Penile fibromatosis
Penile fibromatosis
Clinical features Penile fibromatosis (Peyronie disease) is an uncommon fibromatous lesion of the penis that results in pain or curvature on erection.1–3 The etiology is entirely unknown and although it has traditionally been considered to be a form of fibromatosis it appears more likely to represent an unusual fibrotic reaction developing in response to chronic inflammation, veno-occlusive dysfunction, or trauma, maybe in combination with genetic factors.4–7 Veno-occlusive dysfunction has been demonstrated by Doppler studies.4 The prevalence of the disease is higher in diabetic patients and in those with low testosterone levels.4,8 Hypertension and serum lipid abnormalities appear to have an impact in the severity of the symptoms and outcome.9 A case was reported in association with methotrexate therapy.10
Desmoid fibromatosis occurring in children less than 10 years of age is referred to as infantile fibromatosis.11 Most patients with this form of fibromatosis present before the age of 5 and there is predilection for the head and neck, shoulder girdle or thigh.8,12–14 Infiltration of neighboring tissues may be prominent.
Peyronie disease usually presents as either solitary or multiple fibrous plaques adjacent to the corpora cavernosa, most often on the dorsal surface of the shaft. The peak incidence is in the fifth and sixth decades and there is no predilection for any particular racial group. The plaques rarely exceed 2 cm in diameter. The alleged rapidity of onset in many patients probably reflects the severe psychological problems that frequently develop. Spontaneous resolution is rare.
Histologic features The microscopic appearances vary according to the duration of the condition. Early lesions are typified by a vasculitic and chronic inflammatory process in the loose connective tissue between the corpora cavernosa and penile fascia. This leads to an irregular reparative fibrotic process, culminating in the development of dense masses of hyalinized collagen with occasional foci of chronic inflammation (Fig. 35.130). Occasionally, metaplastic ossification may occur. There is no differential diagnosis.
A nonrandom association with gastrointestinal stromal tumor has been reported.15 In addition, an association between desmoid fibromatosis and papillary thyroid carcinomas has been reported.16
Pathogenesis and histologic features Familial adenomatous polyposis patients have germline inactivation of the adenosis polyposis coli gene (APC) which helps mediate the destruction of β-catenin.17–19 The location and type of mutation in FAP appear to affect likelihood of desmoid development.20,21 The tumors develop with loss of heterozygosity at the wild-type allele. Mutations in CTNNB1, the gene encoding β-catenin, are seen in approximately 85 % of sporadic desmoids.22–25 Somatic mutations in APC can also be seen in sporadic cases.26–28 All of these genetic deficits allow unregulated accumulation of β-catenin in the
1739 Intermediate (locally aggressive) fibroblastic and myofibroblastic tumors
nucleus. Cytogenetic anomalies include trisomies of chromosomes 8 and/or 20 and loss of Y and 5q where APC is located.29–32 Overactivation of the Wnt/APC/β-catenin pathway contributes to desmoid development by constitutive activation of pathways in common with fibrosis and scarring.24,33,34 In addition to β-catenin, VEGF overexpression may play a role in progression of sporadic desmoid tumors.35 Although etiologically there is clear evidence to suggest a genetic predisposition, this is probably secondarily influenced by trauma or sex hormones.36 It has been shown that high levels of estrogens can promote, but do not initiate, growth of desmoid tumors. Moreover, it has been suggested that macrophages and microangiogenesis may play a role in the biological behavior.37 AKT1 and BRAF mutations have been found in pediatric cases.38
In children, tumors may show a pattern typical of extra-abdominal fibromatosis or else may show a pattern consisting of more immature round cells in a myxoid background.
Immunohistochemical studies show variable positivity of tumor cells for actin and only rarely and focally for desmin. Demonstration of nuclear accumulation of β-catenin can be helpful, but is not entirely specific (Fig. 35.134).23,39–41
Histologic features are very similar in all subsets of desmoid tumor. Typical cases show a variegated appearance characterized by an admixture of plump spindled cells with rounded or tapering nuclei showing occasional mitotic figures embedded in a variably hyalinized or myxoid collagenous stroma (Figs 35.131–35.133). At the periphery of the lesion, skeletal muscle fibers, subcutaneous fat and fascia are irregularly infiltrated, resulting in bizarre atrophic, degenerative or reactive muscle cell forms. Peripheral collections of chronic inflammatory cells, particularly lymphocytes, are common.
Occasional positivity for keratins and calretinin may lead to diagnostic pitfalls.42 Cytoplasmic, but not nuclear, positivity for WT1 has been described in young type fibromatosis.43 FAP-related lesions are also positive for COX2 and may be positive for cyclin D1 and TP53.44
Ultrastructural studies show cells with features of myofibroblasts and fibroblasts.
