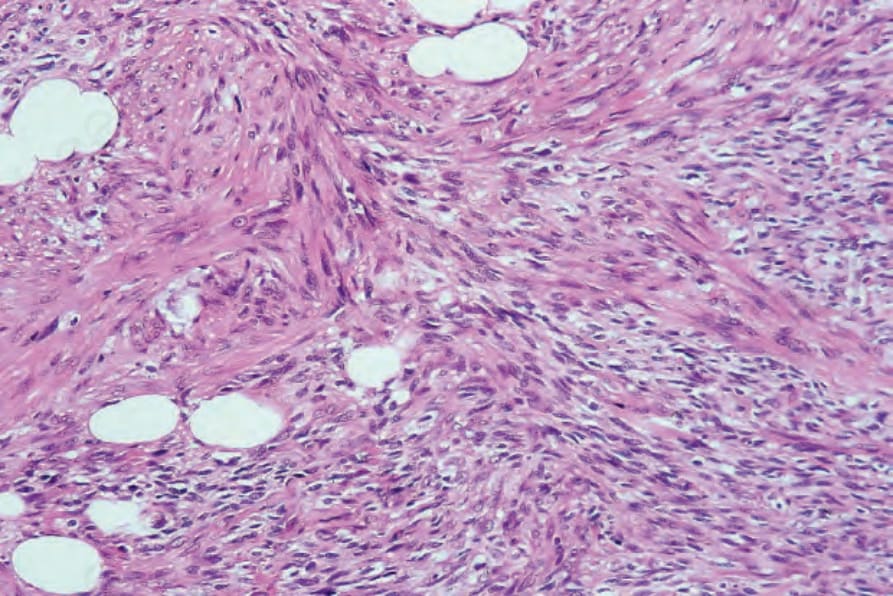
Fig. 35.162 Dermatofibrosarcoma protuberans: high-power view of Figure 35.170.
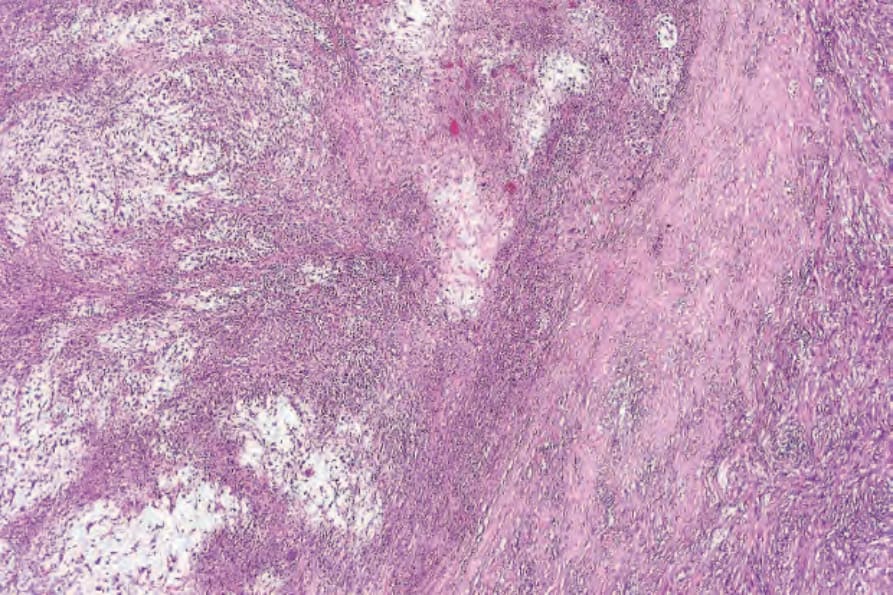
Fig. 35.163 Acral myxoinflammatory fibroblastic sarcoma: within the dermis is a multinodular tumor with striking myxoid change.
