Palmar fibromatosis
Palmar fibromatosis
protein binds laminin and collagen type IV and alterations in the protein result in abnormalities in the assembly of basement membrane material with the typical manifestations of the disease. Interestingly, ANTXR2 also serves as a receptor for anthrax toxin.36 Infantile systemic hyalinosis has similar disease manifestations and ANTXR2 mutations and it likely represents a disease spectrum with juvenile hyaline fibromatosis. The name of hyaline fibromatosis syndrome has been proposed to include both entitites.37–43
Clinical features Palmar fibromatosis (Dupuytren contracture) is a common condition that is largely confined to adults; its incidence increases with age.1–6 Presentation in children is rare and occasional congenital cases may occur.7,8 Males are affected more often than females and up to 4% of the adult male population, particularly the elderly, are thought to develop this lesion.9 People of northern European descent are predominantly affected and women usually develop the disease much later in life than men.10,11 The disease is much less common in Oriental Jews.12 In contrast to keloid, Dupuytren contracture is comparatively uncommon in the dark-skinned races, but the incidence is increased in patients with plantar fibromatosis and knuckle pads. An association with diabetes and with Peyronie disease has also been documented.13,14 Traditionally, the disease has been associated with alcoholism and epilepsy but this has not been substantiated in recent studies.13,15 Bilateral involvement is common, but is usually asynchronous. There is an increased familial incidence, but no evidence of any relationship to either occupation or trauma.16
The tumors are largely composed of irregular poorly circumscribed masses of deeply eosinophilic, hyalinized, collagen-like material within which are embedded a variable (though usually small) number of fairly plump spindled cells (Figs 35.123–35.125). Hyalinization is rarely not prominent.44 Scattered macrophages and multinucleated giant cells may also be seen.25 Basophilic calcospherules have been documented.44
Electron microscopy shows mesenchymal cells with dilated rough endoplasmic reticulum, prominent Golgi complexes and vesicles with abundant fibrillogranular material.45
Differential diagnosis The presence of multiple lesions arising in childhood and the characteristic histologic features narrow down the differential diagnosis. Infantile
Typically, palmar fibromatosis begins as firm nodules in the distal palmar aponeurosis and culminates in disabling flexion at the metacarpophalangeal joints, especially in the ring finger, giving rise to a claw-like deformity and puckering of the palmar skin. Involvement of the wrist and of the interphalangeal joints is very rare.17,18 Local recurrence is very common unless radical excision of the palmar fascia is performed.9
Pathogenesis and histologic features The etiology is unknown. Although trauma has been suggested as an important factor, this has not been substantiated in a large study.19 Array comparative genomic hybridization has shown no gene copy number changes.20 Indinavir treatment in human immunodeficiency virus (HIV)-positive patients has been linked to the development of Dupuytren contracture.21
1737 Intermediate (locally aggressive) fibroblastic and myofibroblastic tumors
With the passage of time, maturation of the fibrous tissue leads to late lesions characterized by large amounts of hypocellular, hyalinized collagen (Fig. 35.128). Scattered chronic inflammatory cells may be present at the periphery of the tumor, but there is no evidence of an active inflammatory process. Hemosiderin is uniformly absent, militating against a traumatic etiology. By immunohistochemistry, variable positivity for smooth muscle actin is seen, as expected in a myofibroblastic lesion. Desmin may be focally positive. Lesional cells are negative for CD34 and h-caldesmon. Nuclear β-catenin positivity is usually absent in superficial fibromatoses. However, occasional focal positivity may be seen. P16 is usually positive and estrogen receptor is expressed in many cases.
The degree of cellularity appears to correlate with the risk of local recurrence.33
TGF-β1, a multifunctional cytokine that plays a central role in wound healing, fibrosis and collagen deposition, is implicated in the pathogenesis of the disease.22 While β-catenin is overexpressed, mutations in the encoding gene CTNNB1 which are common in desmoid fibromatosis are not seen in palmar fibromatosis.23–29 Overexpression of β-catenin does not seem to be related to risk of recurrence.30 Periostin, an extracellular matrix protein, may have a role in the pathogenesis of the disease by inducing proliferation, contraction and apoptosis of fibroblasts.31
Differential diagnosis The only lesion that requires exclusion in the differential diagnosis is desmoid fibromatosis, which rarely occurs in the hand, is more uniformly cellular and tends to be deeper. Moreover, diffuse nuclear β-catenin positivity, although not specific for desmoid fibromatosis, is usually seen in the latter and not in palmar fibromatosis.