Differential diagnosis The differential diagnosis is broad.45,46 The most important differential diagnosis is fibrosarcoma, which shows greater cellularity, nuclear atypia, prominent abnormal mitotic activity, a much lower collagen content and, typically, a herring-bone pattern. Scarring or reactive fibrosis can show virtually identical findings and here history is helpful. Distinction from myofibroblastic tumors including myofibroma is based on the fact that desmoid
1740 Connective tissue tumors
tumor is deep seated and infiltrative and shows β-catenin nuclear staining. Myofibroblastic tumors tend to be negative for the latter marker. CTNNB1 sequencing may be of help in challenging cases.22,23,39,45,46 CTNNB1 and APC genotyping can also aid screening for FAP when desmoid fibromatosis is diagnosed in children.47
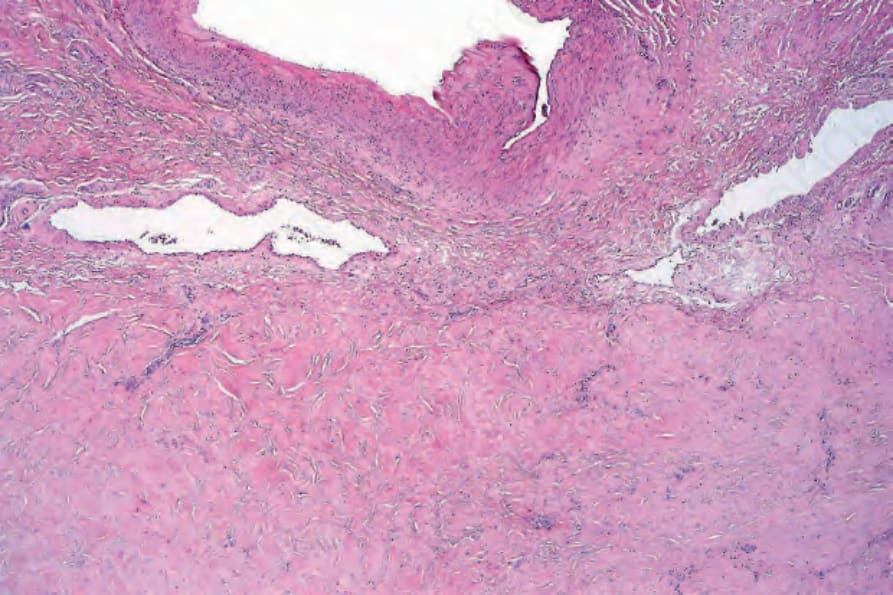
Fig. 35.130 Penile fibromatosis: biopsy from end-stage disease showing dense collagen without any significant inflammation. Despite its name, the condition most probably represents a reactive process.
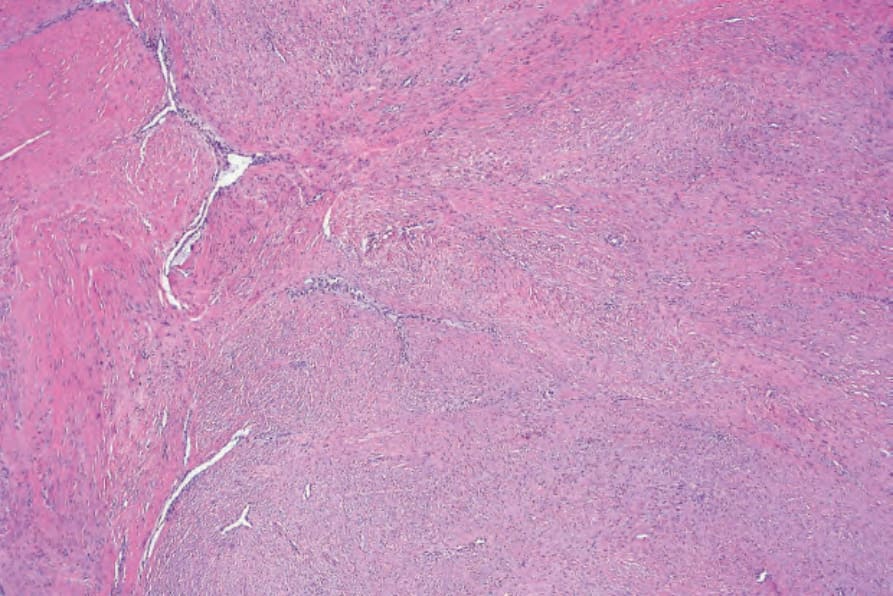
Fig. 35.131 Desmoid fibromatosis: low-power view showing cellular bundles with focal collagen deposition.