1744 Connective tissue tumors
1745 Intermediate (rarely metastasizing) fibroblastic and myofibroblastic tumors
Fibrosarcomatous dermatofibrosarcoma Fibrosarcomatous dermatofibrosarcoma is a variant in which a focal fascicular or ‘herring-bone’ pattern is present.62–64,80 Fibrosarcomatous transformation may occur either de novo or in the recurrence of a typical dermatofibrosarcoma protuberans. These areas are more cellular, show more nuclear atypia and the mean mitotic count is higher than in typical dermatofibrosarcoma (Figs 35.154 and 35.155). Focal loss or less intense staining with CD34 is seen in the fibrosarcomatous areas.86 Fibrosarcomatous dermatofibrosarcoma combined with Bednár may occur.136 A case with formation of giant rosettes and one with a plexiform growth pattern have been reported.137,138
Pigmented dermatofibrosarcoma Pigmented dermatofibrosarcoma (also known as the Bednár tumor or formerly as pigmented storiform neurofibroma) contains dendritic melanocytes and small deposits of melanin pigment within an otherwise typical tumor (Figs 35.156 and 35.157).145–147 The presence of melanocytes within the tumor is puzzling and is probably secondary to colonization. An alternative view proposes neuroectodermal multidirectional differentiation to explain this phenomenon.148
Progression in dermatofibrosarcoma protuberans to the fibrosarcomatous variant appears to be related to microsatellite instability and mutations in TP53 as early and late events respectively.139
In rare cases, areas of a high-grade sarcoma may be found within an otherwise ordinary dermatofibrosarcoma protuberans.140–144 These areas can mimic a myxofibrosarcoma or a pleomorphic malignant fibrous histiocytoma. It is not clear what the prognosis of these tumors is, as the occurrence of this phenomenon is very rare. Interestingly COL1A1-PDGFB fusion transcripts is also detected in sarcomatous areas of the tumor.144
Myxoid dermatofibrosarcoma Myxoid dermatofibrosarcoma is a term used to describe rare cases in which the more typical features may be only focally identifiable because of extensive myxoid degeneration (Figs 35.158–35.160).149–151 Macroscopically, tumors are gelatinous. Thin-walled blood vessels are prominent. Myxoid change may occur in association with any variant of the tumor.152
Dermatofibrosarcoma with areas of giant cell fibroblastoma Dermatofibrosarcoma with areas of giant cell fibroblastoma has already been discussed.
1746 Connective tissue tumors
Dermatofibrosarcoma with myoid nodules
Dermatofibrosarcoma with myoid nodules refers to cases showing areas composed of bundles of eosinophilic SMA-positive spindle, desmin-negative cells indicating myofibroblastic differentiation (Figs 35.161 and 35.162).153,154 Most cases of dermatofibrosarcoma protuberans with myoid nodules have fibrosarcomatous areas.153,154 Small biopsies can cause confusion with myofibroblastic lesions, such as adult myofibroma, but other typical features of dermatofibrosarcoma are usually evident. It has been suggested that the myoid nodules do not represent true myofibroblastic differentiation but rather residual smooth muscle originating from blood vessels destroyed by the tumor.155 However, the bundles of myoid cells are usually positive for actin and negative for desmin and H-caldesmon, suggesting myofibroblastic rather than smooth muscle origin/differentiation.
Flow cytometry studies in dermatofibrosarcoma protuberans often show aneuploidy.156
Differential diagnosis The differential diagnosis includes fibrous histiocytoma, especially its cellular variant, dermatomyofibroma, perineurioma, plaque-like CD34-positive dermal fibroma (medallion-like dermal dendrocyte hamartoma) and neurofibroma (mainly in the superficial part of the tumor). Fibrous histiocytoma tends to be CD34 negative, shows cytological polymorphism, only a
1747 Intermediate (rarely metastasizing) fibroblastic and myofibroblastic tumors
focal storiform pattern and limited superficial infiltration of the subcutis, usually in a radial pattern.157 Epidermal changes (especially hyperplasia) are much more commonly associated with fibrous histiocytoma than with dermatofibrosarcoma protuberans. Cellular fibrous histiocytoma may show positivity for CD34 but this is often in the periphery of the tumor and associated with focal staining for SMA. Plaque-like CD34-positive dermal fibroma (medallion-like dermal dendrocyte hamartoma) has to be distinguished from the plaque stage of dermatofibrosarcoma protuberans.158,159 The former occurs predominantly but not exclusively in children, is a neoplasm of the reticular dermis that tends not to extend to the subcutaneous tissue and consists of CD34-positive fibroblast-like cells with superficial cells oriented perpendicular to the epidermis and deep cells oriented parallel to the epidermis. The superficial part of a dermatofibrosarcoma protuberans may mimic neurofibroma, as the storiform pattern is usually lacking, and this is a particular problem in superficial samples.160 Immunohistochemistry for CD34 and S100 is crucial as the latter is positive for both markers and the former positive for CD34. It has been suggested that there is a small subgroup of indeterminate fibrohistiocytic tumors of the skin in which it is not possible to distinguish accurately between dermatofibrosarcoma protuberans and fibrous histiocytoma because of histologic and immunohistochemical overlap; however, these tumors lack the COL1A1-PDGFB fusion transcript.161,162 Distinction between neurofibroma and the myxoid variant of dermatofibrosarcoma is based on the storiform growth pattern, CD34 expression and S100 protein negative cells in the latter condition.
