Inclusion body fibromatosis
Inclusion body fibromatosis
Clinical features
Inclusion body fibromatosis is a rare benign neoplasm initially described as infantile digital fibromatosis. The latter term derives from the fact that almost all cases arise on the fingers or toes of infants less than 3 years of age, and one-third of the cases are congenital.1–7 However, rare cases have been reported in older children and in adults and at other sites, and a more accurate designation is that of inclusion body fibromatosis.8–12 Typically, it presents as a small (usually less than 1 cm diameter), rapidly growing, dermal or subcutaneous nodule on the dorsal or lateral aspect of one of the digits; multiple lesions arising synchronously or separately on more than one digit (fingers and toes) are not uncommon. Lesions may also be seen elsewhere on the hands and feet.7 Inclusion digital fibromatosis shows a marked tendency towards local recurrence after excision (up to 50%), but has no capacity to metastasize. Spontaneous regression is usually seen in most cases and therefore treatment should only be symptomatic.
Histologic features The lesion is composed predominantly of an irregular mass of proliferating myofibroblasts, showing occasional normal mitoses, but no atypia, embedded in a dense collagenous stroma, which extends deeply from the dermis and may be attached to underlying osteoarticular structures (Fig. 35.104). The diagnostic sine qua non and characteristic feature is the presence of brightly eosinophilic intracytoplasmic inclusions in a variable number of the myofibroblasts (Figs 35.105 and 35.106) which can be seen as red inclusions with a Masson trichrome stain. A focal lymphocytic inflammatory cell infiltrate can be seen and it has been reported to be more common in areas with numerous inclusion bodies.13 Tumor cells are usually positive for alpha smooth-muscle actin, calponin, and desmin.7 Occasionally, they may be positive for h-caldesmon and beta-catenin (nuclear staining).7 These inclusions are actin positive, especially in alcohol-fixed tissue, and the presence of these filaments has been demonstrated by immunoelectron microscopy.14,15 The inclusions can also be highlighted with anti-calponin 1.16 Positivity for actin may also be demonstrated if sections are pretreated with KOH.17 The inclusions are composed of intermediate filaments measuring 5–7 nm. It is not clear why these inclusions are formed. It is very likely that they are the result of a defect in actin metabolism.18 Other myofibroblastic lesions (including myofibrosarcoma), the stromal cells of phyllodes tumor, fibroadenoma, and some leiomyomas can rarely show similar actin-positive intracytoplasmic inclusions.19–24
Differential diagnosis The presence of eosinophilic inclusions and the clinical history allow no differential diagnosis. Identical lesions may occur in the digits of patients with a syndrome consisting of terminal osseous dysplasia and pigmentary defects.25,26 However, in these patients, inclusions are not seen.
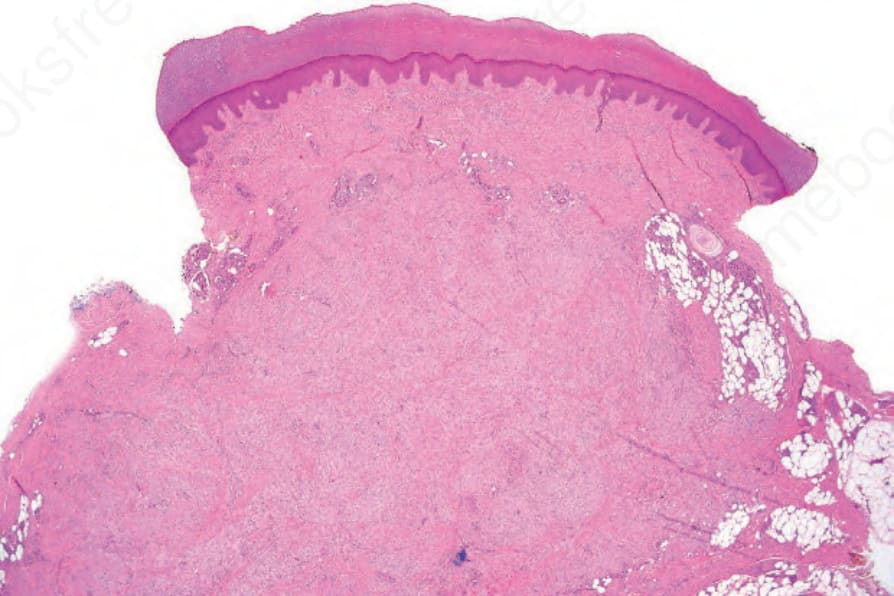
Fig. 35.104 Inclusion body fibromatosis: the tumor is composed of bland spindled cells with a collagenous stroma.