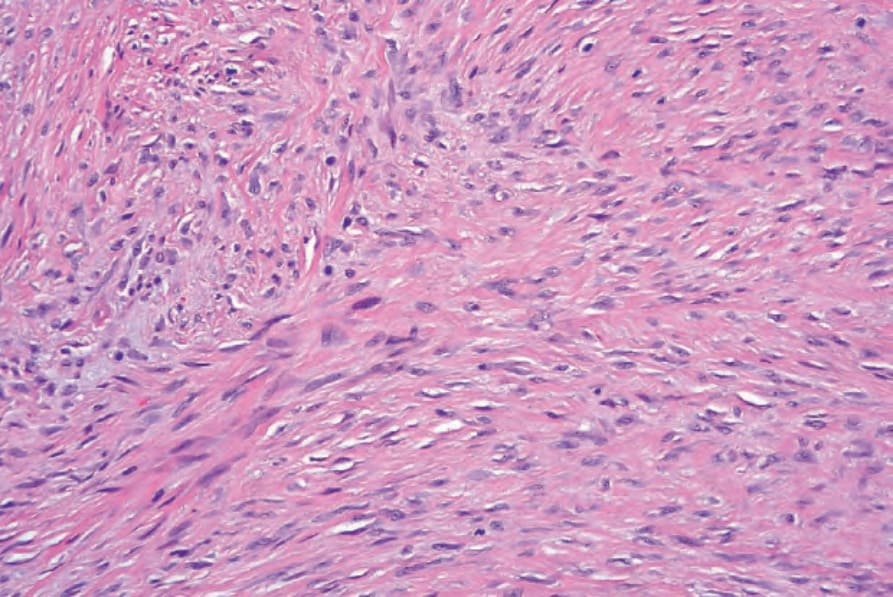
Fig. 35.132 Desmoid fibromatosis: the tumor is composed of spindled cells with a variable admixture of collagen.
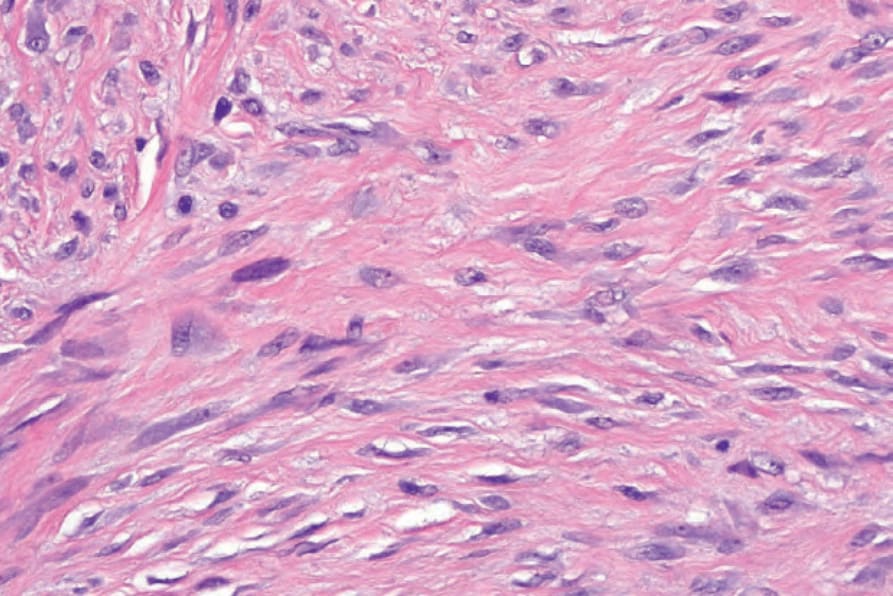
Fig. 35.133 Desmoid fibromatosis: the spindled cells have vesicular nuclei with small nucleoli. Mitoses are commonly present.
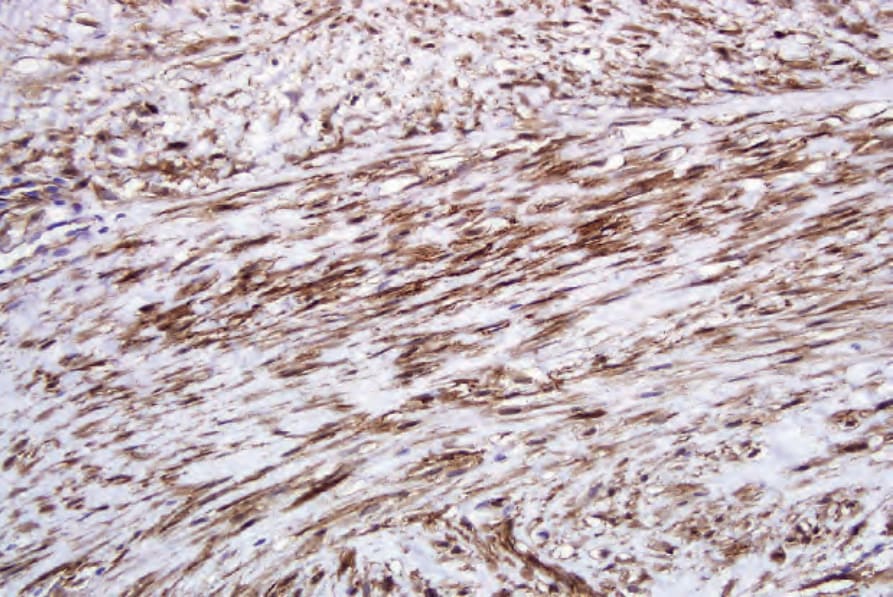
Fig. 35.134 Desmoid fibromatosis: the spindled cells are beta-catenin positive.