Calcifying aponeurotic fibroma
Calcifying aponeurotic fibroma
Clinical features Calcifying aponeurotic fibroma (also known as juvenile aponeurotic fibroma) is a very rare lesion seen predominantly in the first two decades of life, with a predilection for males.1–3 It presents as a single small nodular or infiltrative mass, most often on the feet or hands, especially the palms. Involvement of other sites such as the head and neck, back, abdominal wall, legs and arms is very rare.4,5 Multiple lesions are exceptional.6 Bone involvement is extremely rare.7 Local recurrence, particularly in younger patients, is common and occurs in up to 50% of cases.
Histologic features An FN1-EGF gene fusion, not detected so far in any other neoplasm, has been reported as the main driver mutation in this tumor.8
1731 Benign fibrous and myofibroblastic tumors and tumorlike lesions
Calcifying aponeurotic fibroma characteristically forms an irregular mass of dense, fairly cellular, fibrous tissue invading subcutaneous and muscular structures widely (Fig. 35.107). Myofibroblasts tend to be plump with prominent nuclei. Usually, these cells have a linear or palisaded arrangement and comprise the bulk of the tumor. As the lesion matures, the calcified areas undergo chondroid metaplasia (Fig. 35.108). Extramedullary hematopoiesis may occasionally be seen.9
attention of either clinicians or pathologists.1–3 They present as fairly ill-defined foci of fibrous thickening over the metacarpophalangeal or proximal interphalangeal joints, most often in the middle aged (Fig. 35.109).4–6 They may be familial, associated with Dupuytren contracture or plantar fibromatosis, secondary to repeated trauma or idiopathic. They are almost always asymptomatic. Knuckle pad-like lesions occur in epidermolytic palmoplantar keratoderma associated with mutations on keratin 9.7–9 A case of knuckle pads with leukonychia and deafness has been documented.10 An exceptional association with pseudoxanthoma elasticum is probably coincidental.11
Differential diagnosis The differential diagnosis includes palmar fibromatosis, which is rare in young people and tends to be fairly circumscribed, and soft tissue chondroma, which lacks the dense myofibroblastic component and is composed solely of cartilaginous tissue, which is often rather cellular.
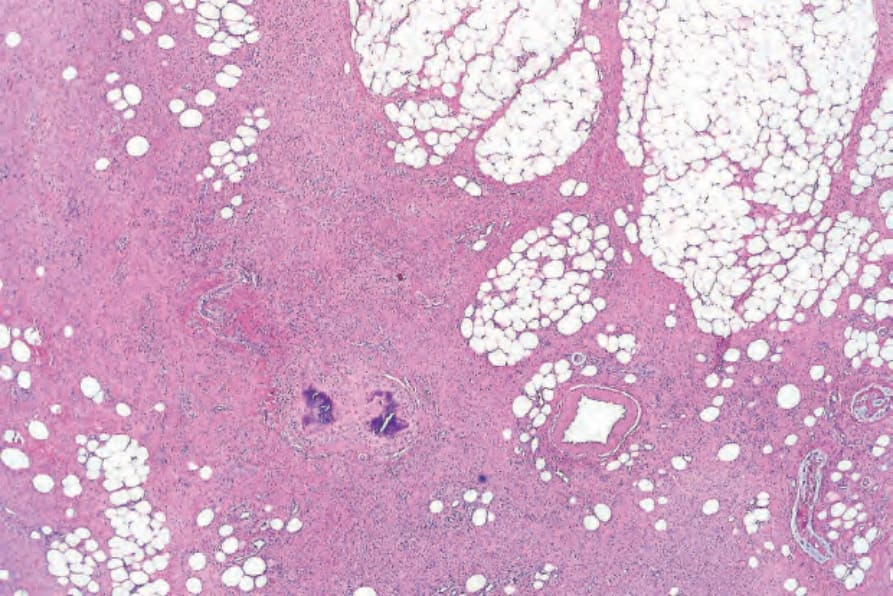
Fig. 35.107 Calcifying aponeurotic fibroma: an irregular infiltrative mass of fibroblastic tissue is present in the subcutaneous fat.