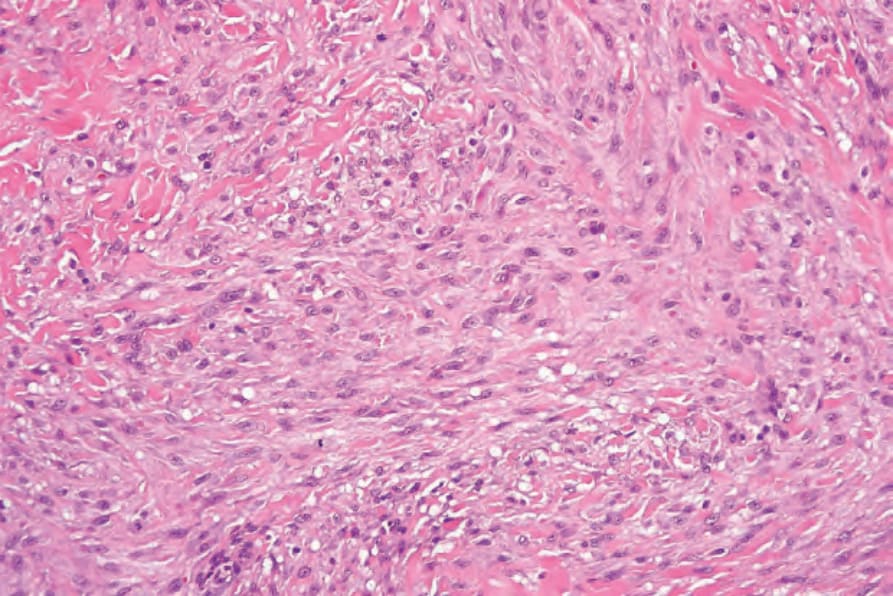
Fig. 35.105 Inclusion body fibromatosis: the spindled cells have uniform vesicular nuclei with small nucleoli.
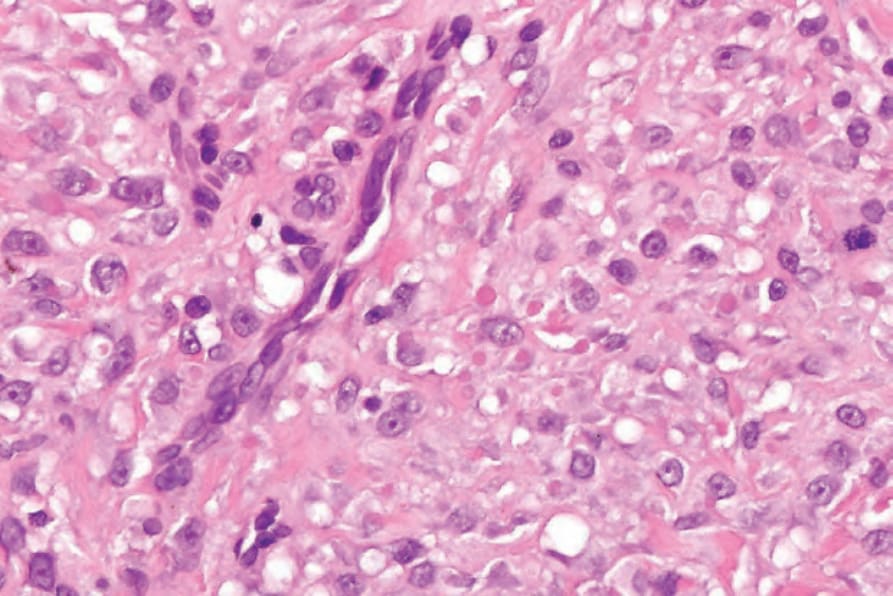
Fig. 35.106 Inclusion body fibromatosis: in this example, there are numerous inclusions.