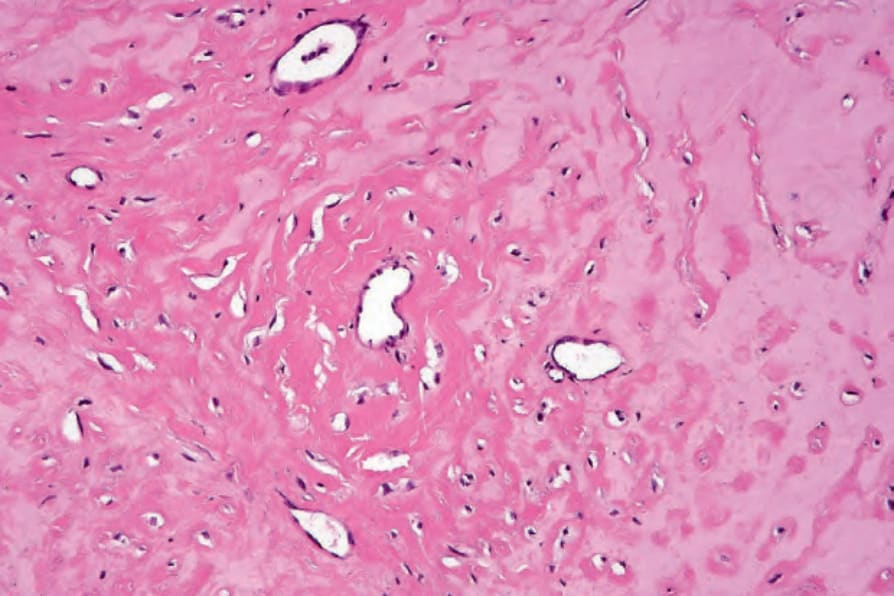
Fig. 35.123 Juvenile hyaline fibromatosis: this field is largely acellular and composed of intensely eosinophilic, hyalinized material. By courtesy of J. Sciubba, DDS, Baltimore, USA.
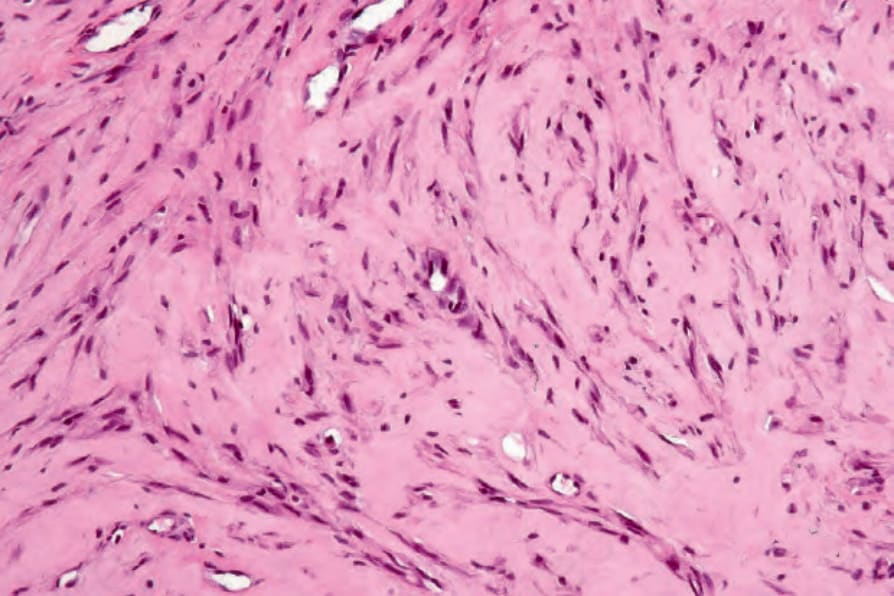
Fig. 35.124 Juvenile hyaline fibromatosis: other areas may be more cellular. By courtesy of J. Sciubba, DDS, Baltimore, USA.
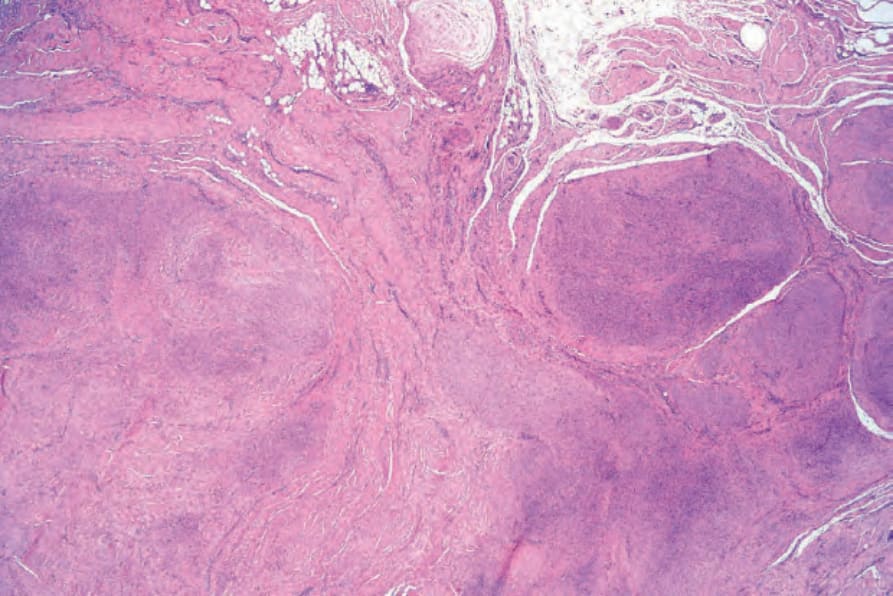
Fig. 35.126 Palmar fibromatosis: scanning view showing multiple nodules of hypercellular tissue with admixed hyalinized collagen.