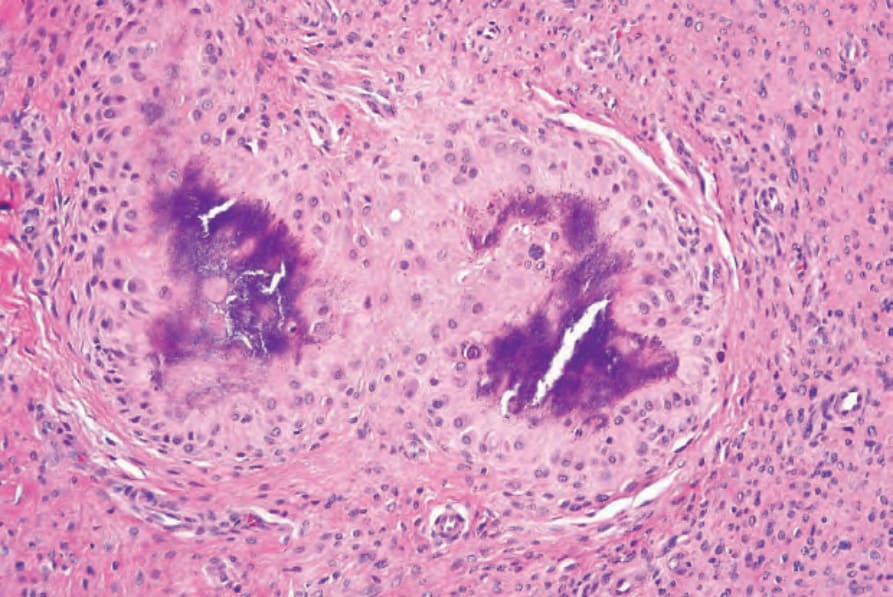
Fig. 35.108 Calcifying aponeurotic fibroma: in this section, there is chondroid metaplasia and there is focal basophilic calcification.

Fig. 35.109 Knuckle pad: typical thickened plaques are present over the interphalangeal joints and second metacarpophalangeal joint. By courtesy of M.M. Black, MD, Institute of Dermatology, London, UK.
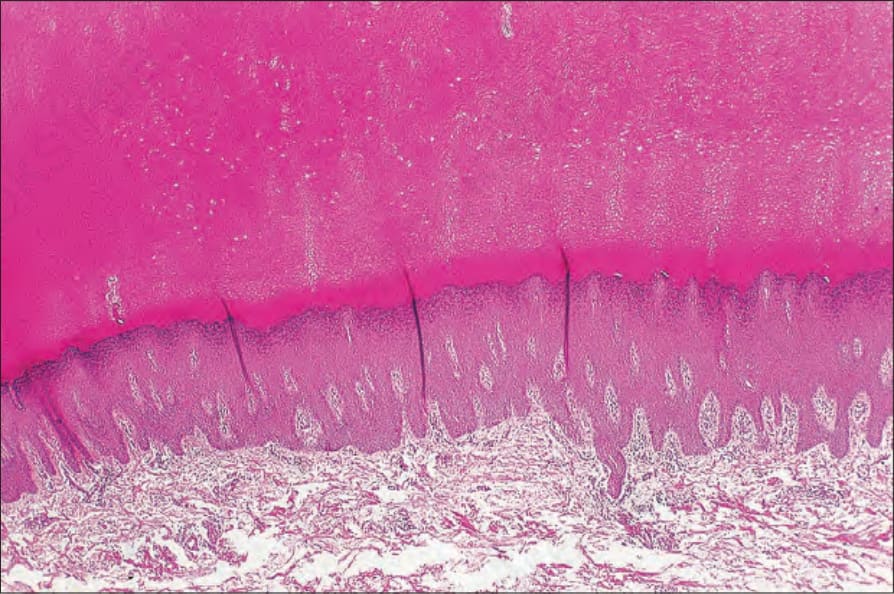
Fig. 35.110 Knuckle pad: in this section there is massive hyperkeratosis and acanthosis. The appearances are non-specific.