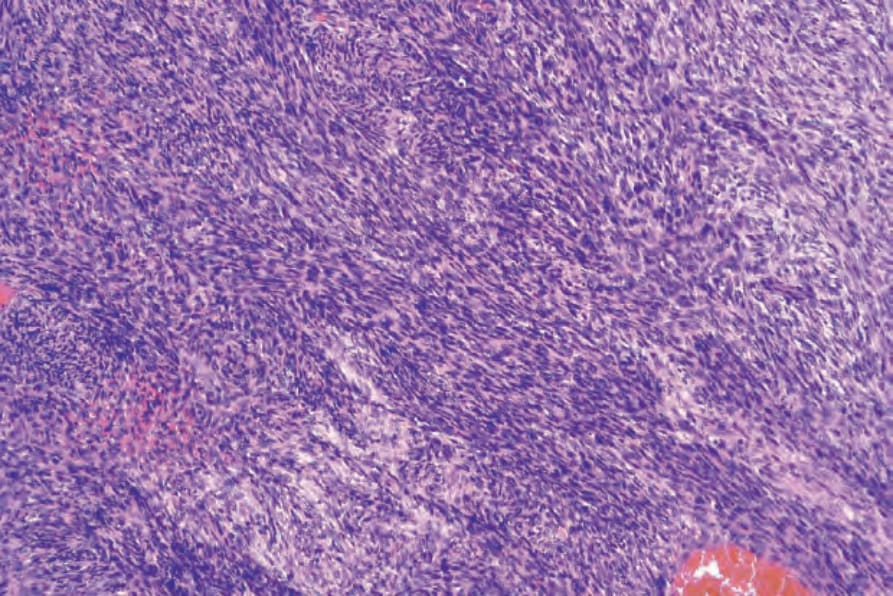
Fig. 35.154 Dermatofibrosarcoma protuberans: this is an example of fibrosarcomatous change. Note the characteristic herringbone pattern.
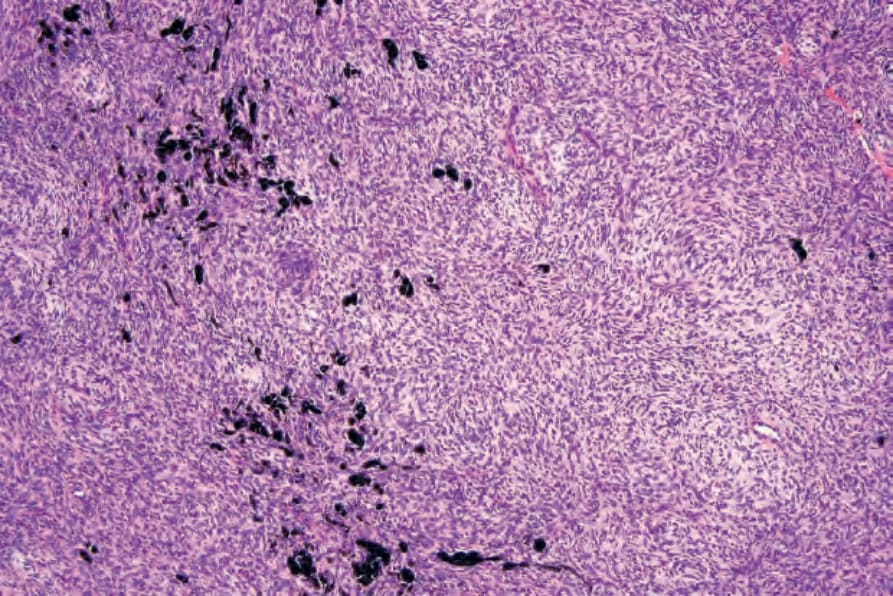
Fig. 35.156 Bednár tumor: except for the foci of pigmented cells, the appearances are identical to those of dermatofibrosarcoma protuberans.