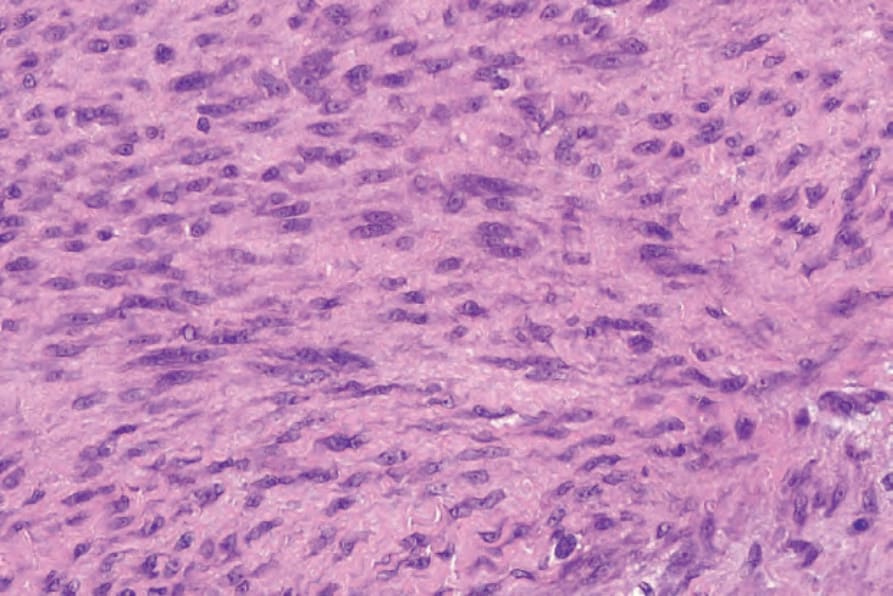
Fig. 35.127 Palmar fibromatosis: the lesion is composed of spindled cells with elongated vesicular nuclei containing small central nucleoli. Occasional normal mitotic figures are typical in early lesions.
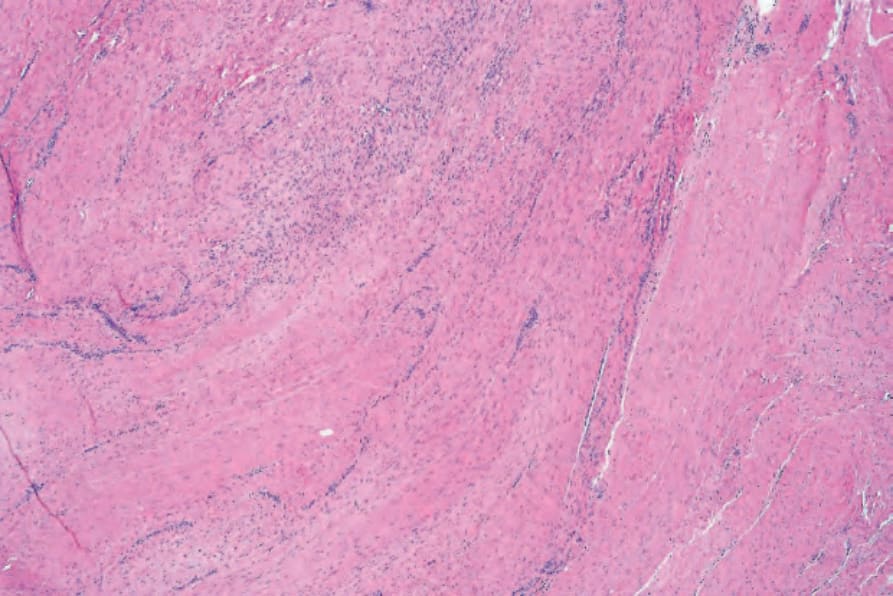
Fig. 35.128 Palmar fibromatosis: older lesions are characteristically hypocellular and consist largely of broad bundles of hyalinized collagen.