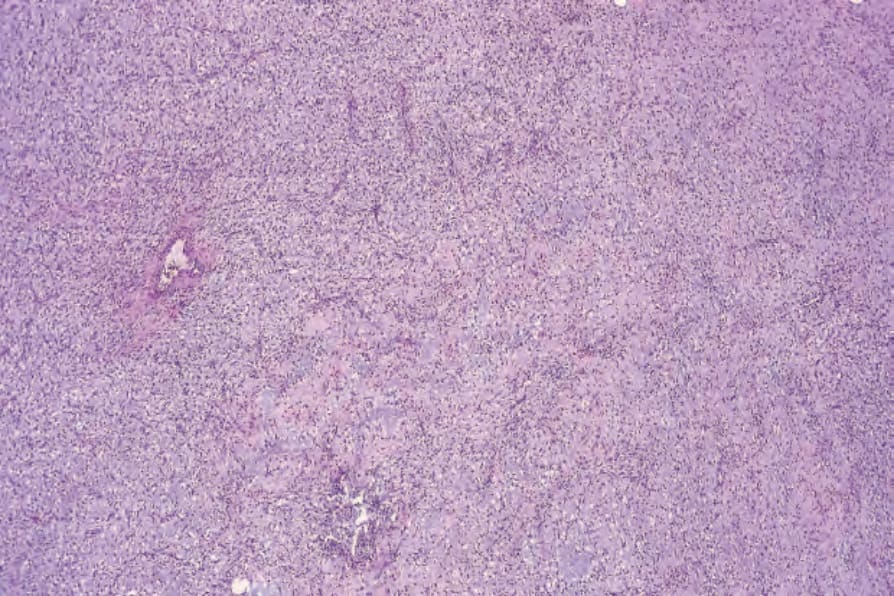
Fig. 35.158 Myxoid dermatofibrosarcoma protuberans: myxoid areas, as seen here, are nondiagnostic and therefore may cause confusion. A careful search should be made for more typical foci.
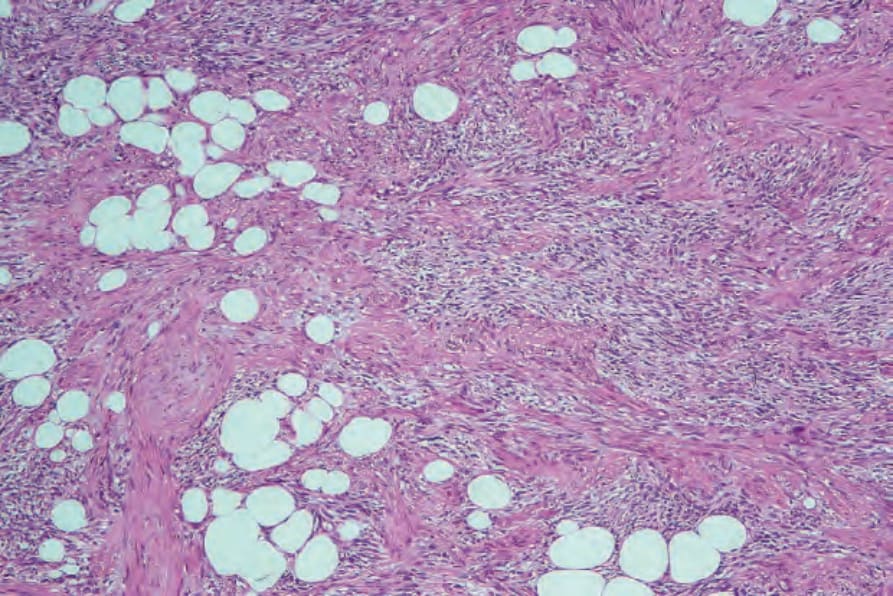
Fig. 35.161 Dermatofibrosarcoma protuberans: some tumors, particularly the fibrosarcomatous variant, contain nodules and bundles of myofibroblasts (the myoid variant).